
Remember me

Credit: Sam Ogden
With the UK’s approval of Vertex and CRISPR Therapeutics’ exagamglogene autotemcel (Casgevy) for sickle cell disease and beta-thalassemia in November, expectations are high that the FDA will soon follow suit with their first green light for a gene-editing modality. But while the CRISPR–Cas9 editor that exa-cel uses is getting much of the credit, the therapy was enabled by decades of research into haemoglobin biology. In particular, the discovery of the transcription factor BCL11A unlocked the gene-editing opportunity.
“What Vertex and CRISPR Therapeutics have done is wonderful,” says Stuart Orkin, a paediatric haematologist and molecular biologist at the Harvard Medical School and HHMI, who unravelled BCL11A’s biology. “But it’s important that people know about the research and investment in science that went into this.”
A clinician first noticed in 1948 that babies only develop the symptoms of sickle cell disease at the age of about 6 months, leading to the hypothesis that a functional form of fetal haemoglobin might protect newborns from the effects of this blood disorder. Researchers spent decades trying to understand how the production of this protein gets switched off, with a view to turning it back on, but were stumped until the mid-2000s. “We were despondent,” recalls Orkin. “Most people who had been working on it were either working on different problems, were retired or were deceased.”
But the process of discovery lies “not in seeking new landscapes but in having new eyes,” says Orkin, borrowing from Marcel Proust. In this case, genome-wide association studies (GWAS) and other emerging technologies provided the light. Orkin and colleagues zeroed in on BCL11A in 2008, and in 2015 found a stretch of nucleotides that controls the expression of the transcription factor. Editing this Achilles heel lowers BCLA11a expression, restarting fetal haemoglobin production. “There was a lot of serendipity and a lot of good luck along the way,” says Orkin.
Exa-cel, making use of these insights, entered clinical trials in 2018. Haematopoietic stem cells are harvested from patients, edited and then re-infused — that is, after patients have received chemotherapy to make way in the bone marrow for the edited cells. It shows curative potential, although longer-term data are needed to prove that it has lasting power.
But exa-cel will cost millions of dollars, and its preconditioning regimen is harsh. Other options are needed to address the global burden of the disease. “This is not the end game,” says Orkin.
How did you get to BCL11A as a target?
I've been studying globin genes for more than 40 years. In the 1980s, when cloning first became possible, we isolated beta-thalassemia genes and determined the mutations that caused the disease. This was the first comprehensive molecular description of a disease. But the Holy Grail for us in haematology and globin genetics was really to understand why cells make predominantly β-globin after the neonatal period, rather than fetal haemoglobin. If we could make more fetal haemoglobin, we realized, it would provide a tremendous benefit for patients.
By the late 1990s and early 2000s, we were somewhat despondent that we would be able to understand it. We and others had looked for factors that might be responsible and hadn’t found any. We didn't even know how many factors might be involved. If there were 10 factors, there's nothing we could do about it. It was a black box.
Then, in mid-2004, Vijay Sankaran, then a MD-PhD student, came to my lab and wanted to work on the switch. I said “I want to work on the switch too. But we've tried a lot of things that have failed.” But we had some hypotheses and started petering along.
Then a colleague at Boston Children’s Hospital, Joel Hirschhorn, who was plugged into the human genetics GWAS community, became aware that the group of the late Antonio Cao in Sardinia had performed a GWAS study, looking at fetal haemoglobin levels and other traits. They submitted the work to the NEJM for publication, but it was rejected. The journal wanted confirmation from an independent cohort. We linked up with them, because Vijay had acquired DNA samples from the NIH’s natural history study of sickle cell disease in order to do GWAS. Data from this cohort confirmed the findings of the Sardinia GWAS, which identified BLC11A as a candidate locus.
NEJM still rejected a revised manuscript. Meanwhile, there was a report by Swee Lay Thein’s group in the UK in Nature Genetics that also pointed to BCL11A. We submitted the combined results from Sardinia and the NIH cohort to PNAS.
BCL11A was the new player on the block. At the tail end of Vijay’s PhD thesis, he showed in Science in 2008 that shRNA-mediated downregulation of BCL11A was accompanied by increased fetal haemoglobin expression.
You speculated then that targeted manipulation of BCL11A might lead to new therapies, years before CRISPR had arrived. How did you want to target it?
We didn't really have any idea how it would be done. Maybe small molecules, or zinc finger nucleases? That statement is the kind of thing you put into the conclusion of a paper to make it more interesting.
The stake in the ground for me was really our 2011 Science paper, where we showed that inactivation of BCL11A in erythroid cells rescued engineered sickle cell mice. That experiment showed that if you could achieve BCL11A inactivation by some means in humans, you would have a therapy. And it showed that targeting one factor was sufficient. That's really the basis for all the ongoing clinical work.
When did you turn to CRISPR?
In a 2013 Science paper, we showed that common genetic variation in BCL11A that leads to small but measurable differences in fetal haemoglobin levels resides in the intron of the gene. Using TALEN nucleases to remove the intron, we also showed that this region, an enhancer, is required for BCL11A expression, but only in erythroid cells. CRISPR was just coming on the scene at that time, and we were early adopters. In our 2015 Nature paper, we basically used CRISPR to find a vulnerable site in the enhancer that could be targeted with CRISPR.
That paper not only provided a clear path to a CRISPR therapy, but also highlighted the power of CRISPR as a research tool.
Exactly. This was one of the first papers describing unbiased genetic dissection of a regulatory element by CRISPR screening. We had a great system to do it in, because there was an application.
The site we identified is targeted by CRISPR and Vertex’s exa-cel, with the guide RNA described in that paper. They took out a non-exclusive license to use it. We made the conscious decision to make our license non-exclusive, so that any company could take a shot at it.
What will an FDA approval mean for you?
An approval is obviously going to be a landmark for gene editing. But I think it's also an illustration of how discoveries build on other discoveries from years before. Certainly we could not have made the progress we made if it weren't for the tools and insights available to us from other clinical, cellular and genetic studies. All that background was essential.
Many GWAS studies don't go anywhere, because we don't understand the rest of the biology. Many targets that are tested in the clinic don't get validated because there's no genetic substance behind them. For this one, we had the biology, the genetics and the tools.
The translation from our 2015 paper to the clinic only took a few years. It was remarkably fast. I think that it went the way it should go: the target discovery was made in the academic space, and drug developers who know how to execute did the clinical studies at scale for approval. It is a perfect example of how the ecosystem can work. CRISPR and Vertex should be congratulated for their superb execution. The field would have been set back otherwise.
Sickle cell disease, in many ways, is an orphan disease when it comes to investment. I hope that this work will stimulate interest into this disease, which affects many people not just in Africa, but also in South America and India.
Exa-cel’s cost and preconditioning therapy will preclude its global use. What’s needed for broader, global impact?
There are a few things to watch. One is that this is the first-generation CRISPR. There may be second-generation therapies that are as or more effective. The clinical results with exa-cel are excellent, but you could do a little better. We know how to get fetal haemoglobin to higher levels, and the question is whether pharma will make the investment to do that.
Work is also being done to make these therapies more scalable. One of these is to improve the preconditioning therapy. People are also holding out for in vivo gene editing [in which the cells are edited directly in patients]. I have concerns that this might not be possible any time soon, because we've learned from these trials that you have to modify 50% or more of a patient’s haematopoietic stem cells to get into the therapeutic range. I think we're far from where we need to be for efficient in vivo editing.
The third possibility, which I and others including Vertex are working on, is small molecules. BCL11A is validated. We know it's a good target. Transcription factors have been seen as undruggable, but now nothing is undruggable.
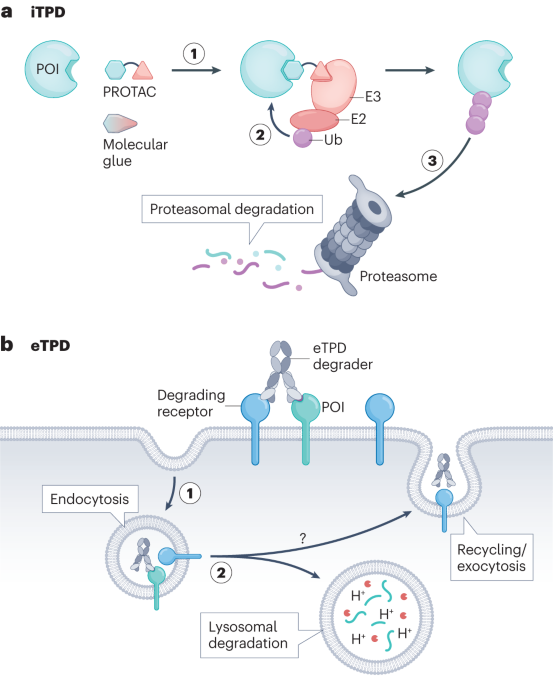
Such as with your degraders?
Degraders are one possible solution. I don't think we know what the solution is going to be yet, but we are winnowing away the choices.
My main focus, until I retire, is on trying to do what's necessary to understand the mechanism of how this protein works, in all its gory detail, so that we can get to small molecules. This keeps me in the game. I like the hunt.
This is the third time your research has paved the path to a new drug. You helped provide the molecular basis for Takeda’s recombinant von Willebrand factor (vWF), approved in 2018, and Epizyme’s EZH2 inhibitor, approved in 2020.
Those are two examples of situations where very talented trainees came into the lab and started new projects. With vWF, David Ginsburg, now a faculty member at the University of Michigan, joined my lab as my second postdoctoral fellow and wanted to clone vWF. This was when cloning a gene was a big thing. We cloned it, and that was published in Science [in 1985]. We worked on it together for a brief period of time, and then it was all his.
We filed a patent for this, and through a lot of interesting machinations — the patent was challenged and the decision was kicked along for years — the patent was not issued for around 30 years. Eventually Baxter [acquired by Shire and then Takeda] secured approval for recombinant vWF. And we get royalties, believe it or not, more than 30 years after we filed the IP. It's a great case study for a business school.
As for the SWI/SNF work, Charles Roberts, who now heads the cancer center at St. Jude, came into my lab as a postdoctoral fellow to work on a cancer project. A paper had just been published in Nature showing that the rhabdoid cancer predisposition syndrome was due to a germline mutation of one subunit, and I said “Gee, I think this will be an important thing for you to work on”. He set up mouse models to recapitulate the cancer, and we collaborated for a number of years on the mechanism and hit on a vulnerability for rhabdoid cells, EZH2, which is targeted by Epizyme’s drug.
Given this hat-trick, any project selection tips?
You’ve got to take lots of shots on goal, and they don't all go in. I guess I've had a few that made it to the goal. But very little of this work was motivated by trying to get an approved product to market. We're interested in discovering things, learning about biology, learning about disease, and doing things that are relevant to patients. It's the icing on the cake when you can actually deliver something.
You have to be patient. Delayed gratification is an attribute that you need to make it through this.
Comments (0)