Study design and population group
This was a single-center observational study conducted from July 2020 to July 2022 at the Obstetric Department of Guangzhou Women and Children’s Medical Center, Guangdong, China. Pregnant women with suspected PE from 28 + 0 weeks to 33 + 6 weeks were enrolled in this study. Inclusion criteria included: (1) singleton pregnancy; (2) having new onset only one of suspicious symptoms but not reach PE diagnose criteria: hypertension, proteinuria, fetal growth restriction (FGR), decreased levels of platelets, increased liver enzymes, or edema. Exclusion criteria included: (1)multiple pregnancies; (2) confirmed PE diagnosis; (3) chronic hypertension; (4) have taking antihypertensive drugs; (5) concomitant chronic liver and kidney disease ;(6) lost follow-up in delivery.
Participants underwent both ABPM and sFlt-1/PlGF sampling at the time of initial inclusion. Maternal clinical characteristics including age, parity, height, weight, gestational age at the time of sampling were also collected. Participants received written information to donate their surplus aliquots of serum samples during prenatal care for scientific research before their written consent was obtained. This study was approved by the Institutional Ethics Committee of the Guangzhou Women and Children’s Medical Center (Reference number: 2017022008).
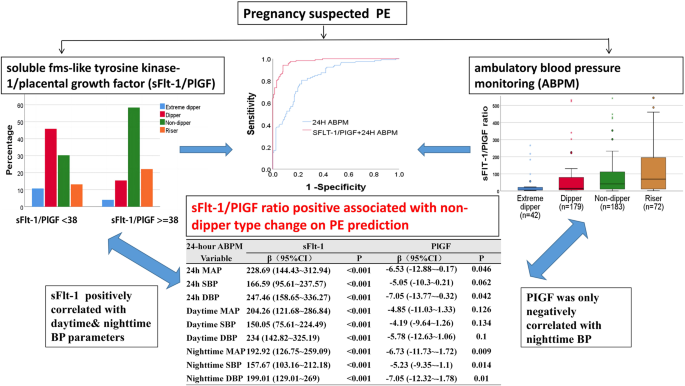
Participants were divided to two groups: sFlt-1/PlGF < 38 group and sFlt-1/PlGF ≥ 38 group, as sFlt-1/PlGF ratio 38 was considered a high NPV for PE. These two groups were followed up for 2 weeks from first inclusion to determine whether PE developed, and then followed until delivery. Delivery gestational weeks, peripartum maternal organ dysfunction levels, and fetal outcomes were also collected.
Outcome definitions
PE refers to the new onset of hypertension accompanied by one or more of the following newonset conditions at ≥20 weeks’gestation (ISSHP diagnostic criteria): (1) proteinuria (2) other maternal end-organ dysfunction, including: (a) neurological complications (eclampsia, altered mental status, blindness, stroke, clonus, severe headaches, or persistent visual scotomata), (b) pulmonary edema, (c) hematological complications (platelet count < 150,000/μL, disseminated intravascular coagulation, hemolysis), (d) acute kidney injury (such as creatinine ≥ 90 μmol/L or 1 mg/dL), (e)liver involvement (alanine transaminase (ALT) or aspartate transaminase (AST) > 40 IU/l) with or without right upper quadrant or epigastric abdominal pain, (f)uteroplacental dysfunction (placental abruption, fetal growth restriction, abnormal umbilical artery Doppler waveform analysis, or intrauterine fetal death) [10].
Serum sample collection and sFlt-1&PlGF measurement
A 5 ml peripheral maternal blood sample was obtained from patients with suspected PE at inclusion. The serum samples were separated by centrifugation at 2000 g for 10 min at room temperature and immediately stored at −80 °C until assayed at an independent laboratory. The levels of sFlt-1 and PlGF were measured using an electrochemiluminescence immunoassay analyzer (cobas e 411 system; Roche Diagnostics GmbH, Mannheim, Germany).
Ambulatory blood pressure monitoring
Ambulatory BP was measured on the non-dominant arm during a 24-h period using an Oscar 2 ambulatory BP monitor (SunTech Medical). Measurements were recorded every 30 min from 6 am to 10 pm as daytime, and every 60 min from 10 pm to 6 am the following day as nighttime. During monitoring, the patients were instructed to (i) engage in normal activities, (ii) stop moving and talking during measurement, (iii) keep the arm still with the cuff at heart level at the time of cuff inflation, and (iv) record information on symptoms and events that may have influenced BP, meal times, in a diary. The measurements were downloaded to the computer and were considered technically satisfactory only if at least 85% of values during daytime and nighttime periods were satisfactory. The following values were obtained by ABPM: SBP(systolic blood pressure), DBP(diastolic blood pressure), HR(heart rate) in daytime, nighttime, 24 h period. The mean arterial pressure (MAP) was calculated as (SBP + (2 × DBP))/3 [11].
BP change pattern types groups of the ABPM: The nocturnal BP drop rates of 10%–20%, 0%–10%, <0%, and >20% were defined as dipper, non-dipper, riser, and extreme dipper types of ABPM, respectively. And the equation nocturnal blood pressure drop rate = (daytime average blood pressure value − nighttime average blood pressure value)/daytime average blood pressure value × 100% reflected the daytime and nighttime fluctuations of blood pressure.
Statistical analysis
Maternal characteristics and perinatal period outcome data were compared between sFlt-1/PlGF <38 group and sFlt-1/PlGF ≥38 group. Data were expressed as mean ± standard deviation (SD) or median (25th–75th percentile as interquartile ranges) for continuous variables based on the distribution. Independent t-tests were used for normally distributed data, Mann–Whitney U-tests if otherwise. Counts with proportions were presented as frequencies and percentages, and tested using the chi-square (χ2) test.
A multivariable linear correlation analysis was conducted using Spearman correlation to assess the relationship between parameters of ABPM (mean blood pressure, systolic blood pressure, diastolic blood pressure, heart rate during daytime, nighttime, and 24 h) and sFlt-1, PlGF, as well as the sFlt-1/PlGF ratio. The results, including 95% confidence intervals (CI), were reported after adjusting by maternal characteristics(including maternal age, BMI, whether IVF, multiparity).
Binomial logistic regression analysis was used to generate a predictive model for PE by sFlt-1/PlGF, parameters of ABPM, and their combination, respectively. The area under curve (AUC) in receiver operating characteristic curve, were calculated to determine the performance of prediction model. For each of the models, sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), were calculated. The power of the markers or parameters to increase prediction value was evaluated by discrimination (integrated discrimination index (IDI)) and reclassification analyses (free net reclassification index (NRI)).
All the analyses were performed with the statistical software packages R (http://www.R-project.org, The R Foundation) and P value of <0.05 was considered statistically significant.


Comments (0)