
Remember me




Simultaneous bilateral quadriceps tendon ruptures (BQTR) is a debilitating injury associated with trauma and systemic disease.1,2 Obesity, diabetes mellitus, chronic renal failure, hyperparathyroidism, hypertension, and anabolic steroid use are commonly associated risk factors.1,2 Simultaneous BQTR is rare, as a recent study found only 105 cases in English and German literature.1 Parathyroid carcinoma is also a very rare condition that may result in hyperparathyroidism, with <0.1% of hyperparathyroidism cases attributed to parathyroid carcinoma.3,4
The presentation of a patient with simultaneous BQTR and parathyroid carcinoma is reported. To date, several cases of simultaneous BQTR have been reported in individuals with hyperparathyroidism; however, only one other case (ie, a brief editorial) was attributed to parathyroid carcinoma.2,5 The patient provided written informed consent for this case to be reported.
Case ReportA 31-year-old man presented to an orthopaedic clinic with a sudden onset of severe bilateral knee pain and weakness after routine yard work. The patient reported lifting a lightweight wooden log from the ground and then felt a painful pop in his left leg. While falling, he felt a pop in his right leg. He was unable to bear weight and presented to the emergency department, where he was diagnosed with bilateral patellar fractures and was referred for orthopaedic consultation.
The patient was seen in clinic 3 weeks after the injury and was still nonambulatory. His medical history included hypertension controlled with calcium channel blockers, and he was previously a short-term smoker (3 years), but he quit 10 years earlier. He denied anabolic steroid use, diabetes mellitus diagnosis, or any other pertinent medical history.
A bilateral lower extremity examination demonstrated 3+ suprapatellar edema, and he was tender to palpation over the quadriceps tendons with a palpable defect. He was unable to actively extend either knee.
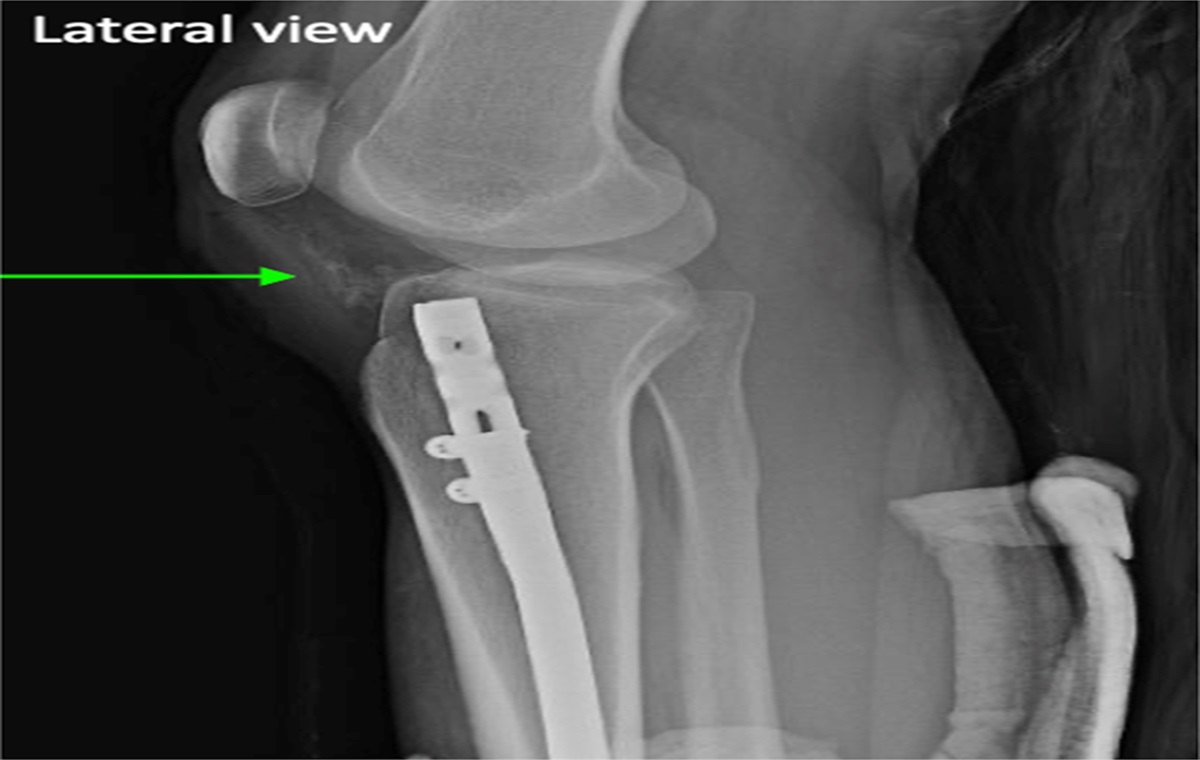
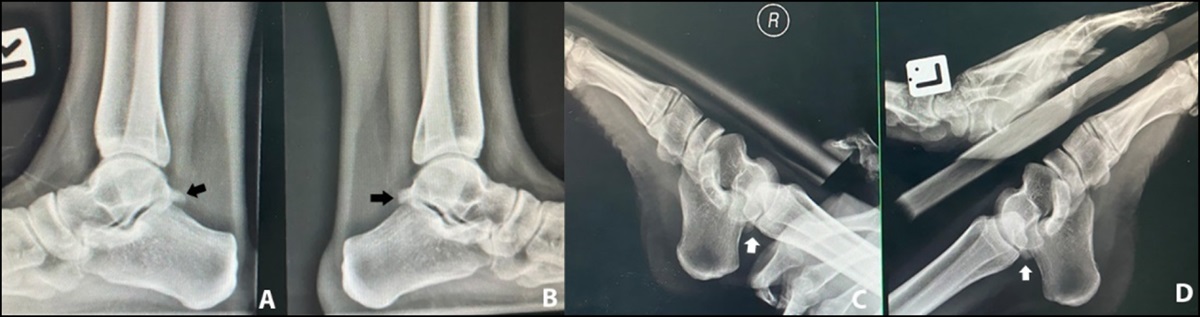
Initial radiographs of the left leg demonstrated a low-lying patella with an avulsion fracture of the superior pole. The right knee radiograph was normal. The patient then underwent magnetic resonance imaging of both knees, which revealed a complete rupture of the left quadriceps tendon and a full-thickness central tear of the right quadriceps tendon. He was advised to undergo surgical repair of both tendons because of his debilitating symptoms and loss of function.
A presurgical complete blood count and complete metabolic panel revealed abnormal creatinine, blood urea nitrogen, serum calcium, phosphorus, calcium-phosphorus product, alkaline phosphatase, aspartate aminotransferase, alanine aminotransferase, hemoglobin, and hematocrit (Table 1). On further questioning, the patient revealed that he had been experiencing intermittent nausea, vomiting, abdominal pain, nocturia, and polydipsia for the past 3 months.
Table 1 - Initial Laboratory Results CBC Case Reference Range Hematocrit (%) 30.8a 37.5%-51.0% Hemoglobin (g/dL) 10.6a 12.6-17.7 CMP Sodium (mmol/L) 137 135-148 Potassium (mmol/L) 4.4 3.6-5.2 Chloride (mmol/L) 107 95-110 Glucose (mg/dL) 95 70-110 Creatinine (mg/dL) 3.7a 0.6-1.3 BUN (mg/dL) 32a 7-18 Total protein (g/dL) 7.0 6.4-8.2 Serum albumin (g/dL) 4.0 3.4-5.0 Serum calcium (mg/dL) 15.3a 8.8-10.5 Phosphorus (mg/dL) 4.8a 2.5-4.5 Calcium-phosphorus product 79a <55 Alkaline phosphatase (IU/L) 394a 41-137 Aspartate aminotransferase (IU/L) 12a 15-37 Alanine aminotransferase (IU/L) 26a 30-65 Additional blood work performed Intact serum PTH (pg/mL) 1273a Upper limit of 65BUN = blood urea nitrogen, CBC = complete blood count, CMP = complete metabolic panel, PTH = parathyroid hormone.
aOutside of reference range for adult male patients.
A nephrology consultation led to a CT urogram, which revealed bilateral kidney stones, an atrophic left kidney, and atrophy of the lower pole of the right kidney. His glomerular filtration rate was 24/mL·min·1.73 m2 with hypercalcemic crisis, which indicated stage 4 chronic kidney disease associated with nephrocalcinosis and likely long-term hypercalcemia.
A physical examination performed by a consulting endocrinologist revealed a small, firm mass in the region of the thyroid gland. His intact serum parathyroid hormone (PTH) was 1273 pg/mL, 20 times greater than the upper normal limits. An ultrasonography of the thyroid revealed a left-sided mass present in either the thyroid or parathyroid glands, and a magnetic resonance imaging with gadolinium confirmed a left-sided parathyroid mass. Ultrasound-guided core biopsy confirmed a parathyroid carcinoma. A metastatic bone survey demonstrated lytic skull lesions, characteristic of hyperparathyroidism; cortical bone resorption of the proximal humerus; and C7 transverse process, but no metastatic lesions were observed. Our patient was aggressively managed with intravenous (IV) fluids, furosemide, and calcitonin and hemodialysis to correct the serum calcium level and halt advancement to acute renal failure. The patient responded well to the IV management, and serum calcium dropped from 12.8 to 10.9 mg/dL before surgery.
An otorhinolaryngologist consultation recommended en bloc resection of the parathyroid mass. He underwent surgery for tumor removal and bilateral quadriceps tendon repair 5 days after our initial examination.
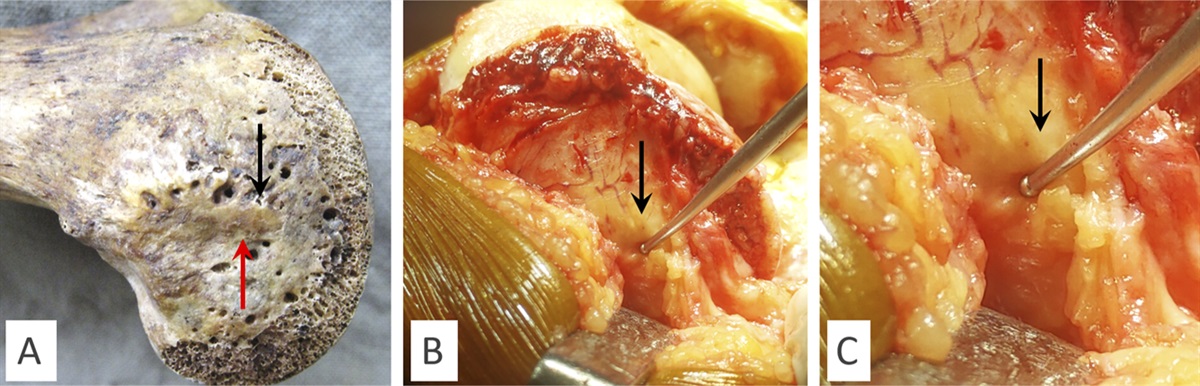
Surgical exploration of the right knee showed a quadriceps tendon tear in the central portion. The medial and lateral portions of the tendon were intact, and the retinaculum had no tears. Overall, the tendon had a very healthy appearance, except for the distal portion that avulsed from the patella, which was débrided. Five Tycron suture was then passed through the tendon using a Krackow-type stitch, which was passed through the superior pole of the patella and then tied over the inferior pole of the patella (Figure 1). The soft tissue was oversewn using one Vicryl suture. It was possible to flex the knee to 90°.
 Figure 1:
Figure 1: Photographs depicting a superior lateral view of the anterior knee. The surgeon pictured is placing transosseous sutures from the quadriceps tendon through the patella and tightening the sutures to reapproximate the quadriceps tendon against the patella.
On the left knee, a similar approach was used and there was a complete rupture of the quadriceps tendon off the superior pole of the patella. Extensive tearing down the lateral retinaculum and partially through the medial retinaculum was present. A 1-mm cottony Dacron suture was woven through the central portion of the tendon using a Bunnell-type suture. Peripherally, a five Tycron suture was woven using a Krackow stitch, passed through the patella from superior to inferior, and tied over the inferior pole. The retinacular tears were repaired with interrupted 0 Ethibond sutures. The knee could easily flex to 90° and demonstrated normal patellar tracking and approximation of the tendon to the patella. Later, the histological examination of the en bloc resection confirmed parathyroid carcinoma (Figure 2).
 Figure 2:
Figure 2: Images showing sections of the malignant tumor showing pleomorphic malignant epithelioid cells arranged in rosettes, columns, and fascicles. The tumor showed focal degenerative change and some dyshesiveness. Based on serologic and histologic evaluation, diagnosis of parathyroid carcinoma was made.
Postoperatively, the patient was permitted to bear weight as tolerated in knee immobilizers. Postoperative laboratory test results indicated hypocalcemia with hungry bone syndrome as calcium levels dropped to 7.6 mg/dL and PTH was intact at 66 pg/mL, which indicated suppression of the remaining parathyroid glands. The patient was managed using oral vitamin D3 and calcium and IV infusion of calcium gluconate.
Two weeks postoperatively, he transitioned from knee immobilizers to long hinged braces locked in full extension. Over the ensuing several weeks, he was gradually allowed incrementally to increase his braces' range of motion. Five months after surgery, the patient walked independently without pain or abnormal gait. He denied pain, and his physical examination revealed full active range of motion bilaterally.
He then began a low-weight and high-repetition strength program and returned to work full-time without restriction.
At 15 years postoperatively, the patient had one brief bout of prepatellar bursitis that resolved with activity modification and short-term bracing treatment. His kidney disease worsened and eventually required a living donor kidney transplant. Dual-energy radiograph absorptiometry revealed improvement of his 1-year AP spine L1 to L4 T-scores (T = −1.1 to −0.1). The patient exhibited normalization of blood work and was cancer-free.
DiscussionSimultaneous BQTR secondary to hyperparathyroidism is well-documented in the literature.1,6–9 Parathyroid carcinoma is a known cause of hyperparathyroidism, albeit rare, with an incidence of <0.1% of all cancer cases over a 10-year period.10–12 We found one previous case in an editorial documenting the coexisting conditions of simultaneous BQTR and parathyroid carcinoma during our literature review; however, little detail was provided with only short-term follow-up.5
Simultaneous BQTR may be diagnosed clinically as patients usually present with bilateral posttraumatic loss of knee extension, severe knee pain, and a palpable defect at the superior pole of their patella.13 The suprapatellar defects may be unnoticed in obese patients or those without a complete quadriceps tendon tear. Plain radiographs may demonstrate obliteration of the quadriceps tendon shadow, a suprapatellar mass, a suprapatellar calcific density, and possible patellar displacement.14
Most cases of closed QTR occur with a contraction of the quadriceps muscle while the knee is flexed.1,7,8 In the absence of trauma, one must consider predisposing conditions potentially responsible for simultaneous BQTR.1,2 Most cases reported associated with hyperparathyroidism were due to secondary hyperparathyroidism with chronic renal failure.2,15 While primary hyperparathyroidism has been linked with simultaneous BQTR, it is rare, accounting for only 5% of cases between 1949 and 2002.2,13
The clinical presentation of hyperparathyroidism includes polyuria or polydipsia, myalgia or arthralgia, weight loss, and nephrolithiasis.10,16 During the initial laboratory workup, special attention should be paid to creatinine, calcium, and PTH levels to assess kidney function.10 Nearly 75% of these patients will present with calcium levels above 15.5 mg/dL, with approximately 12% of these patients expected to present in hypercalcemic crisis, like our patient.17,18 Studies of patients with confirmed parathyroid carcinoma have also demonstrated PTH levels up to 12 times greater than normal limits.16 Once parathyroid cancer is diagnosed, en bloc resection is usually a curative procedure, as in our case.19
ConclusionAlthough BQTR have been reported, this case raises awareness for orthopaedic surgeons to have a high index of suspicion for systemic disease when the patient history, mechanism of injury, and clinical examination provide unusual or conflicting findings.
AcknowledgmentsWe thank Mark Fahey and James Franklin for their assistance during orthopaedic surgery and Duncan S. Postma and Adrian Roberts for their work on the parathyroidectomy. We also thank Robert Bradford for the nephrology consultation and Charles Manning Jr. for the pathology interpretation.
References 1. Neubauer T, Wagner M, Potschka T, Riedl M: Bilateral, simultaneous rupture of the quadriceps tendon: A diagnostic pitfall? Rort of three cases and meta-analysis of the literature. Knee Surg Sports Traumatol Arthrosc 2007;15:43-53. 2. Shah MK: Simultaneous bilateral rupture of quadriceps tendons: Analysis of risk factors and associations. South Med J 2002;95:860-866. 3. Owen RP, Silver CE, Pellitteri PK, et al.: Parathyroid carcinoma: A review. Head Neck 2011;33:429-436. 4. Ruda JM, Hollenbeak CS, Stack BC: A systematic review of the diagnosis and treatment of primary hyperparathyroidism from 1995 to 2003. Otolaryngol Head Neck Surg 2005;132:359-372. 5. Benameur H, Chaves C, Sautet A, Feron JM, Cambon-Binder A: Spontaneous bilateral quadriceps tendon rupture revealing a parathyroid carcinoma. Joint Bone Spine 2018;85:131-132. 6. Loehr J, Welsh RP: Spontaneous rupture of the quadriceps tendon and patellar ligament during treatment for chronic renal failure. Can Med Assoc J 1983;129:254-256. 7. MacEachern A, Plewes J: Bilateral simultaneous spontaneous rupture of the quadriceps tendons. Five case reports and a review of the literature. J Bone Joint Surg Br 1984;66:81-83. 8. Stein V, Petersen W, Laprell H: Bilateral spontaneous rupture of the quadriceps tendon in a patient with Wilson disease. A case report. Unfallchirurg 1999;102:733-736. 9. Ribbans WJ, Angus PD: Simultaneous bilateral rupture of the quadriceps tendon. Br J Clin Pract 1989;43:122-125. 10. Thompson SD, Prichard AJN: The management of parathyroid carcinoma. Curr Opin Otolaryngol Head Neck Surg 2004;12:93-97. 11. Hundahl SA, Fleming ID, Fremgen AM, Menck HR: Two hundred eighty-six cases of parathyroid carcinoma treated in the U.S. Between 1985-1995: A national cancer data base report. The American college of surgeons commission on cancer and the American Cancer Society. Cancer 1999;86:538-544. 12. Fraker DL: Update on the management of parathyroid tumors. Curr Opin Oncol 2000;12:41-48. 13. Browner BD: Skeletal Trauma: Basic Science, Management, and Reconstruction. Philadelphia, PA, Saunders/Elsevier, 2009. 14. Campbell W, Canale S, Beaty J: Campbell's operative orthopaedics. Philadelphia, PA, Mosby/Elsevier, 2008. 15. De Franco P, Varghese J, Brown WW, Bastani B: Secondary hyperparathyroidism, and not β2-microglobulin amyloid, as a cause of spontaneous tendon rupture in patients on chronic hemodialysis. Am J Kidney Dis 1994;24:951-955. 16. Wynne AG, Van Heerden J, Carney JA, Fitzpatrick LA: Parathyroid carcinoma: Clinical and pathologic features in 43 patients. Medicine (Baltimore) 1992;71:197-205. 17. Shane E, Bilezikian JP: Parathyroid carcinoma: A review of 62 patients. Endocr Rev 1982;3:218-226. 18. Obara T, Fujimoto Y: Diagnosis and treatment of patients with parathyroid carcinoma: An update and review. World J Surg 1991;15:738-744. 19. Fujimoto Y, Obara T, Ito Y, Kodama T, Nobori M, Ebihara S: Localization and surgical resection of metastatic parathyroid carcinoma. World J Surg 1986;10:539-547.
Comments (0)