
Remember me


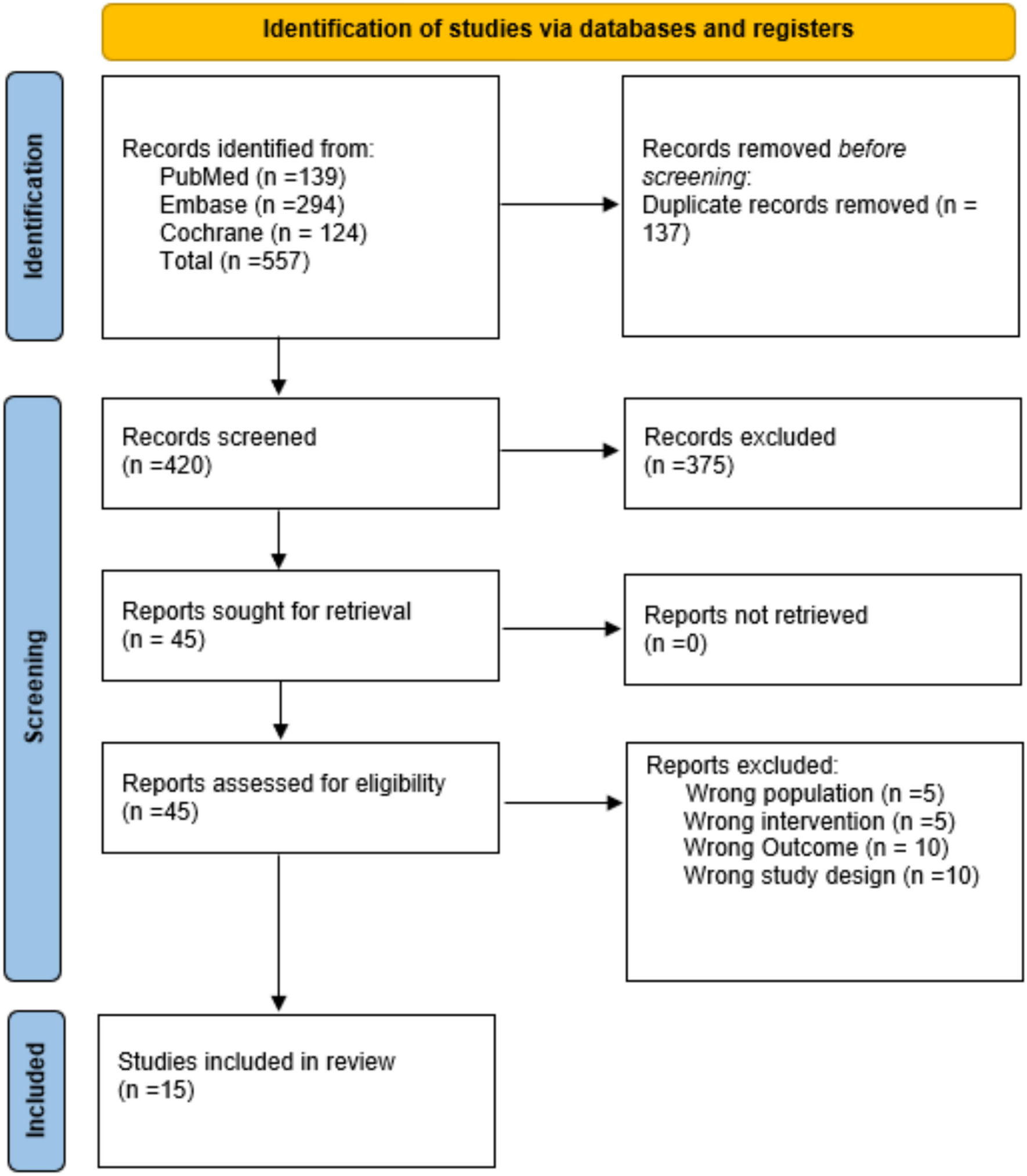
Figure 1 is the flowchart of the systematic review. A total of 554 references were identified, of which 518, after reviewing the title and the abstract, were discarded as not pertinent.
Of 36 potentially relevant papers, we excluded 21 papers for the following reasons: uncertainty whether GBS was related to COVID-19 disease or vaccination (n = 1), GBS not related to a vaccine (n = 2), not sufficient data (n = 2), missing data on total COVID-19 vaccine doses (n = 7), possible overlapping patients (n = 9).
Overall, 15 studies were included [25,26,27,28,29,30,31,32,33,34,35,36,37,38,39]. The meta-analysis only deals with adeno-vectored and mRNA vaccines since very few data are available for other vaccine technologies.
GBS incidence per COVID-19 vaccine doses administered regardless of the vaccine technologyWe included 17 cohorts from 13 studies, collecting 1450 GBS cases over a total of 1,058,927,070 administered vaccine doses. The random-effects model yielded 1.25 GBS cases per million vaccine doses (95%CI 0.21; 2.83) (Fig. 2). The prediction interval yielded a range of 0 to 9.6 cases per million vaccine doses. Regional subgroup analyses showed for Asian countries 1.53 GBS cases per million vaccine doses (95%CI 0.00; 11.08), and for European countries 1.81 GBS cases per million vaccine doses (95%CI 1.08; 2.71) (SI).
Fig. 2
Forest plot of GBS incidence with respect to COVID-19 vaccine doses administered regardless of the vaccine technology. Events: number of GBS cases; Total: number of vaccine doses
Risk ratio after first and second vaccination doseWe included five cohorts in the analysis of risk between GBS cases after the first and second doses of COVID-19 vaccination. We excluded vaccines that required only one vaccine dose (e.g., Jcovden). The MH method yielded an RR of 2.60 (95%CI 0.42, 15.92) for the first dose (Fig. 3).
Fig. 3
Forest plot about risk ratio between GBS cases linked to first and second doses of COVID-19 vaccine. Events: number of GBS cases; Total: number vaccine doses
GBS incidence per COVID-19 vaccine technologyFor adenoviral-vectored vaccines, we included 11 cohorts from 7 studies, collecting 806 GBS cases over a total of 127,355,745 vaccine doses. The random-effect model yielded 3.93 (95%CI 2.54; 5.54) GBS cases per million doses of adenovirus-based COVID-19 vaccine (Fig. 4A). More specifically, for Vaxzevria the random-effect model proportion was 2.23 GBS cases every million doses (95%CI 0.00, 7.88). For Jcovden the random-effect model proportion was 6.63 for every million doses (95%CI 4.75, 8.80) (SI, Section 2).
Fig. 4
Forest plot of GBS incidence with respect to A adenoviral-vectored COVID-19 vaccine doses administered, and B with respect to mRNA-based COVID-19 vaccine doses administered. Events: number of GBS cases; Total: number of A adenoviral-vectored or B mRNA-based vaccine doses
For mRNA vaccines, we included 14 cohorts from 8 studies, collecting 534 GBS cases over a total of 823,793,743 vaccine doses. The random-effect model proportion yielded 0.69 (95%CI 0.38; 1.06) GBS cases per million doses of mRNA-based COVID-19 vaccine with a prediction interval from 0.00 to 2.18 (Fig. 4B).
Specifically, for Comirnaty the random-effect model proportion was 0.64 GBS cases every million doses (95%CI 0.12, 1.45), and for Spikevax the random-effect model proportion was 0.66 every million doses (95%CI 0.27, 1.21) with a prediction interval between 0.0 and 2.6 (SI, Section 2).
Risk ratio between observed and expected GBS cases after COVID-19 vaccinationWe included 15 cohorts from 5 studies in the analysis of risk between observed and expected GBS cases after COVID-19 vaccination regardless of the vaccine employed. The quantification method for expected cases for each study is summarised in SI. We identified 1690 observed and 2190 expected GBS cases over a total of 706,234,418 vaccine doses. The MH method yielded an RR of 1.09 (95%CI 0.68; 0.90) (Fig. 5).
Fig. 5
Forest plots of risk ratio between observed and expected GBS linked to COVID-19 vaccine doses administered regardless the vaccine technology; B with respect to vector-based vaccines; C with respect to mRNA vaccines. For vaccinated, Events: number of GBS cases; Total: number of vaccine doses. For expected, Events: number of expected GBS cases; Total: number of subjects in the population considered. AdV: adenoviral-vectored vaccines
Regarding GBS after adenovirus-based vaccination, we included ten cohorts from 5 studies. The MH method yielded an RR of 2.37 (95%CI 1.67, 3.36) (Fig. 6A). For GBS after mRNA-based vaccination, we included nine cohorts. The MH method yielded an RR of 0.32 (95%CI 0.23, 0.47) (Fig. 6B).
Fig. 6
Forest plot about risk ratio between GBS cases linked to COVID-19 vaccine doses administered; A with respect to adenoviral-vectored vaccines; B with respect to mRNA vaccines. For vaccinated, Events: number of GBS cases; Total: number of vaccine doses. For expected, Events: number of expected GBS cases; Total: number of subjects in the population considered
GBS mortality per COVID-19 vaccine doses administered and among GBS casesWe included six cohort studies in the analysis of mortality among people who developed GBS after being vaccinated against COVID-19 regardless of the vaccine technology. We identified 28 deaths in 524 GBS cases for a total of 696,978,860 vaccine doses. The random-effect model proportion yielded 0.10 deaths with GBS per million doses of COVID-19 vaccine (95%CI 0.00; 0.75) (Fig. 7A). Considering the mortality among GBS the random-effect model proportion yielded 4.6 deaths for every 100 GBS cases after COVID-19 vaccination (95%CI 1.23, 5.45) (Fig. 7B).
Fig. 7
Forest plots of GBS mortality after COVID-19 vaccination. A with respect to administered doses; B with respect to GBS cases after vaccination. Events: number of deaths; Total: number of total COVID-19 vaccine doses (A) and GBS cases (B)
Assessment of study quality, publication bias, heterogeneity, and sensitivity analysesThe overall quality of the included studies was deemed high (SI, Table S2). Assessment of funnel plot asymmetry with visual inspection and Egger’s and Peter’s test showed potential asymmetry for the following analyses: all vaccine technologies and adenoviral-vectored incidence, risk ratio between observed and expected for all vaccine technologies. Both FTT and GLMM methods showed similar results, with GLMM giving greater asymmetry in funnel plots and slightly wider prediction intervals (SI, Section 2). Leave-one-out sensitivity analysis was performed for some analyses (SI, Section 2). No single study significantly affected the computed effect size for each outcome, as shown by influence analysis and outlier remotion (SI, Section 2). Baujat plots were also produced when feasible to elucidate the contribution of a single study to the overall random-effect model heterogeneity (SI, Section 2).
Comments (0)