Physician stress and burnout are recognizable problems among orthopaedic surgeons, and numerous studies have shown that stress can negatively affect both surgical performance and patient outcomes.1–3 Orthopaedic surgery is a physically demanding career in which repetitive injuries are not uncommon and can affect productivity and career duration. Davis et al2 found approximately 50% of orthopaedic surgeons surveyed had sustained work-related injury and 10% required time off as a result. A better understanding of the physical toll of surgical procedures might aid surgeons in optimizing techniques and performance. This underscores the importance of understanding the relationship among surgeon stress, performance, and productivity and patient outcomes. Surgeon physiologic stress, however, can be difficult to quantify. Variations in the health or fitness level of the individual surgeon, differences in training and experience, and patient factors can all affect levels of physiologic stress, as occurs in athletes. In contradistinction to most athletics, however, surgery is typically performed largely in a static posture or even sitting, and the physical task in surgery largely involves the upper extremities more than the lower extremities. Furthermore, surgery involves intense mental stress, as well as physical, and the cerebral component of surgical care is not insignificant.
A number of studies have investigated heart rate (HR) and calorie consumption as markers of physician stress during surgery.3–5 Bergovec and Orlic examined physical stress on the surgeon during total hip arthroplasty. Kremer et al reported that in spine surgery, the attending surgeon had higher calorie consumption and HR variability than the resident surgeon.3 Whitney et al6 showed that surgeons performing simulated spine surgery on a cadaver had higher energy consumption than at resting baseline. Another study demonstrated a larger energy consumption during total hip arthroplasty compared with total knee arthroplasty.7 To our knowledge, there has been no study in the English language literature that investigated a spine surgeon's energy expenditure as various surgical variables change.
A number of tools exist to measure energy consumption such as oxygen consumption, weight change, HR, calorie consumption, and others.3,6 With the advent of wearable technology such as HR monitors and triaxial accelerometers, their use and study has increased, with some studies showing them as valid tools to estimate energy consumption.8,9 In particular, our study group validated the use of an upper arm triaxial accelerometer (Fitbit) and a HR monitor to calculate energy expenditure and calorie consumption during simulated cadaveric spine surgery.6
The purpose of our study was to quantify a fellowship-trained spine surgeon's energy consumption during actual spine surgery using the validated method of an intraoperative HR monitor and triaxial accelerometer amidst various conditions. Our desire was to investigate the effects various patient and intraoperative variables such as patient's BMI, wearing of lead garments, usage of instrumentation and intraoperative navigation (O-arm use), status as a primary or revision surgical procedure, and anatomic spinal region have on surgeon energy consumption. Our null hypothesis is that there is no change in surgeon energy consumption as patient and intraoperative factors are altered. These findings could ultimately place into context surgeon stress as it relates to surgical execution.
Methods
This study was approved by the institutional review board at Albany Medical Center. The senior author, a fellowship-trained spine surgeon with over 10 years of experience (Lawrence), wore a chest strap HR monitor (Polar) and upper arm triaxial accelerometer (Fitbit one) during 164 spine surgeries. These monitors had been used and validated in prior studies.6 Consideration of surgeon energy consumption played no role in surgical decision making. The surgeon's choice of using instrumentation, intraoperative navigation, tranexamic acid (TXA), or lead (full body vest with a thyroid shield) was not affected by this investigation. Chart review was used to record TXA use, patient BMI, primary or revision status of the surgery, use of O-arm CT navigation, use of instrumentation, and anatomic location of the spine surgery. Anatomic location of the spine was split into two categories. The first contained surgeries performed on the cervical, cervicothoracic, and thoracic regions (upper spine) and the second on the thoracolumbar, lumbosacral, and lumbopelvic regions (lower spine). BMI was stratified into three categories: <25, 25.1 to 29.9, and >30. The HR monitor and accelerometer provided assessments of our primary end points including mean HR (mean HR), maximum HR (max HR), calories (cal) consumed per minute, total calories as measured by the Polar device (P calories), and total calories as measured by the Fitbit device (F calories) consumed. Alpha was set to P ≤ 0.05. Data analysis was conducted using International Business Machines SPSS Statistics for Windows-Version 27. Shapiro-Wilk test for data normality rejected the null hypothesis, thereby nonparametric Mann-Whitney test was used to test between surgery types, TXA use, instrumentation use, and lead use. Bivariate testing included Mann-Whitney and chi square tests. BMI stratification into three groups used the Kruskal-Wallis test statistically. Multivariate backward stepwise linear regression was used to predict k/cal expenditure. Variables were eliminated based on variance inflation factors and statistical nonsignificance (P ≥ 0.05).
Results
One hundred sixty-two surgeries were included in the final analysis.
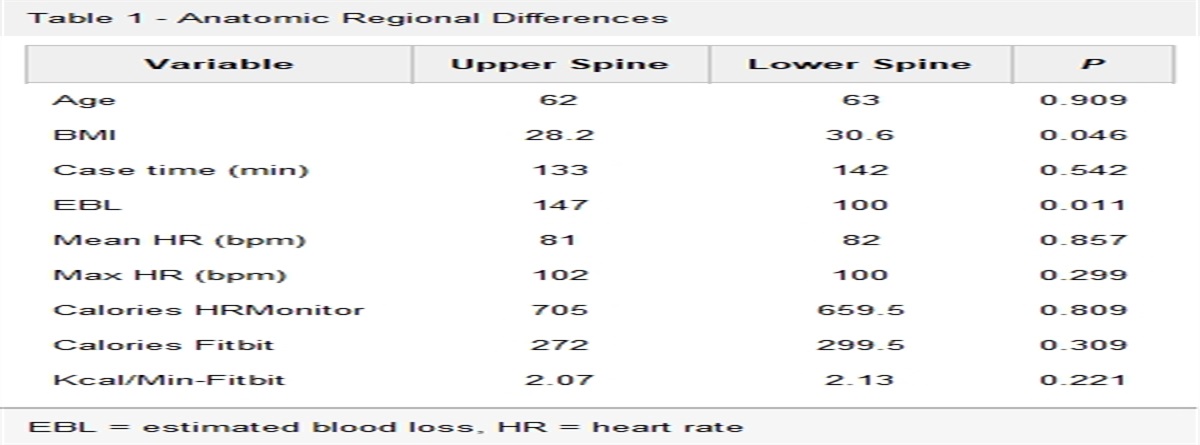
The median patient age was 62 years, and median BMI was 29.02. Using anatomic spine locations, statistically significant differences existed for BMI (P = 0.046) and estimated blood loss (P = 0.011) as summarized in Table 1. Case time, used as a proxy for equivalence, between the upper and lower spine was nonsignificant (P = 0.542). Use of TXA did not have a statistically significant effect on mean HR or max HR as summarized in Table 2. However, use of TXA did have a statistically significant effect on case time (P = 0.001), estimated blood loss (P = 0.001), calories based on HR monitor (P = 0.001), calories based on Fitbit (P = 0.001), and Kcal/min based on Fitbit (P = 0.048). Use of instrumentation was statistically significant for all variables, except for mean HR (P = 0.152) and Kcal/min-Fitbit (P = 0.599) as summarized in Table 3. Use of lead (full body apron and thyroid shield) aprons did not have a significant effect on max HR (P = 0.602), P calories (P = 0.558), F calories (P = 0.079), and Kcal/min-Fitbit (P = 0.704) as summarized in Table 4. Use of O-arm CT navigation was associated with a statistically significant P values for every variable tested (P ≤0.05), thereby distinguishing itself as the only divisor in bivariate analysis with every variable statistically significant (Table 5). BMI was statistically significantly higher (P = 0.046) among the lower spine group (30.8) compared with the upper spine group (28.4). Statistically significant differences existed between primary and revision surgeries for case time (P = 0.001), estimated blood loss (P = 0.001), and calories consumed based on Fitbit (P = 0.045) (Table 6). Comparing surgery type (upper spine/lower spine), statistically significant differences were found between instrumentation (P = 0.001) and lead use (P = 0.045). No significant differences were observed for use of TXA (P = 0.100). The Kruskal-Wallis test showed no statistical differences among continuous variables (P ≥ 0.05) when BMI categories were stratified. Finally, with stepwise backward linear regression, the most stable prediction model using Kcal/min (Fitbit) as the dependent variable included the following predictors: lower spine surgery type (P = 0.030), case time (P = 0.031), use of TXA (P = 0.035), and no use of lead (P = 0.009).
Table 1 -
Anatomic Regional Differences
Variable
Upper Spine
Lower Spine
P
Age
62
63
0.909
BMI
28.2
30.6
0.046
Case time (min)
133
142
0.542
EBL
147
100
0.011
Mean HR (bpm)
81
82
0.857
Max HR (bpm)
102
100
0.299
Calories HRMonitor
705
659.5
0.809
Calories Fitbit
272
299.5
0.309
Kcal/Min-Fitbit
2.07
2.13
0.221
EBL = estimated blood loss, HR = heart rate
Table 2 -
Usage of Tranexamic Acid
No. TXA
TXA
P
Case time (min)
78
148
0.001
EBL (mL)
50
100
0.001
Mean HR (bpm)
81
81
0.939
Max HR
97
101
0.056
Calories HR monitor
417
711
0.001
Calories Fitbit
179
313
0.001
Kcal/min-Fitbit
1.91
2.13
0.048
EBL = estimated blood loss, HR = heart rate, TXA = tranexamic Acid
Table 3 -
Usage of Instrumentation
Variable
No Instrumentation
Instrumentation
P
Case time (min)
90
155
0.001
EBL (mL)
50
100
0.001
Mean HR (bpm)
81
82
0.152
Max HR
96
102.5
0.001
Calories HR monitor
364
741
0.001
Calories Fitbit
178
324
0.001
Kcal/min-Fitbit
2.02
2.16
0.599
EBL = estimated blood loss, HR = heart rate
Table 4 -
Usage of Intraoperative Lead Aprons
Variable
No Lead
Lead
P
Case time (min)
125
159
0.002
EBL (mL)
100
100
0.011
Mean HR (bpm)
82
81
0.019
Max HR
101
100
0.602
Calories HR monitor
364
741
0.558
Calories Fitbit
178
324
0.079
Kcal/min-Fitbit
2.02
2.16
0.704
EBL = estimated blood loss, HR = heart rate
Table 5 -
Usage of Intraoperative Navigation
Variable
No O-Arm
O-Arm
P
Case time (min)
115
180.5
0.001
EBL (mL)
75
200
0.001
Mean HR (bpm)
81
83
0.031
Max HR
100
103
0.004
Calories HR monitor
532
1017
0.001
Calories Fitbit
233.5
408.5
0.001
Kcal/min-Fitbit
2.01
2.26
0.01
EBL = estimated blood loss, HR = heart rate
Table 6 -
Primary Versus Revision Surgical Status
Variable
Primary
Revision
P
Case time (min)
132
169
0.001
EBL (mL)
100
150
0.001
Mean HR (bpm)
81
83
0.106
Max HR
100
102
0.516
Calories HR monitor
645
742
0.063
Calories Fitbit
277
327
0.045
Kcal/min-Fitbit
2.06
2.21
0.199
EBL = estimated blood loss, HR = heart rate
Discussion
This study quantified a fellowship-trained spine surgeon's calorie consumption and HR during spine surgery in different surgical environments for the first time. Among the bivariate comparisons, the most statistically significant findings among the three measures of calories consumed (calories HR monitor, calories Fitbit, and kcal/min with Fitbit) were with the usage of TXA (Table 2), usage of instrumentation (Table 3), usage of intraoperative navigation/O-arm (Table 5), and status as a primary or revision case (Table 6). These data support the precision of these instruments for measuring caloric consumption and identifying trends. While some studies have called into question the accuracy of these wearable devices,10 our data show their usefulness during spine surgery cases and intraoperative assessment tools to reflect surgeon physiologic parameters accurately. Regarding measuring HR, we believe the use of the Polar HR monitor allowed for the most accurate measurements given Polar's superiority in measuring HR among different wearables.11,12
This study presents valuable insight into the concept of intraoperative surgeon stress and distress. There are no tools available to assess surgeon stress, and thus, it is unknown whether it can markedly affect the outcomes in complex spinal surgery. The current line of thought believes that lack of surgeon stress results in a lower average HR, calorie consumption, and a decreased rate of medical error. Extensive surgical training would seem to minimize the adverse effects of stress by creating methods of coping and sharpening technical skills. Measures such as regular rest, managing nutrition, timely breaks during extensive surgical cases, and the support of a skilled assistant or co-surgeon are all applicable ideas that could serve to mitigate stress. However, the true extent of this remains unknown. Additional research and more validated data are warranted.
The fact that BMI had no effect on mean HR and calorie consumption may be surprising, given surgeons' frequent frustrations while operating on patients with a higher BMI, but is consistent with a prior study that showed BMI had no effect on energy consumption in total joint arthroplasty.7
Interestingly, TXA use was associated with a higher caloric expenditure in all three categories assessed (HR monitor, caloriesFitbit, and Kcal/min with Fitbit). Use of TXA did not affect mean or max HR, although max HR neared statistical significance (P = 0.056). Rieger et al5 suggested that HR variability is an indication of surgeon stress. Although not seen in this study, TXA's success at decreasing intraoperative blood loss should theoretically have had the simultaneous effect of decreasing surgeon stress in measurable terms. In our study, however, TXA may have been used only for the more complex cases; therefore, it was not correlated with decreases in measureable parameters of surgical stress and energy expenditure.
Intraoperative lead (full body apron and thyroid shield) use had no statistically significant effect on any of our end points. Although wearing lead vests during surgery may be uncomfortable,13 that discomfort does not seem to result in increased energy expenditure or HR variability, based on these findings.
Use of instrumentation did affect maximum HR and calories consumed based on Polar and Fitbit measures. The fact that Kcal/min was not statistically significant could be attributed to the fact that a fellowship-trained spine surgeon may not have any more stress while instrumenting the spine than while only decompressing the spine. Instrumentation is associated with an increased Polar and Fitbit calorie consumption; however, this is negated by no change in F calories per minute. This can be attributed to the typically longer surgical time when instrumentation is added to the surgical procedure.
Revision spine surgery used statistically significantly more calories than primary surgery, based on Fitbit, which could be driven by revision cases lasting statistically longer. The fact that the Polar monitor Kcal/min, mean HR, and max HR were not statistically different may indicate that surgeon stress was not markedly affected by case type. This again may highlight this surgeon's experience and may vary with less experienced surgeons.
Use of intraoperative navigation (O-arm) surprisingly showed statistically significant differences in all end point variables. Increased median values for all variables when the O-arm was used could be explained by the increased complexity of these cases requiring navigation of the increase in resident participation in these cases, potentially elevating the attending surgeon's HR and calorie consumption. In fact, it has been reported that the attending surgeon has an increased HR variability compared with the resident surgeon.3
Breakdown by anatomic region allowed our group to divide the spine into case groups that primarily were at the level of or levels below the termination of the spinal cord. No difference was observed in energy consumption between those two groups. Possibly, more surgical experience can mitigate stress or energy consumption even in higher risk cervical or thoracic cases.
Finally, our linear regression found that the following end point variables were most predictive of caloric expenditure per minute: lower (thoracolumbar) spine surgery type, longer case time, use of TXA, and no use of lead.
This study had a robust patient volume examining multiple intraoperative variables that affected surgeon experience in terms of energy expenditure and HR variation. This study, however, had several limitations. The measures of HR and calorie consumption serve as proxies for surgeon stress but are not definitive. In addition, a single surgeon monitored the parameters of interest. As such, the results at this stage are not generalizable beyond the practice of the senior author who partook in the study. Stratification according to pathology and urgency of case was also not included, which we hypothesize could affect the results. Additional investigation is needed to confirm the aforementioned concepts and provide generalizability. Comparative monitoring of resident physicians might have allowed for comparisons that would examine the effect of experience. In theory, enhanced experience in surgery should lead to improved intraoperative efficiency of motion and reduced energy expenditure for more experienced surgeons. Reduced surgeon stress as a consequence of experience might provide for less extreme variations in intraoperative HR. Furthermore, the personal fitness baseline of the individual may play an important role in the assessment of intraoperative surgeon physiology.
An analysis of specific surgical procedures might further elucidate differences that were not apparent in the aggregate data. For instance, O-arm navigation vs fluoroscopy for a posterior C1-2 fusion may reveal notable differences in HR and energy consumption with the use of navigation. Considering that surgical time based on the multiple bivariate analyses is the biggest driver of energy consumption, optimization of time in the operating room may be the most important factor in lowering energy expenditure in spine surgery.
Finally, the fact that we conducted multiple unpaired comparisons may have increased our risk of type I statistical error. This study is the first that looks at surgeon energy utilization comprehensively in spine surgery, orthopaedics, or neurosurgery and should serve as a first step in allowing for a greater understanding of the physical stress of surgery and potential ways to reduce it and allow for greater physician health and reduced burnout.
References
1. Hui RWH, Leung KC, Ge S, et al.: Burnout in orthopaedic surgeons: A systematic review. J Clin Orthop Trauma 2019;10suppl 1:S47-S52.
2. Davis WT, Sathiyakumar V, Jahangir AA, Obremskey WT, Sethi MK: Occupational injury among orthopaedic surgeons. J Bone Joint Surg Am 2013;95:e107.
3. Kremer J, Reinhold M: Intraoperative stress in orthopaedic spine surgery: Attending surgeon versus resident. Orthopade 2016;45:1039-1044.
4. Thielmann B, Boeckelmann I: Heart rate Variability as an Indicator of mental Stress in surgeons - a Review of the literature. Zentralbl Chir 2015;141:577-582.
5. Rieger A, Stoll R, Kreuzfeld S, Behrens K, Weippert M: Heart rate and heart rate variability as indirect markers of surgeons' intraoperative stress. Int Arch Occup Environ Health 2014;87:165-174.
6. Whitney DC, Ives SJ, Leonard GR, VanderBrook DJ, Lawrence JP: Surgeon energy expenditure and substrate utilization during simulated spine surgery. J Am Acad Orthop Surg 2019;27:e789-e795.
7. Sharkey PF, Danoff JR, Klein GR, Parvizi J: Surgeon energy expenditure during total joint arthroplasty. J Arthroplasty 2007;22:210-212.
8. Bouten CV, Westerterp KR, Verduin M, Janssen JD: Assessment of energy expenditure for physical activity using a triaxial accelerometer. Med Sci Sports Exerc 1994;26:1516-1523.
9. Price K, Bird SR, Lythgo N, Raj IS, Wong JYL, Lynch C: Validation of the Fitbit One, Garmin Vivofit and Jawbone UP activity tracker in estimation of energy expenditure during treadmill walking and running. J Med Eng Technol 2017;41:208-215.
10. Dooley EE, GolaszewskiBartholomew NMJB, Bartholomew JB: Estimating accuracy at exercise intensities: A comparative study of self-monitoring heart rate and physical activity wearable devices. JMIR Mhealth Uhealth 2017;5:e34.
11. Gillinov S, Etiwy M, Wang R, et al.: Variable accuracy of wearable heart rate monitors during aerobic exercise. Med Sci Sports Exerc 2017;49:1697-1703.
12. Pasadyn SR, Soudan M, Gillinov M, et al.: Accuracy of commercially available heart rate monitors in athletes: A prospective study. Cardiovasc Diagn Ther 2019;9:379-385.
13. Wertheimer A, Kirzner N, Olaussen A, Abetz J, Martin C, Jones C: Keeping your cool - a simple reusable neck cooler in orthopaedic surgery: A pilot randomized controlled trial. ANZ J Surg 2018;88:1294-1297.





Comments (0)