A cross-sectional survey of 300 women from an Iranian infertility clinic by Laya Farzadi [19] revealed that the mean irrational parenthood cognition score was 39.7, which is similar to the results of this study, indicating that the surveyed patients with RIF had an internal desire to have a child to live a happy life. The outcomes of the cross-sectional study are comparable to those of the current study. In the findings of Zhao Jing [20] et al.’s study of factors related to morbidity stigma and infertility-related stress among 233 female infertility patients at the Wuhan Reproductive Centre, the mean infertility-related stress score was 137.69±29.42, which closely matched the mean total fertility stress score in the study by Newton et al. [21]; the fertility stress score of the patients with RIF in this study was considerably greater than those of the previous studies. The treatment of infertility is a process that involves both hope and disappointment; most patients are middle-aged and young adults who bear greater responsibilities and experience family- and career-related stress. This stress, coupled with repeated treatment cycles in the face of multiple implantation failures and high psychological fluctuations, significantly increases the level of fertility stress. Patients with an education level of high school or less and an irrational parenthood cognition score in the upper middle range had higher fertility stress scores and received relatively less social support. The higher a woman’s education level was, the lower the level of infertility stress. This may also be because the perceptions of fertility in patients with lower education levels are largely inherited from the traditional concept of women continuing the family line; therefore, these patients, who have a limited understanding of infertility and its treatment, are more likely to blame themselves for their inability to conceive. Additionally, they may be more affected by social opinions and prejudices, causing them to experience greater fertility stress. In contrast, patients with a higher degree of education can learn more pertinent knowledge and are better able to communicate with health care experts; consequently, they experience less fertility stress. The higher the annual household income level and the lower the levels of irrational cognitions and fertility stress are, the greater the level of social assistance received by patients. In women with regular jobs or high annual household income levels, work can be considered an accomplishment and balance the focus on fertility, and a higher household economic level ensures a higher quality of life, resulting in a relatively low perception that this group of infertility patients must have a child. This study also identified statistically significant differences between the irrational parenthood cognition scores of women with RIF and the relationship and social support scores of their partners. The degree of rationality of women's beliefs about fertility was associated with the quality of the couples’ relationships, with those who had better relationships with their partners having a greater degree of rationality about fertility and obtaining greater amounts of social support. This suggests that a healthy couple relationship and the support of one’s partner are particularly important in the treatment of female infertility, which does not improve somatic symptoms but significantly improves negative emotions in female patients, allowing them to face treatment with optimism and increase their resilience.
In this study, the greater the irrational parenthood cognition score was, the higher the fertility stress score; conversely, the higher the amount of social support, the more rational the perception of fertility. When enduring stressful events, irrational parenthood cognitions can lead to significant emotional and behavioral disturbances, whereas correct perceptions about infertility can lead to increased treatment cooperation and reasonable thinking about the stigma of the condition [22]. Although many cultures do not have specific solutions to childlessness, people do not accept childlessness passively [7]. Female patients with high levels of irrational parenthood cognitions believe that childlessness implies the loss of the parental role, making them deficient regarding typical family life and prone to increased marital conflict and crises [23]. Traditional perspectives on sexuality consider that limited or diminished reproductive potential indicates low sexual functioning, which impacts the gender role identities of couples experiencing infertility and causes a certain amount of sexual stress [24]. Some African cultures view infertility as an exclusive female problem [7]. A study of involuntary childlessness in seventy-eight societies found that women were significantly more likely to be blamed for childlessness than men, a fact attributed to the ubiquity of women’s low social statuses across cultures [25]. Infertility occurs in close to equal amounts for men and women, yet the general awareness of male factors contributing to involuntary childlessness is limited in society [26]. Almeling examined the reporting and dissemination of pregnancy and reproductive health information in the US cultural environment and found a lack of information on male reproductive health in the public domain [27]. This invariably increases the social and reproductive pressure on women with infertility, making them reluctant to interact with others and vulnerable to discrimination and prejudice, which can lead to inferiority complexes. Simultaneously, psychological problems caused by irrational fertility perceptions can have a negative impact on the medical behavior of women with infertility, thereby delaying the treatment process and resulting in a reluctance to communicate with others about fertility, decreasing the social support these patients receive. Therefore, during clinical therapy for infertility, we should have a comprehensive understanding of the lives and cultural backgrounds of such patients, urge them to actively seek and accept social support from all available sources, and provide them with professional health education on infertility. Assisting patients in replacing irrational ways of thinking and beliefs with rational ones can also be achieved through psychological interventions such as positive thinking therapy, group cognitive therapy, and rational emotive behavior therapy.
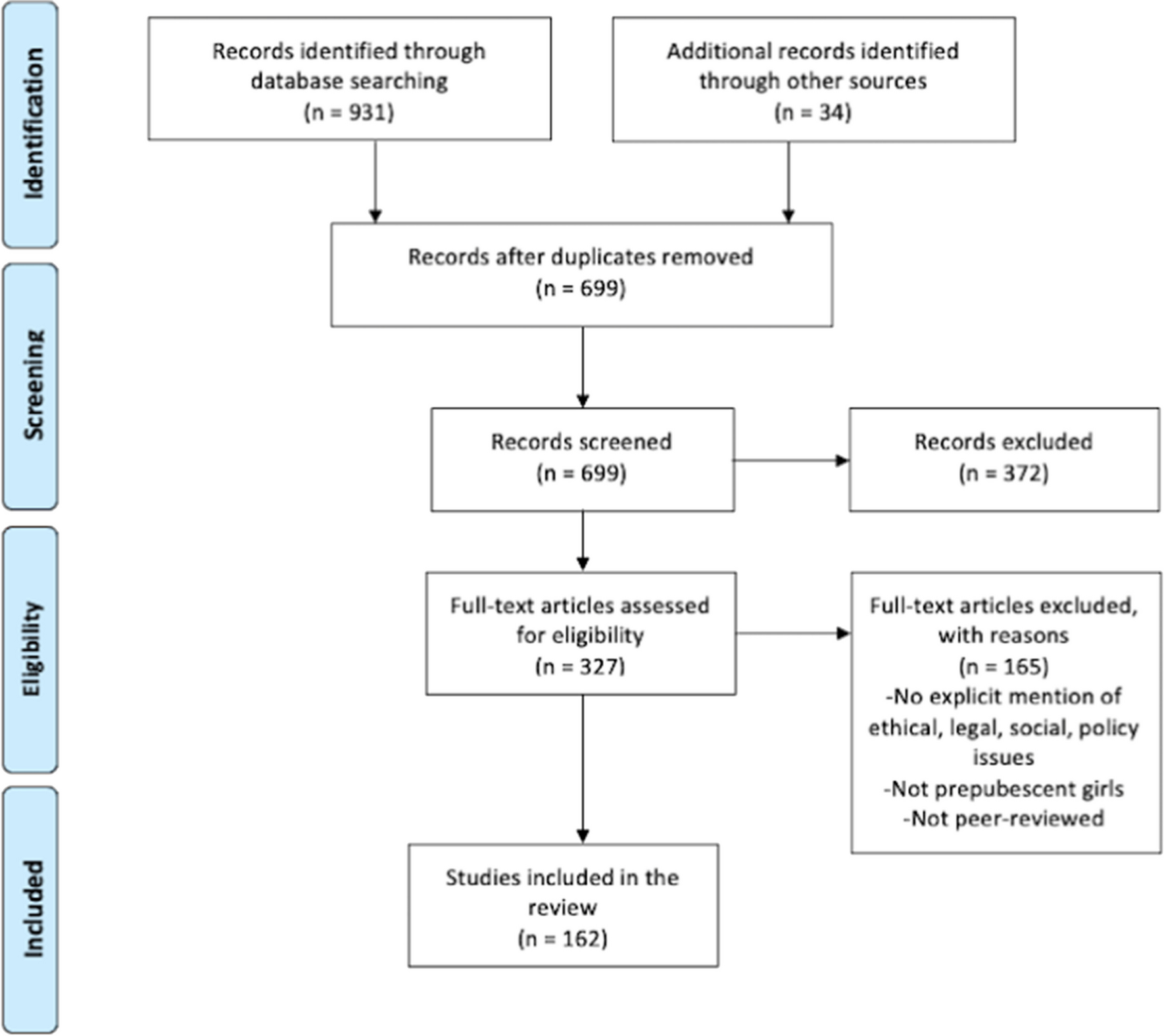
Figure 1 depicts the findings of the analysis of the mediating influence of reproductive stress on the relationship between irrational parenthood cognitions and social support in patients with RIF. However, social support did not have a direct effect on irrational parenthood cognitions. Specifically, the amount of social support received by women with RIF could not directly predict illogical parenthood cognitions, while the level of fertility stress could indirectly predict irrational parenthood cognitions. This may be because patients with RIF have experienced multiple IVF-ET failures and have expended a greater amount of human, material, and financial resources than other patients, creating strong psychological feelings of guilt, which manifest as social stress, couple relationship stress, sexual stress, and childlessness trade-off stress, hence predicting the level of illogical parenthood cognitions among female patients with RIF. The vast majority of patients undergoing assisted reproductive treatment aim to achieve a successful pregnancy and improve their quality of life and well-being. However, repeated failed transfers not only fail to meet the therapeutic requirement for a successful pregnancy but also increase the financial and psychological burdens on patients and their families, with familial and social pressures dominating the situation. Patients experience negative emotions such as low self-esteem, anxiety, and guilt due to infertility. This, combined with traditional thinking and previous transfer failures, depletes not only their savings but also increases the pressure these patients feel from their spouses and other sources, causing them to become even more nervous, anxious, fearful, and desperate about having children.










Comments (0)