
Remember me



One of most important challenges of aging is the ability to retain functional independence (Motamed-Jahromi and Kaveh, 2020). Many older adults report that preserving their ability to live independently and engage in activities of their own volition is one of the most important aspects of approaching older age. While functional independence is understandably associated with preserved cognitive abilities (Gamage et al., 2019) cognitive status in and of itself does not fully explain the capacity for some individuals to engage in vibrant, independent activities in their older age (Molenaar et al., 2023). Indeed, although the clinical definition of dementia is defined by impairments of activities of daily living (ADLs), a substantial number of individuals without dementia experience loss of independence and associated reductions in quality of life (QoL) (Colón-Emeric et al., 2013). Loss of independence also results in and exorbitant amount of public health expenditures, as many individuals not only lose their own ability to meaningfully contribute to society, but also usurp time and other tangible resources from family members who provide their care (Falck et al., 2022). Better understanding the predictors and associated intervention targets to retain independence is therefore an important public health problem (Morgan et al., 2019).
Emerging data suggest that chronic disease management is a major driver of successful aging and retaining functional independence. As the population ages, the number of individuals managing chronic medical conditions such as hypertension, obesity, cardiovascular, and cardiopulmonary disease has increased dramatically due to more successful treatment mitigating mortality rates for both cancer and cardiac diseases. Among chronic medical conditions that impact the population, obesity and hypertension are two of the major modifiable risk factors for loss of functional independence. Obesity and hypertension both increase the risk of numerous chronic conditions, including cognitive impairment, and higher levels of obesity in midlife are a robust predictor of cardiovascular disease, stroke, and excess death. Fortunately, these risk factors are highly modifiable through lifestyle modification among middle-aged adults, primarily managed through increasing physical activity, modifying dietary habits, and reducing caloric intake for weight maintenance. Individuals who are physically active during middle-age have approximately 40% lower risk of Alzheimer’s disease and related dementias (ADRD). Similarly, interventions for both weight loss hypertension have demonstrated improved cognitive function following treatment, suggesting that more adequate management of behavioral risk domains may help to protect against cognitive decline: the strongest driver of functional impairment. Because of the multiple skills needed to effectively manage chronic diseases, multicomponent interventions have been shown to have the greatest efficacy for improving physical activity (Chase, 2015). As noted in a prior comprehensive review of long-term physical activity intervention programs, ‘a multipronged approach to interventions with goal of affecting behavior change that can influence multiple systems (physical, cognitive, and psychological health) … using a personalized approach [and personalized goals that incorporates] social support” is most likely to succeed (Chase, 2015). This review will highlight one such high-level systems variable that helps to determine successful aging and can be readily personalized: self-regulation.
The present review attempts to address a critical gap in the existing literature linking chronic disease management to long-term cognitive decline by integrating across several previously disparate literature bases: self-regulatory behaviors and health behavior maintenance, psychological profiles predicting health behavior changes (e.g., neurocognitive, personality, and affective phenotypes), and chronic disease predictors of functional independence. Prior reviews have been limited in their lack of integration across relevant literatures, relying on an examination of either single-factor predictors of behavioral management, focusing within single domains of function (e.g., psychological, cognitive, or social) without attempting to integrate across domains of function, focusing on either the initiation or maintenance of activity without an attempt to bridge these divergent targets, or by proposing limited, personalized approaches that do not cultivate sustainable lifestyle patterns. The present review attempts to integrate these previously disparate areas of study, proposing a more unified framework by which clinicians can approach personalization of treatment to enhance long-term behavior change maintenance.
2 Self-regulation and resilience through behavioral flexibilitySocial and personality psychologists define self-regulation as the cognitive, emotional, and behavioral processes through which one establishes, monitors, and evaluates progress in personal goal pursuit (Karoly, 2010; Hoyle and Gallagher, 2015). Although prior work examining self-regulatory functioning in the context of aging has tended to focus on coping styles, an emerging literature suggests that flexibility in behavioral regulatory strategies is associated with better behavioral outcomes (Kato, 2020; Kato, 2021). Indeed, some individuals conceptualize psychological flexibility as a fundamental aspect of human health and effective behavioral coping with the inherent challenges of leading a fulfilling life (Kashdan and Rottenberg, 2010; Kashdan et al., 2020). Individuals with a broader set of coping strategies, greater variability in coping approach, and more effective coping skills demonstrate more effective behavioral changes over time. Notably, effective coping involves both the learning of new coping strategies and the ‘unlearning’ of others that have proven ineffective. The engagement in such behavioral learning and ‘unlearning’ involves inherent discomfort and broadening of behavioral coping approaches, for which greater psychological flexibility and acceptance of discomfort in the service of learning are critically important (Tabibnia, 2020).
Psychological flexibility is inherently multifaceted and, accordingly, may be achieved through different psychological and behavioral changes across individuals (Ruork et al., 2022). Psychological flexibility involves an individual’s ability to adaptively respond to contextual demands in the service of valued actions, often by tolerating distressing experiences, being present focused, and cultivating flexible response patterns (Kashdan and Rottenberg, 2010). It may be immediately apparent from contemporary definitions of psychological flexibility that several important subprocesses facilitate higher-order flexibility in responding. Individuals who lack clarity in their values, who are avoidant of aversive internal experiences, who have trouble staying present focused, and who exhibit a narrow range of behavioral responses may all be viewed as inflexible, albeit in different ways. Because all behavioral responses may be judged effective or not based on context-related goals, examining specific patterns of behavior is sometimes less useful than assessing the capacity to generate flexible response patterns when needed. Examples include the use of amplifying anger, which may be injurious in some interpersonal relationships but necessary when confrontational interactions are warranted in some work-related settings. Similarly, the flexible generation of coping strategies may be beneficial for individuals who respond in a rigid manner but function to reduce mindfulness for individuals already disconnected from important interpersonal relationships. Much of this work and associated randomized trials was developed by Lynch and colleagues Multiple types of coping are required to adapt effectively to aging and cultivating different coping strategies may take different forms for different individuals (Lynch, 2018; Lynch et al., 2020).
Perhaps not surprisingly, recent conceptual frameworks examining psychological resilience have begun to focus on the importance of regulating affect as a critical component of learning new coping skills and psychological resilience (Tabibnia, 2020; Troy et al., 2023). Affect refers to the experience of feeling emotions and affective processing lies at the intersection of neurobiological and psychological factors (Troy et al., 2023). Individuals still early in the course of neurodevelopment exhibit an exaggerated affective response and difficulty regulating their affect (e.g., lowering arousal following a startle), as indicated by taking a longer time to self soothe (Kittel et al., 2017; Mamrot and Hanc, 2019; Stalnacke et al., 2019). Older adults, or adults who have experienced a neurological insult, also experience degradations in their ability to regulate affect but in a more variable and qualitatively distinct manner (Berry et al., 2019; Schweizer et al., 2019; Cotter et al., 2020). For many older individuals, their affective experiences are characterized by lower reactivity, a slower time course of increasing emotion (relative to dampening reactivity, as is the case with younger individuals), and more diverse and effective set of coping skills to modulate affect (Salehinejad et al., 2021; Stretton et al., 2022). As reviewed below, these changes track broadly with well-characterized of development and disruption to white matter pathways regulating frontal-subcortical pathways of affective control (Cotter et al., 2020; Shafer et al., 2020), most notably the interaction between areas within the salience and executive-control networks. Put more simply, affective differences broadly group into individuals who experience difficulties (1) up-regulating positive affect, (2) down-regulating negative affect, and (3) with a tendency to ruminate (Tabibnia, 2020). For clinical purposes, these can be thought of as differences that require (1) strategies to increase behavioral activation through up-regulating dampened areas within frontal-subcortical rewards systems pathways (Crowther et al., 2015; Alexopoulos et al., 2016; Douma and de Kloet, 2020; Tabibnia, 2020), (2) strategies to enhance the efficiency of relaxation, experiential acceptance, and distress tolerance that are mediated by limbic-PFC integrated brain structures (e.g., amygdala and insular cortex) (Fonzo et al., 2017; Hermann et al., 2017; Addicott et al., 2018), and (3) strategies to get individuals ‘out of their head(s)’ by increasing mindfulness, salience, and transcendence of self (Taren et al., 2017; Demos McDermott et al., 2019).
2.1 Individual differences in cognitive control and emotion regulationAs noted above, self-regulation encompasses both cognitive and affective mechanisms by which individuals pursue their goals in the face of life’s challenges. Although often not integrated into the geriatric literature, there are well recognized differences in how cognitive control influences and motion regulation strategies. Individual differences broadly track with three types of cognitive control: working memory updating, response inhibition, and set-shifting (Hendricks and Buchanan, 2016; Dreisbach and Fröber, 2018; Pruessner et al., 2020). From the neuropsychological literature, these cognitive control processes overlap at a population level but are often different at an individual level (Pruessner et al., 2020). Individuals with deficits in working memory may include adults characterized by inattention or distractibility. This differs from individuals who have response inhibition difficulties, who are typically characterized as more impulsive (Drossel et al., 2023). Similarly, distractible or impulsive individuals often differ from those with set shifting difficulties, who are often characterized as perseverative and exhibiting a ‘stickier’ personality style (Alexopoulos et al., 2015; Voon, 2015). Working memory and updating is more reliant on dorsolateral PFC areas, inhibitory control on the anterior cingulate and ventromedial PFC, and perseveration results from disruptions to posterior cingulate and dlPFC brain regions (Reineberg et al., 2022). In essence, the type of executive control difficulty may vary substantively between individuals and overlap with affective control brain networks (Langner et al., 2018), leading some thought leaders to propose that conceptualizing interrelationships between executive and affect control is best conceptualized as an integrated self-regulation system (Langner et al., 2018).
A related area concerns how individuals with different cognitive profiles tend to benefit differentially from distinct self-regulation strategies, including the use of emotion regulation vs. behavioral regulation. As reviewed in detail elsewhere (Pruessner et al., 2020), effective emotion regulation necessitates flexibility in the use of several different regulation skillsets: (1) strategy stopping or switching, (2) strategy maintenance, and (3) monitoring. Individuals who are less cognitively flexible may not use an adequately variable set of coping responses to help manage daily stressors, failing to either initiate new coping strategies or switch from ineffective ones (Kato, 2022).
Similarly, individuals who are more concrete or with reduced working memory lack the ability to accurately appraise whether a selected coping skill is working, so that effective strategies can be maintained and ineffective strategies modified or eliminated (i.e., referred to as the shielding-shifting dilemma) (Goschke and Bolte, 2014). Individuals who tend to engage in cognitive reappraisal strategies (e.g., thinking about their situation in new ways to reduce distress) may find it necessary to switch to distraction strategies in high-intensity emotional situations (Birk and Bonanno, 2016).
To give several widely studied interactions between cognition and affect for effective self-regulation, individuals with lower working memory abilities have a more difficulties engaging cognitive reappraisal (which requires substantial working memory) in order to regulate their affective responses (Schweizer et al., 2013). Not surprisingly, negative affect has a much greater overlap and impact on working memory updating than it does on other cognitive control domains (Price and Duman, 2020; Pruessner et al., 2020). Individuals who are more depressed, anxious, or avoidant tend to experience greater deficits in working memory than their ability to inhibit impulsive behavior (Saleh et al., 2017; Schweizer et al., 2018; LeMoult and Gotlib, 2019). Similarly, individuals with lower inhibitory control may have more difficulties inhibiting pre-potent impulses, particularly when they are experiencing acutely higher levels of psychological distress, sleep deprivation, or physical fatigue (Hall and Fong, 2015; Evans et al., 2016).
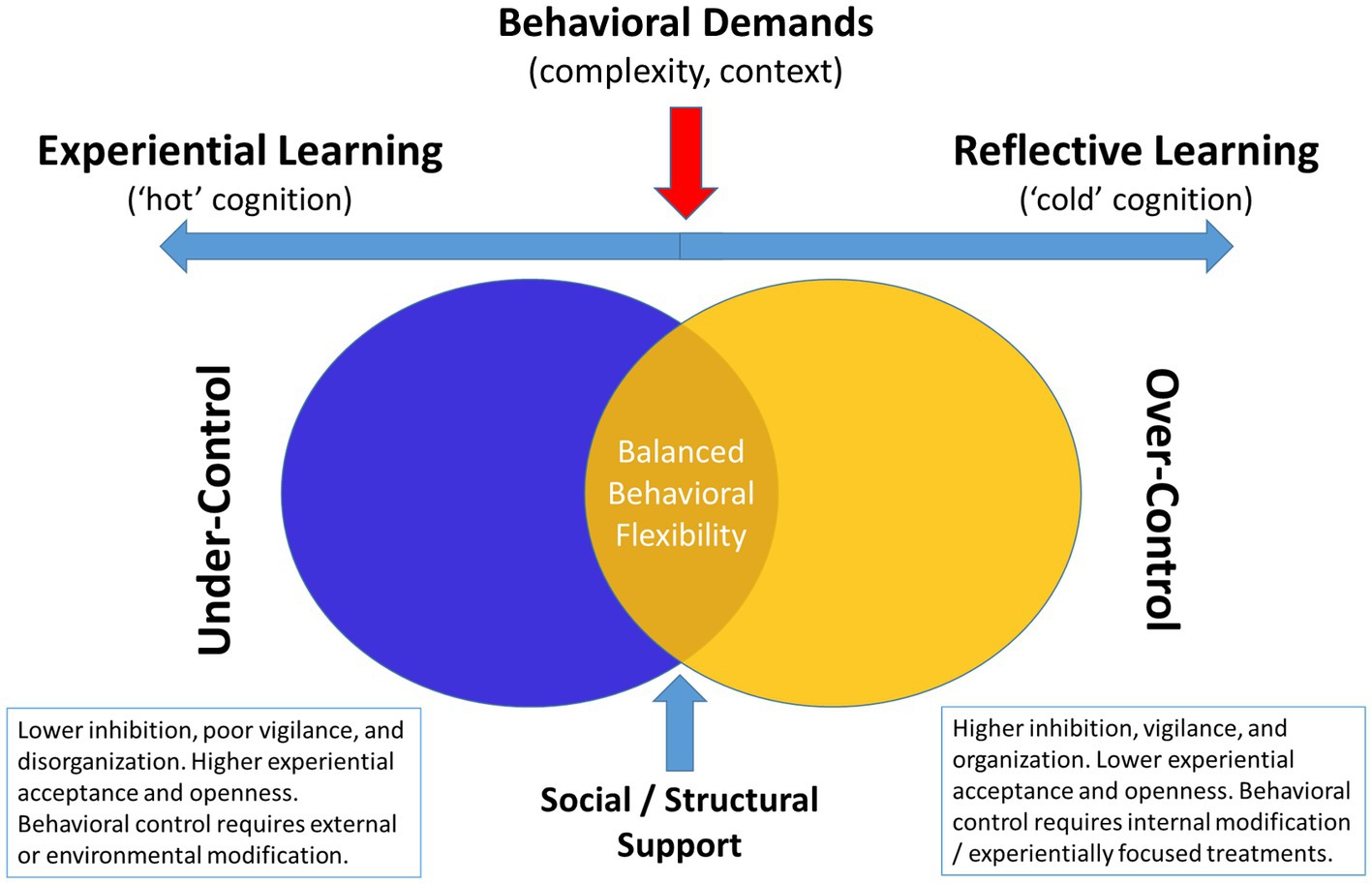
2.2 Age-related differences in self-regulatory stylesWhile there is a substantial literature on each of the various components of self-regulation in healthy adults, there are surprisingly few discussions of how self-regulation changes as we age. Differences between older and younger individuals emphasize an important and under-characterized pattern of self-regulatory functions. Older individuals are often more effective in their coping responses due to a wider behavioral repertoire of coping skills, a greater depth of experience using those coping skills, and an ability to use different coping skills across different contextual settings. Therefore, while they may experience some neurobiological inefficiencies in regulating affect, they are better able to adjust their behavior to compensate for this. Put simply, older individuals coping effectively are better able to regulate their behavior to meet contextual demands, exerting greater behavioral control when needed and more effectively using psychological acceptance approaches in situations where they have limited control. Individuals constantly using control-based coping approaches may have a greater likelihood of developing disorders characterized by ‘over-control’ (e.g., disordered eating, borderline personality disorder, obsessive compulsive disorder) (Ben-Porath et al., 2020; Baudinet et al., 2021; Isaksson et al., 2021), whereas individuals who fail to exert control when its needed may risk developing conditions characterized by disinhibition, poor behavioral regulation, or social disconnection (Burnell et al., 2022; Jones and Schuz, 2022; Wang et al., 2023). Ultimately, adaptive functioning requires flexible up- and down-regulating of self-control impulses depending on the context (Figure 1). A critical limitation in the existing literature is tailoring interventions in order to better understand how different phenotypic patient presentations impact how individuals more effectively modulate self-regulatory functions.
Figure 1. Conceptual diagram linking cognitive and psychological profiles to behavioral over-vs-under control style.
An important but underemphasized aspect of independent aging is the prognostic association between cognitive functioning and preserved self-management abilities (Mace et al., 2017). Although dementia is typified by impairments in memory, impairments in executive functioning are far more predictive of loss of functional abilities and impaired IADLs, even among individuals with comorbid memory impairments (Colón-Emeric et al., 2013; Mansbach and Mace, 2018). Notably, an emerging body of evidence suggests that elements of psychological functioning, including personality factors and associated emotion regulation abilities, interact with cognitive functioning to predict independence (Roy et al., 2016; Brothers and Suchy, 2021). For example, individuals who exhibit greater trait levels of openness to experience and lower levels of neuroticism appear to better navigate the complexities of aging compared to their counterparts (Williams et al., 2010; Hayward et al., 2013; Dermody et al., 2016; Mertens et al., 2022). Similarly, individuals who more frequently engage in ineffective coping behaviors, which may deplete self-regulatory capacity, show greater executive functioning lapses during daily life (Brothers and Suchy, 2021). Taken together, it is likely that impairments in executive functioning interact dynamically with elements of emotional functioning to influence older adults ability to successfully retain independence.
Understanding the interaction between cognitive capacity and psychological functioning is particularly important because executive functioning is critical both for preserving independence and to optimal engagement in health behaviors protecting the brain from future decline in cognitive abilities (Daly et al., 2014; Allan et al., 2016). Habitual engagement in physical activity, healthy dietary habits, medication adherence, and vascular risk reduction are all strongly influenced by the ability to regulate one’s behavior (e.g., self-organize, inhibit untoward impulses, self-motivate) (Reimann et al., 2020; Appelhans et al., 2021). In a recent review of prospective studies linking executive function to health behaviors, the authors reported that executive function deficits were linked to every health behavior outcome (e.g., physical activity, dietary health, medication adherence, tobacco use, etc.) with wide variation in the particular executive function component examined (Reimann et al., 2020). For example, although inhibitory control was frequently linked with poor health behaviors, cognitive flexibility, working memory, planning, and problem-solving were also predictive for other behaviors. Recent data has suggested that the three key subdomains of cognitive function representing critical capacities for maintaining healthy lifestyles on an individual level are inhibitory control, cognitive flexibility/shifting, and updating/working memory (Allan et al., 2016).
A critical component of effective coping involves behavioral flexibility, which is closely related to, and partially constrained by, levels of executive function (Kato, 2021). For example, even among individuals without cognitive impairment there is wide variation in their premorbid levels of cognitive flexibility, inhibitory control, and updating/working memory (Miyake et al., 2000a,b). Lower levels of functioning in any of these subdomains has been linked to worse health maintenance behaviors, including medication adherence (Stilley et al., 2010), weight management (Gowey et al., 2021), and physical activity (Hall et al., 2008). Even subclinical, relative weaknesses within these three subcomponents of executive function alone can result in individuals who will tend to show response patterns notable for being more concrete, impulsive, or distractable, all of which intuit different methods of management (e.g., coping skills training with strategy development, environmental modification, and use of reminder systems). With age-associated decrements in cognition, the ability to flexibly cope with new situations may be constrained as these skills become less efficient (Park and Reuter-Lorenz, 2009; Oberlin et al., 2016; Aschenbrenner et al., 2023), creating a potentially ‘vicious cycle’ by which worsening executive function leads to poorer behavioral regulation, which further degrades executive functioning resources (Morris et al., 2015; Grech et al., 2019).
2.3 Regulating behavior over time: temporal self-regulation and lifestyle maintenanceAs the sections above demonstrate, there are many aspects of how self-regulation changes during the aging process that have yet to be fully delineated and applied. A critical gap in the current literature linking chronic disease management to functional independence is the lack of sustained lifestyle maintenance over time (Rhodes and Sui, 2021). The vast majority of individuals have difficulty maintaining behavior changes over time, such as sustaining physical activity levels (Lachman et al., 2018). Many individuals show chronically sedentary levels of activity and even among those who engage in a lifestyle intervention program, ≥75% tend to show reversion to their sedentary habits over time (Graham et al., 2020). Rates of poor lifestyle maintenance are also found among individuals who report motivation and intentions of engaging in exercise and dietary change, suggesting that these low rates are not exclusively due to lack of motivation (Huang et al., 2020). Indeed, this widely recognized discrepancy between intentions and action has been discussed in detail elsewhere, but appears partially attributable to individual differences in neurobiological factors and also to wide differences in contextual and environmental characteristics that act as facilitators or barriers to optimal engagement (Paganini et al., 2022; Dorina et al., 2023; Wang et al., 2023).
An emerging framework with both predictive and explanatory potential for the lack of lifestyle engagement across different groups is Temporal Self-Regulation Theory (Liddelow et al., 2022; Wang et al., 2023). This theory incorporates both psychological factors and neurobiological factors to explain high variability in success with lifestyle changes. Specifically, TST incorporates information on health behavior beliefs and current intentions with both historical data on pre-potency of habits and self-regulatory capacity as influencing ultimate behavioral outcomes. Components studied within this theoretical framework include the pre-potency for activity engagement, the degree to which the behavior has a prior habit formation, and the degree of executive functioning, which impacts both inhibitory control and also self-regulation of behaviors of differing complexities and across different contextual demands (Dorina et al., 2023). For example, behaviors of greater complexity or that are being engaged in within new contexts are inherently more prone to lapses. Due to this greater amount of ‘behavioral friction’ (Wood and Neal, 2016), it is not surprising that only highly motivated individuals are successful in adopting new, complex behaviors across contexts (Dorina et al., 2023). In addition, prior meta-analytic and clinical studies (Wang et al., 2023) have demonstrated that greater age and poorer executive function moderate the association between intentions and action, with individuals of greater age and lower executive function demonstrating greater discrepancies between their intended behaviors and actual actions (Dorina et al., 2023).
The importance of temporal self-regulation may be particularly important for aging adults, many of whom may be attempting to adopt new health habits following a new medical diagnosis or related health concerns. Many individuals actively engaging in healthy lifestyle habits, or with a prior history of such practices, will be more effective in their adoption of new behavioral repertoires in order to cope with their new chronic medical conditions. For these individuals, providing structural support in the form of supervised rehabilitation or peer-support maybe more than adequate to help facilitate their success with reengaging in health behaviors. In contrast, for individuals being encouraged to learn new health habit behaviors they will by definition be asked to engage in (1) complex behaviors that are (2) in different contexts that they are not familiar with. Perhaps not surprisingly, the most common time for dropping out of lifestyle intervention protocols is within the first few weeks of treatment, when participants are being asked to make the most active and disruptive changes (Bentley et al., 2021; Collins et al., 2022). In parallel, individuals with greater comorbidity burden (Heydarpour et al., 2015; Viken et al., 2019) and lower levels of self-efficacy are the most likely to drop out prior to completing rehabilitation, during the initiation phase of behavior change (Collins et al., 2022). In contrast, individuals with poorer executive function, lower levels of support, and less access to structural resources are at greatest risk for failing to maintain behavior changes over time, regardless of their initial success (Annesi et al., 2016; Mazzoni et al., 2021; Paganini et al., 2022). For this reason, recent reviews on physical activity maintenance stress the importance of flexible response patterns over time and dynamic coping approaches as critical predictors of maintenance (Rhodes and Sui, 2021). Similar findings have been reported for weight loss maintenance, with both psychological (e.g., self-efficacy) and cognitive factors facilitating self-regulatory behaviors serving as important predictors of ultimate success (Varkevisser et al., 2019; Eykelenboom et al., 2020; Roordink et al., 2022). In contrast, basic demographic factors (e.g., age, biological sex, race/ethnicity, socioeconomic status, etc.) were not predictive of weight maintenance (Varkevisser et al., 2019).
The importance of maintaining intact cognitive functioning is particularly relevant for older adults seeking to maintain health lifestyle changes, as emerging evidence suggests a bidirectional relationship between executive function and lifestyle engagement, creating a ‘virtuous cycle’ of increased physical activity and neurocognition (Daly et al., 2014; Allan et al., 2016). Although causal associations between cognitive factors and behavioral outcomes are complex and likely multifactorial (Danks and Davis, 2023), available evidence strongly supports the assertion that better cognitive function predicts healthier lifestyle maintenance, that lifestyle predicts better cognitive function, and that, even in the context of randomized trials lasting several months, treatment-related cognitive changes may prospectively predict behavior changes. Specifically, (1) individuals with greater executive function demonstrate greater capacity for maintaining healthy lifestyles over time (Gettens and Gorin, 2017; Kulendran et al., 2017; Audiffren and Andre, 2019; Butryn et al., 2019; Pfeffer and Strobach, 2021; Walo-Syversen et al., 2021), (2) healthier lifestyles (e.g., greater physical activity and lower obesity) associate with higher executive functions prospectively (Eskes et al., 2010; Best et al., 2015; Lu et al., 2016), and (3) treatment-related improvements in executive function predict greater maintenance of behavior changes over subsequent follow-up assessments (Baruth and Wilcox, 2014; Best et al., 2014; Allan et al., 2016; Audiffren and Andre, 2019). The Taken together, existing evidence suggests that intact executive functioning could be conceptualized as a necessary but not sufficient component of behavioral self-regulation (Allan et al., 2016; Gettens and Gorin, 2017; Butryn et al., 2019; Reed et al., 2020; Pfeffer and Strobach, 2021; Szabo-Reed and Donnelly, 2021).
2.4 Personality and self-regulatory behavior change techniquesSelf-regulation engages a number of stable individual differences or personality variables. For example, using the five factor model of personality (openness, conscientiousness, extraversion, agreeableness, and neuroticism), personality facets demonstrate consistent associations with broad health behaviors in population studies (Bogg and Slatcher, 2015). Individuals who are more conscientious and less neurotic have been shown to have lower risk of mortality and developing chronic medical conditions, although the linkages between personality and health outcomes continue to be elucidated. Recent work suggests that is likely personality and health outcomes is linked through ‘assimilative’ processes, with personality factors tending to predict behavioral response pattens and the likelihood of influence by situational facilitators/barriers (McCrae and Sutin, 2018). For example, individuals who are more neurotic and less open to experience exhibit higher levels of anxiety sensitivity (Wauthia et al., 2019) and experiential avoidance (Mohammadkhani et al., 2016), which may lead them to engage in avoidant behavioral patterns (Sirois, 2015; Sirois and Hirsch, 2015).
A large and diverse literature base suggests that individuals are naturally inclined toward different though common behavioral coping processes (Carver and Connor-Smith, 2010). These can be broadly grouped into action oriented or active coping or avoidant coping through behavioral disengagement of varying forms. Individuals who are more conscientious and open to experience tend to cope in a more approach-oriented fashion. In contrast, individuals with higher levels of neuroticism are more likely to disengage and engage in avoidant coping (Mohammadkhani et al., 2016), and as a corollary, individuals who are more agreeable and conscientious are less likely to disengage (Carver and Connor-Smith, 2010), though may differ in the degree to which they pursue action-oriented coping strategies. Similarly, trait-level individual differences in affective intensity and positivity predispose individuals toward a greater tendency toward behavioral control, behavioral approach tendencies, and avoidance (Segerstrom and Smith, 2019). In parallel, studies of individual differences in self-regulatory function suggest three broad behaviors most closely associated with ‘persistence’ (Moshontz and Hoyle, 2021), each facilitated by overlapping but distinct brain networks. As described by Hoyle and colleagues, these include ‘resisting, recognizing, and returning.’ These track closely with the three cognitive control domains noted above (inhibitory control, cognitive flexibility, and working memory/updating). These neurobehavioral functions in turn are typically associated with differential aspects of the frontal-subcortical brain networks, with inhibitory control tracking closely with SN regions including the ACC (Tuulari et al., 2015), cognitive flexibility with posterior cingulate functions (Wan et al., 2015), and working memory associated with dorsolateral prefrontal cortex function (Mars and Grol, 2007; Lantrip et al., 2019).
In contrast to cognitive functioning, some aspects of personality tend to remain relatively stable over time, vary widely across individuals, and have been associated with different elements of executive functions (Rike et al., 2018; Kemps et al., 2020; Van Malderen et al., 2020). Differences in personality also intuit different behavioral intervention approaches (Ma et al., 2021; Alqahtani et al., 2022). Individuals with higher levels of conscientiousness tend to exhibit better planning and organizational abilities, are more vigilantly engaged with healthy lifestyle habits, and tend to engage in more self-monitoring behaviors. However, this relationship may be constrained among individuals who are also highly neurotic and you have lower levels of trait openness, for whom a more ritualized and rigid approach to coping may develop overtime (Bonanno and Burton, 2013). Conversely, individuals who have higher levels of trait openness may engage in more flexible coping patterns. But in combination with low levels of conscientiousness they may fail to adequately plan for or update these coping approaches for workability within changing life circumstances and therefore fail to adequately utilize them. It is therefore important to consider both personality and cognitive abilities when considering effective behavioral changes.
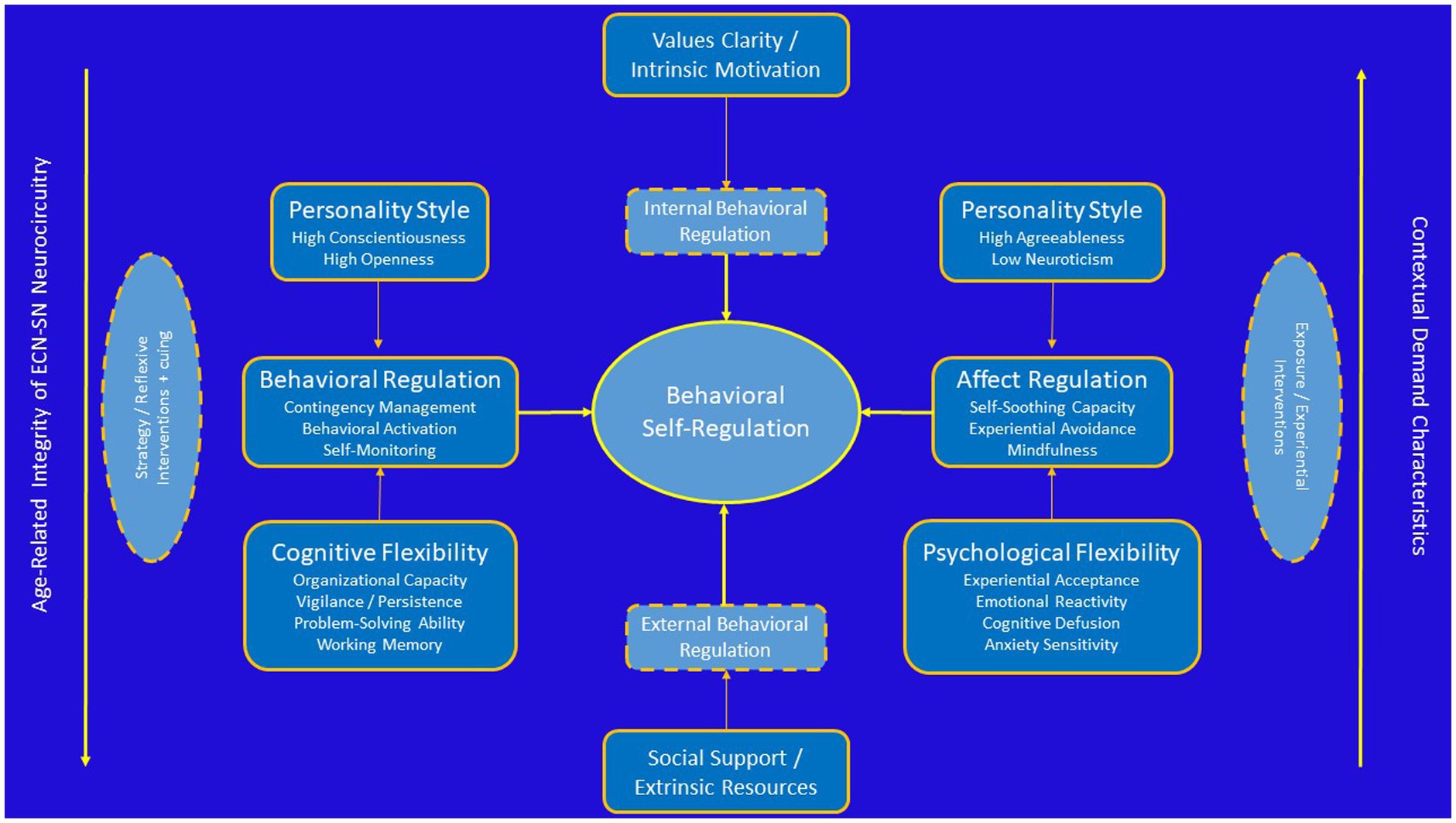
As noted earlier, individuals may be naturally predisposed toward several different action tendencies and these likely have a strong evolutionary intuition. Individuals who are more neurotic and have less openness to experience may be less likely to make major behavioral changes that require them to engage in what is perceived as riskier behaviors out of their comfort zone. For individuals who could benefit from weight loss, this often means greater friction embracing new behavioral patterns at the expense of familiarity with older ones, however ineffective. Similarly, Individuals more open to experience and conscientious may be more effective at making large behavioral changes with the recognition (through self-monitoring) that such changes are needed. In both cases, behavior could likely have an impact on the ability to make behavioral changes in response to changing health-related contingencies. At the same time, some elements of personality may adversely impact the ability of an individual to organize their lives in the service of self-management toward behavioral goals. Among chronic disease populations, individuals who are more conscientious, agreeable, open to experience, and less neurotic are more likely to maintain behavioral changes relative to their counterparts (Jerant et al., 2009, 2010, 2011). In addition, individuals exhibit more control over their own behavioral routines (Knittle et al., 2020) also tend to experience greater affective benefits from health behaviors, particularly physical activity (Ekkekakis et al., 2005). Such phenotypic measures, while not directly associated with personality variables, may provide important predictive information to tailor preventive interventions (Bryan et al., 2017). Emerging data suggest that affective responses are the critical mechanism linking diverse factors such as personality and cognitive functioning to long-term health outcomes (Leger et al., 2021) and that affective responses to physical activity are a robust predictor of physical activity maintenance (Figure 2; Boyle et al., 2019; Pfeffer and Strobach, 2021; Dunton et al., 2023). Taken together, available evidence increasingly points to the need for understanding of functional mechanisms by which behavior change techniques associate with health behavior changes, including an examination of interactions across external, internal reflective, and internal affective domains (Michaelsen and Esch, 2022).
Figure 2. Conceptual diagram linking individual differences in personality and cognitive function to regulation of health behavior changes.
2.5 Neurobiological underpinnings of self-regulationThe construct of self-regulation has been widely used by cognitive neuroscientists to understand complex patterns of neural activity in both healthy and impaired populations. Self-regulatory capacity appears to overlap systematically with markers of frontal-subcortical integrity, efficiency of network activation within the salience (SN) and executive control networks (ECN), and with behavioral markers of executive function (Stubberud et al., 2020; Fournier et al., 2021; Kim and Han, 2021; Smith and Merwin, 2021). Available evidence suggests that preserved cognitive flexibility through balance of highly interconnected cortical systems is critical for resilient self-regulatory function, with an anterior locus critical for behavioral implementation activation (SN) and a posterior locus critical for cognitive reflection and behavioral evaluation (ECN). In addition, the ability to self-regulate affect in the service of implementing behavioral response patterns appears to rely on critical interconnections between default mode network (DMN) and SN brain regions responsive to contextual cuing and experiential training (Kaiser et al., 2016; Walsh et al., 2019; Nagy et al., 2020; Pisoni et al., 2021). Among individuals with behavioral phenotypic evidence suggesting dysfunctional, hyporesponsivity within reward-system pathways (e.g., anhedonia, psychomotor slowing, low vigilance, poor sequencing), behavioral activation approaches appear most effective (Detloff et al., 2020; Nagy et al., 2020). Among individuals with phenotypic evidence suggesting hyperresponsivity within reward-system pathways (e.g., elevated startle response, ruminative, experientially avoidant), experiential interventions with an exposure component appear most effective (Hermann et al., 2017; Fitzgerald et al., 2018; Stojek et al., 2018). It has been widely documented that hyperactivation within SN brain regions strongly associated with diverse anxiety disorders and elevated psychological distress (Rabany et al., 2017). Alterations in DMN connectivity, in contrast, have been widely demonstrated among individuals with depression, pathological rumination, and ADHD, among other disorders. Finally, alterations within the ECN have been implicated in a multitude of clinical disorders, including mild cognitive impairment (Xu et al., 2020). Importantly, the ability to shift behavior flexibly in response to contextual demands and update behavioral planning appears to track closely with interactions within the SN and ECN systems, with hyperactivation resulting in behavioral rigidity, hypoactivation resulting behavioral disengagement, and behavioral regulation resulting from efficient and context-dependent shifting between both systems.
Notably, these distinct neural phenotypes track closely with widely known early neurodevelopmental differences among young children that track across three primary dimensions: emotional intensity, effortful control, and extraversion (Cooke et al., 2017; Brainstorm et al., 2018; Salvatore et al., 2020; Ip et al., 2021; Karlsson Linner et al., 2021; Munn-Chernoff et al., 2021). Emotional intensity (e.g., neuroticism) encompasses trait-level predispositions to experience emotions more intensely than others. Effortful control (e.g., executive function) encompasses a child’s ability to sustain attention over time, their capacity for impulse control, and their predisposition toward mind-wandering and internally directed thought processes (e.g., rumination). And finally, extraversion is the child’s predisposition toward seeking social relationships. These findings track with evidence from pediatric, adolescent, and young adult studies demonstrating elevated SN activity and resultant hyperconnectivity between areas in the SN-DMN associate with higher levels of neuroticism. Similarly, greater activation patterns within the ECN and connectivity between the SN-ECN appear to associate with higher effortful control levels.
There are at least two useful extensions of behavioral interventions and phenotypic variations within them that can be Better appreciated using this overarching framework as a conceptual reference. First, several of the areas within the SN and ECN systems show wide variation both in their initial myelination during development and in their normative disruptions associated with aging. This has been referred to as consistent with a ‘last in, first out’ pattern of disruption, where areas that myelinate the latest in adolescent development Appear to also be the most sensitive to age-related changes, particularly those secondary to cardiovascular disease (e.g., hypertension, obesity, diabetes), which are also highly prevalent. As an example, Areas in the dorsal lateral prefrontal cortex with important projections to the anterior cingulate are last to myelinate and tend to associate behaviorally with inhibitory control, such that younger adults without fully developed connections in these circuits have greater difficulty with behavioral inhibition. In older adults, age-related disruptions within these circuits tend to associate with slower processing speed, even though cognitive strategies tend to remain robust. In other words, the benefits of younger adults in processing speed are offset by lack of behavioral strategies, whereas the opposite pattern is true in older adults. Second, because behavioral phenotypes can result from multiple different underlying causes, understanding core neurocircuitry that mediates behavioral changes, either with normative maturation or in the context of intervention training, provide crucial insight into behavioral intervention strategies.
Several other principles from behavioral training paradigms examining neuroplasticity mechanisms are also relevant to understand the role of behavioral training on brain changes. These have been reviewed in detail elsewhere and are summarized briefly here (Kleim and Jones, 2008). First, areas that activate together tend to develop reciprocal synaptic connections, more commonly referred to as the Hebbian principle that ‘what fires together, wires together.’ Second, brain circuits that go underused become disrupted or even atrophied over time (‘use it or lose it’) and can be improved through training-associated usage (‘use it an improve it’). Improvements in brain circuitry are not monolithic, however, and will occur over different time frames depending on age, premorbid neurological injury, and the timing of intervention. Third, several key elements of behavioral training appear to have an important impact on neuroplasticity changes, including the repetition and intensity of training, the specificity of training, and the presence of interfering behaviors. Finally, training in one modality may enhance or inhibit gains in other domains.
2.6 Intermediate phenotypes of cognitive and psychological functionHow can this self-regulation perspective help to identify commonalities across aging individuals? Cognitive and psychological functioning may converge to result in different affective phenotypes (Tabibnia, 2020). For example, a recently proposed tripartite model of affective resilience suggests three different phenotypic profiles with preexisting vulnerabilities based on differences in efficiency within distinct neuroanatomic functional networks. Within this framework the three profiles broadly corresponded to coping styles that required (1) up-regulation of positive affect, (2) down regulation of negative affect, and (3) strategies to get ‘out of your head’ by transcending the self (Tabibnia, 2020). These broad behavioral phenotypes also correspond to specific neuroanatomical system targets, specifically (1) up-regulating mesostriatal reward system pathways, (2) down-regulating autonomic/amygdalar reactivity within limbic brain regions, and (3) down-regulating default mode network pathways. Similarly, these broad phenotypes intuit different biobehavioral treatment strategies, including but not limited to (1) physical activity, (2) exposure therapies, and (3) mindfulness-based approaches.
Although phenotypes of resilience can no doubt be augmented by biobehavioral treatment approaches, there is strong evidence that genetic predisposition explains a substantial amount of our phenotypic ‘set point’, tending to be present from an early age and tracking within families. Decades of work across multiple disciplines has robustly demonstrated that personality and cognitive functioning have a high degree of heritability and only modest levels of overlap (Malanchini et al., 2019; Friedman et al., 2021; Krueger et al., 2021). For example, studies examining heritability estimates for cognitive abilities facilitating intact inhibitory control, cognitive flexibility, and other executive functions suggest that this capacity has a very high degree of heritability (Friedman et al., 2008), much higher relative to heritability estimates for general intelligence, for example (Freis et al., 2022; Gustavson et al., 2022). Although various aspects of executive functioning are amenable to improvement with behavioral training modalities (e.g., working memory, inhibitory control), individual differences in executive functioning are nevertheless ‘tethered’ to premorbid capacity even after training, suggesting substantial variability across individuals in this critical behavioral domain.
Similarly, several canonical personality factors have a high degree of heritability, including trait levels of neuroticism and openness (Jang et al., 1996). Although the degree of heritability for personality traits is somewhat lower than that observed for executive functioning, this may partly obscure the degree to which core temperamental elements of personality development, such as anxiety sensitivity, may play (Wauthia et al., 2019). In both cases, evidence increasingly suggests a vulnerability model of genetic transmission, in which predisposing vulnerabilities in cognitive and psychological phenotypic markers confer risk of developing an array of subsequent clinical disorders and with adaptive functioning more broadly (Bagby et al., 2008; Mertens et al., 2022). Moreover, individual differences in trait levels of openness, conscientiousness, and neuroticism appear robustly predictive of health behavior engagement: individuals who are more conscientious, open to experience, and lower in neuroticism, are much more likely to exhibit consistent health behaviors relative to their more neurotic and experientially avoidant counterparts. While the specific behavioral elements of heritability remain an active area of research, the robust association between personality profile and behavioral health outcomes provides an opportunity for treatment tailoring.
The importance of personalizing health behavior interventions it is perhaps most evident when examining the great degree of heterogeneity in approaches to change health behaviors. Within the growing Science of Behavior Change (SOBC) framework, more than 90 different behavioral approaches were identified that could be further reduced to 16 clusters. Self-regulatory behaviors represented within these cores included self-monitoring, goal-setting, and ‘down-regulating negative emotions’ (Wilson et al., 2020). Notably, a three-pronged approach to behavioral regulation has been noted by personality researchers as well, underscoring the collective importance of resisting, recognizing, and returning to goal-related pursuits (Moshontz and Hoyle, 2021). While the importance of each components will be intuitive to behavior change success, they rely on somewhat distinct neuroanatomical systems and will be harder or easier to engage with based on personality profile. Effective goal setting, for example, is at least partly dependent on selecting from a diversity of behavioral approaches and therefore partly dependent on personality domains such as openness. Individuals who are more open may not necessarily be effective at self-monitoring, which is more dependent on trait levels of conscientiousness. And the ability to modulate emotional reactivity is known to relate to trait levels of neuroticism. These three broad behavioral clusters (resisting, recognizing, and returning) can also be broadly mapped onto activation patterns within SN, ECN, and DMN networks, underscoring the importance of distinguishing motivational from cognitive strategy deficits when developing behavioral interventions (Berkman, 2018a,b).
3 Behavioral training modalities for self-regulationSelf-regulatory functioning may be best understood as a transdiagnostic behavioral process given its importance in facilitating multiple, disparate behaviors among adults (Sloan et al., 2017; Romer et al., 2021). Broadly speaking, impairments in the capacity to effectively regulate one’s behavior (Cahn-Weiner et al., 2000; Kiosses et al., 2001; Best et al., 2015; Hall and Fong, 2015; Mansbach and Mace, 2018) or effectively regulate one’s emotion response (Gyurak et al., 2012; Etkin et al., 2013; Zhang et al., 2019; Cotter et al., 2020; Troy et al., 2023) in the service of personally valued pursuits may result in an array of bad outcomes (Sirois et al., 2015; Amlung et al., 2017; Kauffman et al., 2022a,b). Behavioral regulation may be conceptualized as having a critical reliance on executive function, with intact executive function serving as a necessary but not sufficient capacity that may change with aging (Cotter et al., 2020; Hoyt et al., 2020), chronic disease burden, or neurological insult (Rike et al., 2014, 2018). Multiple sub-domains of executive function have direct and intuitive influences on behavioral regulation, including inhibitory function, problem-solving ability, learning/behavioral ‘updating’ to environmental or contextual contingencies, shifting attention, and maintaining vigilance over time (Moshontz and Hoyle, 2021). Importantly, many of these skill sets rely critically on the integrated function of dorsolateral and posterior frontal lobe regions (discussed in detail below), which are important for reflective analysis, pattern recognition, and strategy selection. Individuals who cannot recognize and adapt to functionally similar behavioral barriers (e.g., diverse outcomes resulting from poor time management, goal-setting, or self-monitoring) will tend to repeat the same mistakes in a perseverative fashion. Deficits in problem-solving abilities therefore often result from deficits in the ability to mentally abstract, integrating personally-relevant visual information for the purposes of self-monitoring, and generate alternative strategies to deal with complex problems. Such deficits are often treated using reflective strategies, goal-setting approaches, and collaborative self-management strategies (e.g., top-down). In addition, recognizing impulsive tendencies and resisting impulsive behavioral responses typically involve recognizing the cues and using cognitive control strategies for re-interpretation, again suggesting top-down strategy use that is partly contingent on accurate monitoring.
In contrast to more analytical, reflective approaches, several aspects of self-regulation involve persisting in the face of adversity. While these behavioral responses may be subsumed under executive function, these typically involve subdomains that include vigilance and effective sequencing of information (e.g., re-engaging repeatedly). Maintaining behavioral vigilance is typically facilitated by bottom-up behavioral strategies, which may involve sustained maintenance of undivided attention and self-motivation strategies to maintain engagement. Because these behaviors are subserved by anterior and paralimbic brain regions, including the anterior cingulate cortex, there is a high degree of emotional overlay facilitating persistence. Individuals better able to regulate emotional distress are therefore better able to persist in their goal pursuits.
Importantly, different aspects of self-regulatory function are leveraged by different intervention approaches. Many cognitive rehabilitation paradigms, for example, focus on strategy and process, whereas many ‘third-wave’ behavioral interventions focus on affect regulation through mindfulness and priming of personal values. One need not look far to appreciate the far-reaching importance of intact self-regulation, as impairments in self-regulatory capacity have been shown to predict substance abuse outcomes, medication non-adherence, impairments in activities of daily living, obesity, and impaired behavioral compliance writ large. A key conceptual distinction emergent from contemporary process-based therapies is the recognition that the ability to regulate one’s behavior is dependent on intact functioning within several critical domains, including the ability to intentionally flexibly modulate attention (‘cognitive flexibility’) and the ability to regulate or respond effectively to affectively distressing feelings (‘psychological flexibility’). Moreover, both processes are closely related to and impacted by a coherent underlying self-concept and personal values, which provide critical motivation for goal-related pursuits (Hayes and Hofmann, 2021).
Many contemporary therapies focus on only one of the domains above, implicitly assuming capacities in other domains that may constrain the efficacy of intervention approaches or sustained benefits. For example, Acceptance and Commitment therapy explicitly focuses on enhancing the salience of personal values, mindfulness, and behavioral response contingencies in the service of enhancing psychological flexibility but is relatively agnostic to the cognitive capacity of individuals. In contrast, intervention approaches among older adults with some level of cognitive impairment rely on a broader diversity of targeted domains, recognizing that cognitive control techniques, motivational factors, and affect regulation will all constrain an individual’s ability to volitionally modulate behavior in response to contextual demands. The widely used and efficacious Motivationally Enhanced Compensatory Cognitive Training for Mild Cognitive Impairment (ME-CCT-MCI) (Twamley et al., 2014, 2015; Sherman et al., 2017) provides a representative example. Self-regulatory function is a key psychological domain affected by multiple, disparate processes of change. As described in detail by Hayes and Hofmann (2021) self-regulation involves both overt behaviors and a cohesive, internalized sense of self. At the same time, important elements of self-regulatory skills, such as mindfulness, involve integration of affect, cognition, and attention, sometimes in the service of self-transcendence. Individuals who self-referentially perseverate due to a recent traumatic brain injury, for example, may subsequently exhibit increased depression that is being amplified by executive impairments that may improve. Self-regulation therefore combines all elements within contemporary, process-focused intervention initiatives (Hayes and Hofmann, 2021), including emotional, cognitive and attentional flexibility, perspective-taking and sense of self, personal values as a source of self-motivation, and construction of overt behavioral patterns based on these values. Critically, the flexible application of self-regulatory skills across multifaceted contexts in daily life place integral importance on individual differences in psychological flexibility (Kobylinska and Kusev, 2019), such that the ‘effectiveness of emotion regulation strategies depends on both situational contexts as well as individual differences in personality-like characteristics’ (Kobylinska and Kusev, 2019).
The ability to regulate one’s own behavior is one of the most critical psychological processes for leading happy, independent, meaningful lives. ‘Self-regulatory functioning’, or the ability to exert volitional control toward long term goal pursuits has been one of the most widely studied psychological functions, resulting in a wide and often contradictory literature base and multiple, closely related conceptual frameworks incorporating such concepts as executive functioning, self-management, grit, hardiness, and resilience. While there are important conceptual distinctions between each of these concepts, particularly in regard to their study within specific contexts, few overarching conceptual frameworks are available to help integrate these domains in order to inform personalized treatment approaches. An integrated framework is particularly important given the myriad factors plausibly affecting self-regulatory functioning across multiple levels of analysis, including variations in cognitive abilities across the lifespan, phenotypic differences in affective response patterns, and widely varying individual differences in contextual demands that will affect the importance and contingencies of individually initiated self-regulatory behaviors. The present, integrative review will attempt to provide a broad, parsimonious framework integrating elements across all three of these levels (neurobiological, affective, and contextual) toward a simplified framework to generate personalized intervention strategies.
The ability to effectively regulate one’s behavior relies on both functioning neurobiological systems within frontal-subcortical brain circuitry and the ability to effectively regulate ones affective responses to achieve valued behavioral goals. In addition, these functions have been shown to have differential vulnerability depending on contextual demands, with even small decrements manifesting themselves in the setting of high context demand characteristics. Similar to conceptual models for frailty, postoperative cognitive decline, or even more general biobehavioral models, the importance of efficient functioning within these behavioral domains is amplified in the setting of injury, elevated distress, or resource depletion (e.g., sleep deprivation, hunger, physical pain). While injury to systems integral for neurobehavioral facilitation of self-regulation are typified by changes in affect (e.g., traumatic brain injury
Comments (0)