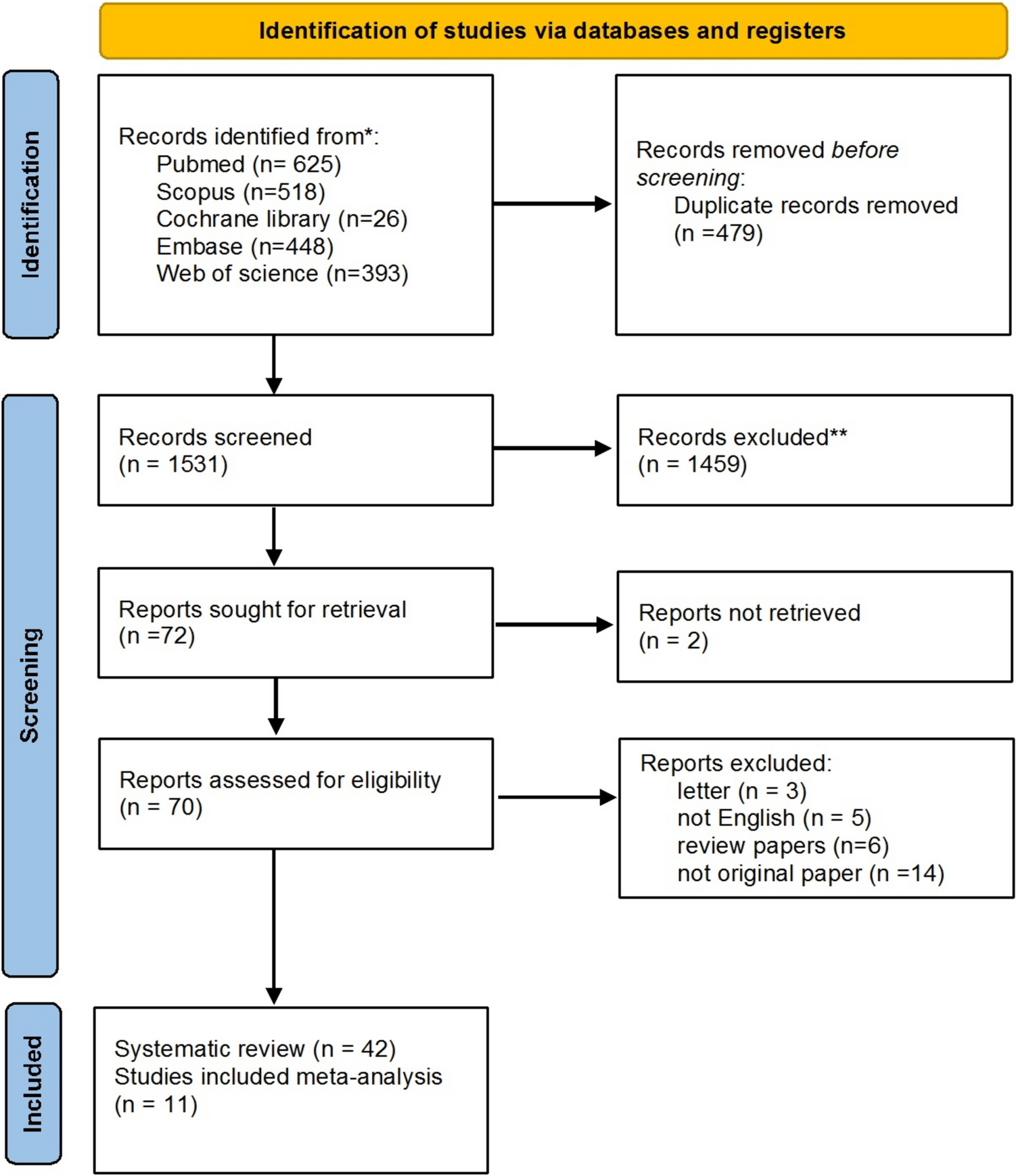
In recent years, significant advancements in endovascular techniques have transformed the landscape of treatment options for patients with posterior communicating artery aneurysms [56, 57]. These improvements have led to increased interest in whether endovascular approaches could offer benefits comparable to or even better than traditional microsurgery; this was especially novel, considering the preference for less invasive procedures by patients and physicians. Our study compared microsurgery and EVT outcomes of PComA aneurysms presenting with ONP. Specifically, we assessed the time course of favorable recovery rates of ONP following treatment. According to the meta-analysis of follow-up results, microsurgery was associated with higher rates of favorable ONP recovery outcomes at 1, 3, 6, and 12-month follow-ups. Notably, after 12 months, comparable recovery outcomes were identified. In a subgroup analysis of early treatment window patients, comparable recovery was achieved earlier at 6 months follow-up. Microsurgery had higher rates of favorable ONP recovery compared to EVT in < 60-year-old patients, large aneurysms (≥ 7 mm), ≥ 7 days of ONP symptoms, and in cases of total ONP. Among ruptured aneurysms, partial ONP, small aneurysms, ≥ 60-year-old patients, and with early treatment, favorable ONP recovery outcomes of microsurgery and EVT were comparable.
Timecourse of ONP recovery outcomes
Understanding the detailed timelines of oculomotor nerve palsy (ONP) recovery, both in the short and the long term, is essential for clinical decision-making and patient counseling, as the timing of recovery can significantly impact a patient’s quality of life and functional outcomes [44]. This study addresses this gap by offering an updated analysis that specifically examines the recovery trajectories following both microsurgical and endovascular interventions. Other meta-analysis studies, with less than 12 months follow-up duration, found lower overall recovery rates, and significantly higher ONP recovery rates associated with microsurgery compared to EVT [5, 43], which is consistent with the findings in our study. However, in this present meta-analysis, increasingly favorable ONP recovery was achieved with a longer duration of follow-up; this would presumably enable fibrosis and shrinkage of the treated aneurysm [6]. The meta-analysis revealed distinct recovery patterns for microsurgery and EVT over time. Microsurgery remains a well-established treatment modality for alleviating ONP symptoms, demonstrating high efficacy in achieving immediate symptom resolution. However, recent evidence indicates that EVT may also contribute to favorable outcomes in ONP management. Although the immediate postoperative recovery rates of EVT are comparatively modest, there is a notable, steady increase in recovery proportions observed over time. This suggests that EVT facilitates a gradual improvement in ONP symptoms, potentially leading to substantial recovery over time. Importantly, our study found that early intervention with EVT may accelerate this recovery process, highlighting its potential role as a viable alternative to traditional surgical methods, particularly in cases where microsurgery is not feasible or poses higher risks, or in cases of patients and physician preferences of less invasive intervention.
In the short term, microsurgery is traditionally preferred, as it effectively eliminates the compressive damage of the aneurysm to the oculomotor nerve; this alleviates the symptoms promptly, and stops the ongoing repetitive injury of arterial pulsation [5, 45, 46]. Of note, detailed surgical technique data is lacking as to whether or not the aneurysms were being needle punctured following clip application.
Although there are concerns with EVT, such as the contribution to mass effect with coiling, recent studies report remarkably high rates of complete nerve recovery (50–85%) with EVT [9, 14, 23, 27, 49]. EVT may not result in a quicker favorable recovery of ONP, but in long-term follow up, it will ultimately lead to a similar ONP recovery rate as microsurgery. This can be attributed to the elimination of pulsation and the long-term shrinking of the treated aneurysm leading to advantages beyond immediate relief [25].
These findings suggest that treatment decisions should be personalized, taking into account both short-term and long-term outcomes to weigh the risks and benefits for each individual.
Early versus delayed window treatment
A crucial factor influencing ONP recovery time from is the duration of symptoms prior to treatment. Research indicates, consistent with our findings, that a shorter symptom duration—defined as 14 days or less—prior to intervention significantly enhances the likelihood of complete recovery [17, 23], highlighting the importance of prompt management. Signorelli et al. conducted a multicenter cohort study of patients with unruptured PComA aneurysms and found that the key predictor of ONP recovery was timely, complete, and durable aneurysm exclusion, irrespective of the treatment approach employed [29]. These findings align with our study, which demonstrates that patients receiving early treatment have a three-fold increased odds of achieving complete recovery compared to those treated later. Moreover, early intervention not only improves the likelihood of complete recovery, but also accelerates the time course of recovery. In this subgroup, ONP early recovery rates are comparable between surgical and endovascular interventions, surpassing the outcomes observed in the main meta-analysis and those treated during the delayed window. However, in both early and delayed treatment windows, microsurgery remains superior to endovascular therapy in terms of ONP recovery outcomes.
Factors influencing treatment outcomes: considerations for optimal decision-making
It is crucial to note that these findings can be better interpreted if various major factors influencing treatment outcomes are considered, when viewed in the context of our meta-analysis and systematic reviews of the literature. As it seems to rapidly relieve the compressive effect [5,6,7,8, 47], microsurgery is the optimal treatment for patients with larger PComA aneurysms that may induce a stronger mass effect- the predominant cause of total ONP- [1, 5] as well as in cases of prolonged ONP symptoms that suggest severe nerve damage. Such factors related to nerve injury appear to play a stronger role in recovery [17]. A longer follow-up time is thus necessary for patients with a longer history of ONP or total ONP at presentation, as full recovery may take up to 2 years after microsurgery [3]. However, this has not been explored in EVT.
EVT of PComA aneurysms can also relieve ONP by eliminating the pulsation effect in the short term, yielding comparable recovery rates in cases with less severe mass effect; this may include cases such as partial palsy with reversible nerve damage, small PComA aneurysms, and shorter time from ONP onset to treatment [2, 6]. To address the inconsistency in partial ONP evaluation, future research could implement more efficient and accurate measures to better explore nerve injury extent and optimize outcomes for both treatments modalities. On the other hand, the correlation between aneurysm size and risk of developing ONP [47] has been questioned because this complication can occur also in the context of very small aneurysms [58]. Thus, our meta-analysis concluded that aneurysm size cannot be considered a predictive factor for ONP recovery. However, in small aneurysms ≤ 7 mm, EVT could yield comparable results to microsurgery.
In ruptured cases, the irritative effects of subarachnoid blood and its resultant inflammation may also contribute to nerve damage resulting in ONP, as opposed to unruptured cases where preexisting mass effect is the sole cause of ONP [3, 15, 37]. These patients tend to show early recovery from ONP due to the prompt attention they receive, leading to earlier treatment. Moreover, both microsurgery and EVT offer protection against rebleeding [4, 5, 7, 37, 45]. However, microsurgery removes surrounding blood immediately [5, 7].
EVT could specifically be preferable for patients ≥ 60 years old and ineligible for microsurgery by effectively reducing potential complications and promoting the recovery of nerve function [46, 59]. Few studies reported complication rates of each treatment modality [11, 18, 19, 24, 25, 34, 46]. Overall, the rate of complications is low, and neither confers a benefit over the other by complication rate alone.
While EVT and microsurgery have been generally studied, the comparison of their effects on ONP recovery within specific subgroups remains underexplored. This gap highlights the need for targeted research to better understand how these factors influence recovery outcomes across different treatment modalities.
Limitations
With a large sample size, our meta-analysis represents a pioneering effort, underscoring the significance of incorporating timing and follow-up in the assessment of treatment efficacy and identifying key factors influencing recovery. Nonetheless, the present study has several limitations. First, the methodologic quality of the included studies along with the variables and outcome measures were not constant. Our results were also associated with the possibility of publication bias. Second, the advancement of surgical [5, 12, 45] and endovascular [4, 23, 27] techniques necessitates further investigation to optimize therapeutic strategies. Our analysis found that the broad classification of “EVT” lacked granularity to assess outcome differences between primary coiling, stent-assisted coiling, and flow diversion. Most studies reported coiling without specifying stent usage, and flow diversion was infrequently detailed, precluding a robust analysis of technique-specific outcomes. Third, because all the included studies are retrospective and non-comparative, meaningful direct comparisons are limited. Finally, data on important factors such as anatomical variations, morphological-hemodynamic patterns (wall shear stress [31], aneurysmal direction [23, 36], and the distance between the internal carotid artery and the anterior–posterior clinoid process [48]) and anti-inflammatory medications [23] were not available and thus, we were unable to control for them. Additionally, our study lacked a comparison of subgroups over time. We did not have sufficient data to analyze these timepoints accurately. Future prospective studies should validate the clinical impact of various surgical approaches, intrasaccular and extrasaccular endovascular techniques, and account for different impacting factors.

Comments (0)