
Remember me




Tibial osteotomy can be indicated for the correction of many lower extremity deformities, prompting the use of various fixation hardware (Figure 1). The high tibial osteotomy (HTO) to address coronal plane deformity about the knee is a common example. Osteotomy at other locations may be indicated to address sagittal plane, rotational, or length deformities. Early literature expressed concern regarding the rate of major complications when performing tibial osteotomy: compartment syndrome, vascular injury, persistent neurologic injury,1–3 and even death.4 Although improvements of surgical technique and technology have improved safety,5,6 the rate of such complications remains non-negligible.7 Because of lingering concerns regarding major complications reported in early investigations of tibia osteotomy,8 some surgeons may be hesitant to electively correct tibial deformities or may consider performing the osteotomy at a different anatomic site than the otherwise preferred bony location. Perhaps because of this apprehension, with the exception of HTO,9 limited contemporary literature exists describing complications of and techniques which maximize safety for tibial osteotomies.
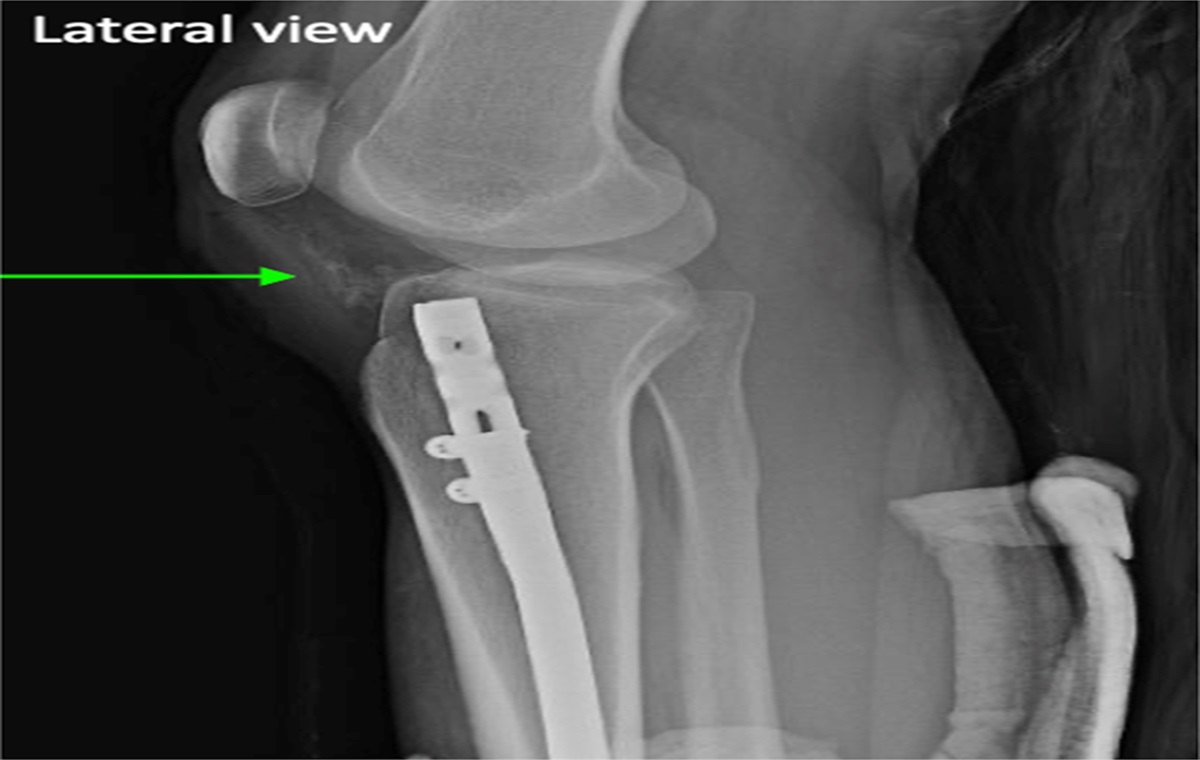
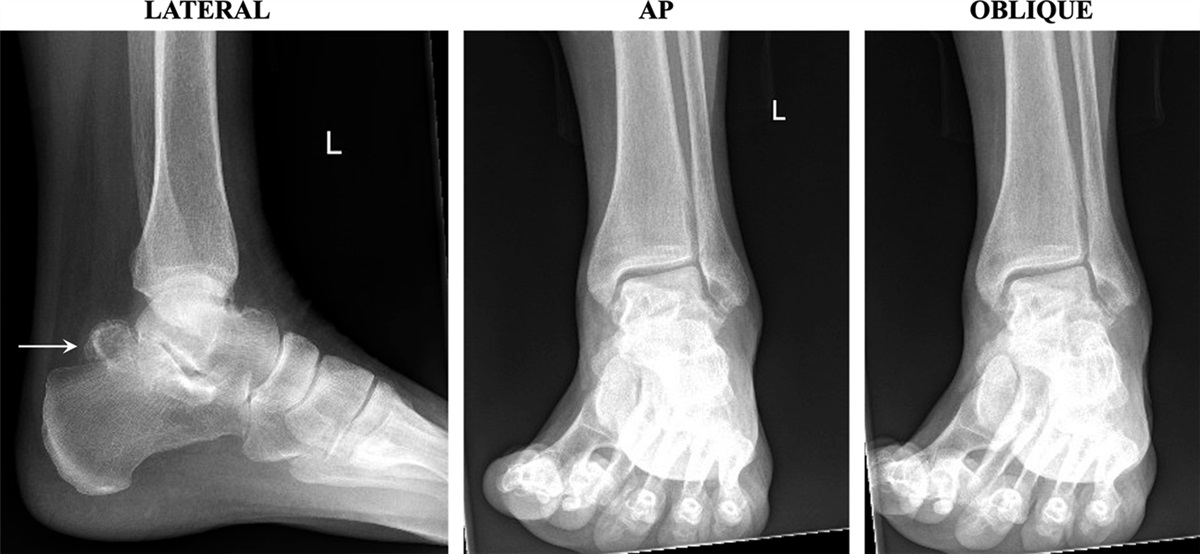
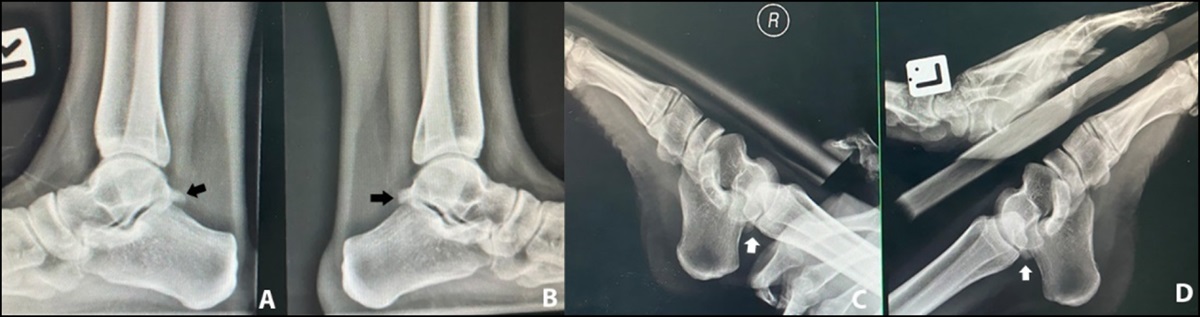
 Figure 1:
Figure 1: Radiographs showing the examples of osteotomies and fixation included in this study. A, A 52-year-old woman with staged bilateral high tibia osteotomies, fixated with plate and screws, to address tibia-based genu varum; she did not have any fasciotomy. B, A 65-year-old woman with right proximal metaphyseal tibia osteotomy and mid-diaphyseal fibula osteotomy, fixated with a dynamic hexapod external fixator, to address torsion; she had an anterior compartment fasciotomy. C, A 21-year-old man with left diaphyseal tibia and fibula osteotomy, fixated with dynamic nail, to address short stature related to hypophosphatemic rickets; he had anterior and lateral compartment fasciotomies. D, A 41-year-old woman with left supramalleolar tibia and fibula osteotomy, fixated with a dynamic hexapod external fixator, to address a multiplanar deformity; she did not have any fasciotomy. The radiographically dense struts and wires are part of a robotically self-controlled programmable adjustment system.
This study was performed to help address that knowledge gap. The primary aim was to evaluate the major complications that occurred after tibial osteotomy performed at various anatomic locations for a diverse variety of indications.
MethodsAfte institutional ethics approval, a retrospective chart review was performed of our practice's surgical registry. Inclusion criteria were tibia osteotomy (any location, any indication) with follow-up through the conclusion of care, performed during the years of 2019 to 2021. Exclusion criteria were tibia osteotomy performed in the setting of existing infection (five limb segments). This yielded 108 limb segments (87 patients).
A chart review identified demographics, indication for surgery, tibial osteotomy location, fixation hardware used, whether the fibula was osteotomized, whether tranexamic acid (TXA) was administered, whether (and which) prophylactic compartment fasciotomy was performed, and the venous thromboembolism chemoprophylaxis regimen.
Outcomes evaluated were major complications: compartment syndrome, vascular injury, nerve injury, infection, delayed/nonunion, broken hardware, other issues prompting surgical intervention, deep vein thrombosis (DVT), and pulmonary embolism (PE).
The radiology picture archiving and communication software used for planning the osteotomies was Sectra picture archiving and communication software (Sectra). Hexapod frame adjustment software used was that provided by the specific device manufacturer, depending on which hexapod product was used for each individual case. Descriptive statistics were calculated using Google Sheets (Google LLC). Comparative statistical analysis was not performed.
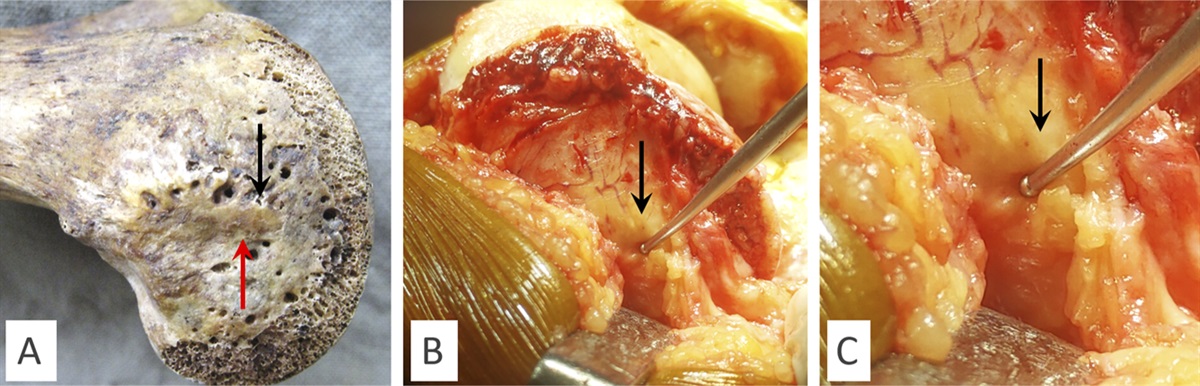
A full description of techniques used for the osteotomies summarized herein is beyond the scope of this manuscript. However, the following principles and considerations were essential and universally applicable. HTOs were approached through a 12-cm longitudinal incision medially, with the cut trajectory from the proximal metaphyseal flare toward the lateral plateau corner guided by a 2-mm guidewire placed centrally. A pneumatic powered oscillating saw with a 40-mm long blade made the initial cuts through the central and posterior tibial cortex; the anterior trajectory preserved the tibial tubercle with the distal tibia by changing the saw trajectory to obliquely cut through the plateau anterior to the joint surface but posterior to the tubercle. Metal retractors protected the posterior soft tissues and also the patellar tendon. Long, thin osteotomes without a continuously widening taper were used to extend the osteotomy toward the lateral subplateau but preserving the lateral hinge, and laminar spreaders were used to achieve the opening gap as needed, which was then filled with allograft wedge and bone void filler paste and stabilized with a locking plate. Fibula osteotomy was never performed for HTOs, and neither were peroneal nerve releases. Complete osteotomies (those without a hinge) were performed by first drilling multiple paths along the trajectory of the osteotomy with a solid core drill bit appropriate for the size of the bone, generally 4 to 5 mm diameter. These osteotomies were completed with manual osteotomes. Manual string-style (Gigli) saws or powered saws were not used, to minimize heat generated and potential associated thermal injury to the bone. Retractors generally were not used for manual osteotome osteotomies because these incisions were generally small. Local soft-tissue protection was achieved by ensuring the osteotome was firmly against bone before impacting, carefully listening to sound changes, gently performing wrench-assisted osteotome rotation as the osteotomy neared completion. In all surgeries, the entire leg was supported above and below the osteotomy, generally with at least two bumps made from sterile towels wrapped in sterile adhesive drape or elastic bandage. These bumps were critically important to prevent the leg from dropping or otherwise rapidly changing gross position upon completion of the osteotomy, which could lead to acute stretch or even laceration against a cut bone surface. Fasciotomies were performed using the full length of a compartment using a fasciotome featuring an “elbow” along its length to slide beneath the skin.
ResultsTable 1 presents the demographics and surgical variables. The average age was 38.0 ± 15.6 (range, 5.7 to 72.8) years. Men represented 57/108 = 53%. Notable aspects include the near-complete rate of TXA administration (107/108 = 99%) and the very high rate of aspirin for DVT chemoprophylaxis (93/108 = 86%). The three most common anatomic locations for osteotomy were the high tibia (35/108 = 32%, 32/35 = 91% medial opening, 3/35 = 9% medial closing), proximal metaphysis (30/108 = 28%), and diaphysis (32/108 = 30%). Fixation was mostly provided with plate and screw (38/108 = 35%) or dynamic external frame (36/108 = 33%). Regarding prophylactic fasciotomy, 33/34 = 97% of anterior releases were performed for patients with a single diaphyseal (26/32 = 81%) or proximal metaphysis (7/30 = 23%) osteotomy; the other fasciotomy was performed for a patient who had multiple osteotomy locations (1/3 = 33%). Specifically, 0/35 = 0% of HTOs had fasciotomy. Myriad fixation options were used for patients who had anterior fasciotomy: 3/34 = 9% had dynamic frames, 20/34 = 59% had static intramedullary nails, 10/34 = 29% had dynamic nails, and 1/34 = 3% had plate and also nail fixation. Lateral compartment release was performed for 16/65 = 25% of fibula osteotomies (none were performed without an associated fibula osteotomy). The tibial osteotomy was performed in the diaphysis for 15/16 = 94% of lateral fasciotomies, with the remaining one associated with a proximal metaphysis osteotomy.
Table 1 - Patient Demographics and Surgical Variables Variable Data: no. (% of 108) (fasciotomies) Anterior fasciotomy 34 (32%) Lateral fasciotomy 16 (15%) Fibula osteotomy 65 (60%) Intraoperative TXA 107 (99%) Chemoprophylaxis None 3 (3%) Aspirin 93 (86%) Rivaroxaban 8 (7%) Multiagent 4 (4%) Osteotomy location High tibia 35 (32%) (0) Proximal metaphysis 30 (28%) (7, 23%) Diaphyseal 32 (30%) (26, 81%) Distal metaphysis 2 (2%) (0) Supramalleolar 6 (6%) (0) More than one location 3 (3%) (1, 33%) Fixation Plate and screw 38 (35%) Dynamic frame 36 (33%) Static frame 20 (19%) Dynamic nail 12 (11%) Plate and screw plus dynamic nail 2 (2%) Indication High tibia varus/valgus 30 (28%) (0) Supramalleolar varus/valgus 1 (1%) (0) Other varus/valgus 15 (14%) (4, 27%) Biplanar 22 (20%) (11, 50%) Multiplanar 13 (12%) (2, 15%) Lengthening 12 (11%) (5, 42%) Torsion 8 (7%) (7, 88%) Malunion 5 (5%) (4, 80%) Procurvatum/recurvatum 2 (2%) (1, 50%)The primary outcome investigated was major complications, which are itemized in Table 2. None of the 108 patients had any of the most concerning complications: compartment syndrome, vascular injury, or nerve injury. Two patients developed a DVT (2%), but none experienced a PE. One patient (1%) required surgery to address infection: a 27-year old woman with a left multiplanar deformity treated with a hexapod developed infection persistent after frame removal, which resolved after a soft-tissue débridement.
Table 2 - Major Complications Overall Complications Occurrences Compartment syndrome 0 Vascular injury 0 Nerve injury 0 Infection surgery 1 (1%) Delayed/nonunion 8 (7%) Broken hardware 0 Other additional surgery 11 (10%) DVT 2 (2%) PE 0DVT = deep vein thrombosis, PE = pulmonary embolism.
Table 3 outlines the interventions for delayed/nonunion, and Table 4 outlines other situations of unplanned surgery. Nine segments (8%) in eight patients had intervention for delayed or nonunion. Five of the segments required relatively minor interventions to stimulate the bone in the osteotomy site, such as percutaneous wire drilling of the regenerate, bone marrow aspirate injection, placement of bone morphogenetic, or nail dynamization. Ten segments (9%) in nine patients had additional surgery for other reasons (Table 4). Most of these were relatively minor (hematoma evacuation, repeat osteotomy, distal tibia-fibula stabilizing screw, gastroc-soleus recession for equinus during lengthening, repeat osteotomy for preconsolidation, or supplemental frame fixation). More substantial surgeries were one revision fixation for malalignment and two patients who fractured between hardware or after hardware removal, prompting osteosynthesis nailing.
Table 3 - Summary of Delayed/Nonunion Age Sex Side, Indication, Location, Fixation Management 30 women Right, multiplanar deformity, proximal metaphysis, static nail Percutaneous wire drilling 65 women Right, torsion and short, proximal metaphysis, hexapod frame Supplemental ring fixation 22 men Bilateral, stature lengthening, diaphysis, MILN Bone marrow aspirate injection 27 men Right, multiplanar deformity, multiple osteotomy locations, plate/screw Bone marrow aspirate concentrate injection with bone morphogenic protein-2 sponge carrier 35 women Right, torsion, diaphysis, static nail Dynamization 56 women Left, short, diaphysis, MILN Bone marrow aspirate concentrate injection with bone morphogenic protein-2 sponge carrier, with subsequent exchange nailing 23 women Left, biplanar deformity, proximal metaphysis, static nail Percutaneous drilling, bone marrow aspirate concentrate injection, autograft from Gerdy tubercle 54 women Left, biplanar deformity and short, proximal metaphysis, MILN Conversion to hexapod frame to improve stability and achieve correctionMILN = motorized intramedullary lengthening nail.
HTO = high tibial osteotomy, MILN = motorized intramedullary lengthening nail.
This study had the primary aim to evaluate the rate of major complications after elective tibial osteotomy. The most important finding is that osteotomies can be performed in many anatomic areas of the tibia, for a variety of indications, using myriad fixation techniques, while avoiding the most catastrophic major complications: compartment syndrome, vascular injury, nerve injury, and PE. No events of these occurred in our cohort of 108 limb segments. Interventions for less calamitous issues such as delayed or nonunion, peri-implant fracture, and other adverse events associated with deformity care did occur, but none led to permanent disability. In our opinion, this suggests that surgeons with training in and experience with safe tibial osteotomy techniques should feel empowered to correct tibial deformity at the appropriate anatomic location, without excessive concern that a serious complication is likely to result. Understanding the situations which increase risk, and mitigating the risk via techniques or technology, is critical to optimizing safety.
Other than death, compartment syndrome is likely the most concerning complication associated with tibial osteotomy. Compartment syndrome can occur from insufficient inflow of oxygen and nutrition or reduced outflow of deoxygenated blood and metabolites. Examples include acutely reducing compartment volume with deformity correction or increasing compartment pressure (bleeding). A fasciotomy expands the volume available for intracompartmental anatomy, reducing pressure. A limited incision approach may be insufficient in acute compartment syndrome10 but is often sufficient when performed for prophylactic situations,11 including tibial osteotomy.5,8,12 Prophylactic fasciotomy for lengthening was reported by 1978,12 and prophylactic fasciotomy has rarely caused detectable muscle injury.13 When not routinely performing compartment release, Krengel and Staheli14 reported a rate of 2/39 = 5% compartment syndrome for proximal tibial osteotomy versus 0/13 = 0% for distal tibial osteotomy. When routinely performing prophylactic anterior fasciotomy, Stotts and Stevens11 reported no compartment syndrome in 59 tibial rotational osteotomies for adolescents and young adults. Our group's main indication for anterior compartment fasciotomy is acute deformity correction, in any plane, except in HTO. In particular, we routinely perform prophylactic anterior fasciotomy when imparting acute correction in the meta-diaphyseal or diaphyseal tibia. Gradual-only correction such as with a lengthening nail or frame is not usually an indication for fasciotomy. We feel that a lateral compartment release is unnecessary without a fibula osteotomy and may be most useful for acute rotation. Complete longitudinal compartment releases can be performed through a 1-cm incision using a fasciotome featuring an “elbow” bend, advanced antegrade, and retrograde. Fasciotomy with scissors is more difficult and may injure adjacent structures.15
Preventing bleeding reduces intracompartmental pressure. Preoperative TXA does this effectively and safely with minimal recognized risk,16 specifically including tibial osteotomy.9 A second dose around four hours after the first dose provides additional benefit.17 Few contraindications other than medication allergy18 or perhaps a history of seizures19 have been recognized. We gave TXA to 107/108 = 99% of this study's patients; no TXA-related adverse events occurred. One patient did not receive TXA because of a concern for inducing a blood clot; in retrospect, this likely need not have been a contraindication. Although this study is not designed or intended to evaluate the specific impact of TXA alone on preventing compartment syndrome or other complications, we believe the apparent safety benefit likely substantially outweighs the risk. This is based on our data identifying no adverse events apparently attributable to TXA in our cohort and also the aforementioned literature explicitly identifying the benefits of TXA with very minimal risks. Additional considerations to limit bleeding include injectable bone void fillers tamponade the cut bone edges and drains to provide egress of extravasated blood.8
Besides compartment syndrome, a vascular injury, specifically arterial injury, is another serious complication. Voluminous literature describes popliteus arterial injury risk during HTO, including these two which explore the relevant anatomy both with and without fibular osteotomy.20,21 In the proximal fibula, the anterior tibial artery and peroneal artery are vulnerable to tibial and fibular osteotomies.22 Reports of arterial injuries beyond the proximal tibia are rare,23 particularly in the supramalleolar region.24 Percutaneous osteotomy technique featuring predrilling optimizes cosmesis and soft-tissue integrity but impairs visibility of neurovascular anatomy. Drilling with two hands,25 using a sharp and well-designed drill bit spinning at full speed,26 optimizes tactile feedback to avoid plunging and produces lower temperatures.27 Accessory incisions, to improve visibility of the bone, allow careful28 predrilling or achieve direct access to improve safety when a single approach is limiting.29 Similarly, when using a saw during an open approach, favorable positioning (knee flexion to move the popliteus artery posterior) is easy and recommended but unreliable on its own,20 and anatomic variation occurs.30 Especially for HTO, encircling the bone with retractors prevents adjacent soft-tissue laceration, not only from the saw blade tip but also from the oscillations,31 which can cause arterial pseudoaneurysm even if true laceration does not occur.23 Irrigation during drilling and sawing reduces temperature32 but can obscure visibility so may be more convenient in spurts between active power utilization.
There are other arterial safety considerations. Acute shortening can kink arteries,33 at or before 4 cm34; in such situations, frequent pulse checks are important. Acute angular or rotational correction can also constrict arteries, which can present as a secondary neurologic dysfunction.3 Vessel injury from sudden position change on osteotomy completion35 can be prevented by supporting the extremity above and below. External fixation can achieve gradual correction, either during surgery or subsequently, preventing vessel kinking. The fixator can remain for the duration of healing or can be exchanged for a plate or a nail.36
Nerve injuries are a third major potential complication. The bulk of nerve injuries are also reported regarding HTO, as an acute varus correction of valgus deformity stretches the common peroneal nerve.37 Any stretch either acutely or during the course of correction can induce a nerve palsy.38 Nerve protection principles are similar to arterial principles, with the following fundamentals optimizing safety. Peroneal nerve release about the fibular head39 can be performed prophylactically or therapeutically. Our group's main indication for peroneal nerve decompression is acute correction of valgus and/or external torsion in the diaphysis or metadiaphysis. The tibial nerve is most often stressed distally after correction of ankle varus, equinus and/or procurvatum, and in lengthening situations. Prophylactic or therapeutic release of the entire tarsal tunnel40 is beneficial, especially if acute bony correction induces equinus, prompting tendoachilles lengthening or gastrocnemius-soleus complex recession. Our group's main indication for tibial nerve decompression via a tarsal tunnel release is the acute correction of varus and/or internal torsion in the distal metaphysis or metadiaphysis. It deserves specifically reiterating that an apparent neurologic deficit may actually be because of a primary arterial compromise.3
Although it is hoped that this study lends support to the safety of tibial deformity correction when best technique and technology practices are used, there are important limitations to consider. The primary may be the generalizability of the outcomes. The surgeons who performed these procedures all focus on deformity correction and have had specific fellowship training in the techniques and principles described; not all surgeons have this familiarity. Another potential limitation is the unequal number of procedures performed at any given osteotomy level or with any given fixation option, limiting equal data interpretation. In addition, as a retrospective study, it is possible that subclinical changes in sensation or motor function may not have been detected. A major strength of the study is the variety of deformity indication, osteotomy location, and fixation type. No events of compartment syndrome, arterial injury, or nerve dysfunction occurred despite the broad range of patient ages, indications, and fixation options supports the utility of the principles and techniques espoused.
ConclusionsTibial osteotomy can be safely performed throughout the tibia to manage a variety of indications without causing major complications such compartment syndrome, vascular injury, and neurologic deficit. Optimizing safety with specific surgical techniques, reducing bleeding, performing prophylactic fasciotomy and nerve release, and consideration of gradual instead of acute correction all contribute to preventing complications. Considering and using these diverse skills and resources can improve correction by allowing the surgeon to make surgical decisions based on deformity correction principles rather than compromise the reconstruction because of an outsized fear of unavoidable complications.
References 1. Schrock RD Jr: Peroneal nerve palsy following derotation osteotomies for tibial torsion. Clin Orthop Relat Res 1969;62:172-177. 2. Hutter CG Jr, Scott W: Tibial torsion. J Bone Joint Surg Am 1949;31A:511-518. 3. Steel HH, Sandrow RE, Sullivan PD: Complications of tibial osteotomy in children for genu varum or valgum. Evidence that neurological changes are due to ischemia. J Bone Joint Surg Am 1971;53:1629-1635. 4. Jackson JP, Waugh W: The technique and complications of upper tibial osteotomy. A review of 226 operations. J Bone Joint Surg Br 1974;56:236-245. 5. Tetsworth KD, Thorsell JD: Combined techniques for the safe correction of very large tibial rotational deformities in adults. J Limb Lengthening Reconstr 2015;1:6. 6. Jacobi M, Wahl P, Jakob RP: Avoiding intraoperative complications in open-wedge high tibial valgus osteotomy: Technical advancement. Knee Surg Sports Traumatol Arthrosc 2010;18:200-203. 7. Schenke M, Dickschas J, Simon M, Strecker W: Corrective osteotomies of the lower limb show a low intra- and perioperative complication rate-an analysis of 1003 patients. Knee Surg Sports Traumatol Arthrosc 2018;26:1867-1872. 8. Herring JA, Mubarak SJ: Complications of a tibial osteotomy. J Pediatr Orthop 1983;3:625-628. 9. Ma J, Lu H, Chen X, Wang D, Wang Q: The efficacy and safety of tranexamic acid in high tibial osteotomy: A systematic review and meta-analysis. J Orthop Surg Res 2021;16:373. 10. Köstler W, Strohm PC, Südkamp NP: Acute compartment syndrome of the limb. Injury 2005;36:992-998. 11. Stotts AK, Stevens PM: Tibial rotational osteotomy with intramedullary nail fixation. Strategies Trauma Limb Reconstr 2009;4:129-133. 12. Coleman SS, Stevens PV: Tibial lengthening. Clin Orthop Relat Res 1978;October:92-104. 13. Degen N, Randeu T, Wolf F, et al.: Prophylactic fasciotomy in tibial osteotomies: Functional results. Unfallchirurgie 2022;125:716-722. 14. Krengel WF III, Staheli LT: Tibial rotational osteotomy for idiopathic torsion. A comparison of the proximal and distal osteotomy levels. Clin Orthop Relat Res 1992;283:285-289. 15. Hutchinson MR, Bederka B, Kopplin M: Anatomic structures at risk during minimal-incision endoscopically assisted fascial compartment releases in the leg. Am J Sports Med 2003;31:764-769. 16. Calapai G: Systematic review of tranexamic acid adverse reactions. J Pharmacovigilance 2015;3:3-7. 17. Fang Q, Zhang Z, Wang D, et al.: Effect of tranexamic acid on blood management during a high tibial osteotomy: A systematic review and meta-analysis. Orthop Surg 2022;14:1940-1950. 18. Chauncey JM, Wieters JS: Tranexamic Acid. Treasure Island, FL, StatPearls, 2022. 19. Lin Z, Xiaoyi Z: Tranexamic acid-associated seizures: A meta-analysis. Seizure 2016;36:70-73. 20. Zaidi SH, Cobb AG, Bentley G: Danger to the popliteal artery in high tibial osteotomy. J Bone Joint Surg Br 1995;77:384-386. 21. Georgoulis AD, Makris CA, Papageorgiou CD, Moebius UG, Xenakis T, Soucacos PN: Nerve and vessel injuries during high tibial osteotomy combined with distal fibular osteotomy: A clinically relevant anatomic study. Knee Surg Sports Traumatol Arthrosc 1999;7:15-19. 22. Rupp RE, Podeszwa D, Ebraheim NA: Danger zones associated with fibular osteotomy. J Orthop Trauma 1994;8:54-58. 23. Rickman M, Saleh M, Gaines PA, Eyres K: Vascular complications of osteotomies in limb reconstruction. J Bone Joint Surg Br 1999;81:890-892. 24. Colin F, Gaudot F, Odri G, Judet T: Supramalleolar osteotomy: Techniques, indications and outcomes in a series of 83 cases. Orthop Traumatol Surg Res 2014;100:413-418. 25. Ding A, Marmor M: Drilling technique can minimize plunging. J Orthop Trauma 2019;33:e309-e312. 26. Alajmo G, Schlegel U, Gueorguiev B, Matthys R, Gautier E: Plunging when drilling: Effect of using blunt drill bits. J Orthop Trauma 2012;26:482-487. 27. Ali Akhbar MF, Yusoff AR: Drilling of bone: Effect of drill bit geometries on thermal osteonecrosis risk regions. Proc Inst Mech Eng H 2019;233:207-218. 28. Chun KC, So BJ, Kang HT, Chun C-H: Pseudoaneurysm Formation due to popliteal artery injury caused by drilling during medial opening wedge high tibial osteotomy. Knee Surg Relat Res 2018;30:364-368. 29. Iobst C: An alternative tibial osteotomy technique. Strategies Trauma Limb Reconstr 2020;15:47-49. 30. Jang Y, Nguyen K, Rocky S: The aberrant anterior tibial artery and its surgical risk. Am J Orthop (Belle Mead NJ) 2018;47(7). 31. Kang T, Lee DW, Park JY, Han H-S, Lee MC, Ro DH: Sawing toward the fibular head during open-wedge high tibial osteotomy carries the risk of popliteal artery injury. Knee Surg Sports Traumatol Arthrosc 2020;28:1365-1371. 32. Pandey RK, Panda SS: Drilling of bone: A comprehensive review. J Clin Orthop Trauma 2013;4:15-30. 33. Ellenhorn JI, Fowl RJ, Akers DL, Kempczinski RF: Femur fracture with limb shortening causing occlusion of a polytetrafluoroethylene femoral popliteal graft. J Vasc Surg 1990;12:558-560. 34. Atbasi Z, Demiralp B, Kilic E, Kose O, Kurklu M, Basbozkurt M: Angiographic evaluation of arterial configuration after acute tibial shortening. Eur J Orthop Surg Traumatol 2014;24:1587-1595. 35. Kim K-I, Thaller PH, Ramteke A, Lee SH, Lee S-H: Corrective tibial osteotomy in young adults using an intramedullary nail. Knee Surg Relat Res 2014;26:88-96. 36. Rozbruch SR, Fragomen AT: Hybrid lengthening techniques: Lengthening and then nailing (LATN) and lengthening and then plating (LAP), in Kocaoğlu M, Tsuchiya H, Eralp L, eds: Advanced Techniques in Limb Reconstruction Surgery. Berlin, Heidelberg, Springer Berlin Heidelberg, 2015, pp 85-99. 37. Curley P, Eyres K, Brezinova V, Allen M, Chan R, Barnes M: Common peroneal nerve dysfunction after high tibial osteotomy. J Bone Joint Surg Br 1990;72:405-408. 38. Nogueira MP, Paley D, Bhave A, Herbert A, Nocente C, Herzenberg JE: Nerve lesions associated with limb-lengthening. J Bone Joint Surg Am 2003;85:1502-1510. 39. Nogueira MP, Hernandez AJ, Pereira CM, Paley D, Bhave A: Surgical decompression of the peroneal nerve in the correction of lower limb deformities: A cadaveric study. J Limb Lengthening Reconstr 2016;2:76. 40. Lamm BM, Paley D, Testani M, Herzenberg JE: Tarsal tunnel decompression in leg lengthening and deformity correction of the foot and ankle. J Foot Ankle Surg 2007;46:201-206.
Comments (0)