
Remember me


A total of 315 patients from our Post-COVIDLMU outpatient department with a likely or confirmed PC syndrome were enrolled in our study. OH, MH, PH and pain were rated by the patients themselves, their treating INT, and PSY independently. This assessment of disease perception was completed in 71 of the 315 cases. Of these 71 patients, the majority was female (56% female vs 44% male; Table 1). The Mdn age at inclusion was 39 [30, 51] years. Most patients reported to be on sick leave (57%) due to the PC condition. The inability to work was also reflected by a Mdn Karnofsky index of 70% [70, 80]. In 88.7% of the cases the initial SARS-CoV-2 infection was non-severe and only 4.2% of patients were hospitalized. At the time point of inclusion, 17 (24%) of the patients had a history of psychiatric conditions with depression (13%) and chronic fatigue syndrome (8.5%) being the most common (Table 1). In 15 (21%) patients, psychiatric conditions were known prior to SARS-CoV-2 infection. 5 (7%) patients were diagnosed with a psychiatric condition after SARS-CoV-2 infection. A Mdn of 4 [3, 6] preexisting somatic conditions was found with 54 (76%) of the patients having a history of at least one somatic disease. Bronchial asthma (14%) and primary hypertension (13%) were the most prevalent somatic diagnoses (Table 1). 45 (63%) patients had known somatic conditions prior to SARS-CoV-2 infection, 21 (30%) acquired new somatic diagnoses after infection.
Table 1 Patient characteristics and PROMsResults of the physical health domain of the WHOQoL-BREF showed a considerably low Mdn value of 44 [31, 54] points (Table 1) well below the reference margin (for reference values, see “Patients and Methods”). Likewise, the psychological health section revealed an impaired Mdn value of 58 [46, 67] points, while the social relationship (Mdn points 75 [58, 75]) and the environment section (Mdn points 72 [66, 78]) did not appear to be negatively affected. The Mdn PHQ-9 score was 10.0 [6.0, 14.0], reflecting moderate depression severity (based on Kroenke et al. [10]). A Mdn FSS of 57 [48, 60] indicated a high degree of clinically relevant fatigue.
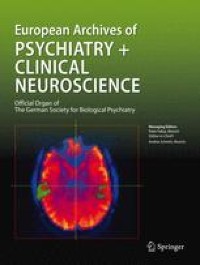
Differences in disease and pain quantification between PAT, INT and PSYComparing health ratings by patients themselves, their attending INT and PSY, we found statistically significant differences with respect to OH (p < 0.001; Table 2), PH (p < 0.001) and pain assessments (p < 0.001) between the three groups. For example, 33% of patients rated their physical health as very poor (1), while PSY found this to apply in only 1.6% and INT in 0% of the cases (Fig. 1). In contrast, the ratings of the patients’ MH did not differ to a statistically significant extent (p = 0.063; Table 2).
Table 2 Comparison of disease perceptions by PAT, INT and PSYFig. 1
Detailed results of health assessments by PAT, INT and PSY. Patients, INT and PSY assessed PC patients’ (n = 71) health on Likert scales (A) or pain using the NPRS (B) as described in Patients and Methods. A The results are shown as ratios of all answers. B Bold vertical lines indicate median values; the colored horizontal bars resemble IQRs
Figure 1 gives detailed insight into the health assessments by the three groups. Respective subgroup analyses of Table 2 are depicted in Table 3A–C. The latter demonstrate that the evaluations of patients’ OH (p < 0.001) and PH (p < 0.001) differed significantly between PSY and PAT, while the ratings of patients’ MH and degree of pain [p values for both = not significant (n.s.)] appeared to be more in line between those two groups (Table 3A). In contrast, comparison of the INT and PAT health evaluations showed statistically significant differences in all fields but MH (p < 0.001 for OH, PH and pain; p = n.s. for MH; Table 3B). Lastly, when comparing INT and PSY health assessments of the patients, MH evaluations seemed to tightly align (p = n.s.), while OH (p < 0.001), PH (p < 0.001) and pain (p < 0.001) assessments did also differ significantly (Table 3C).
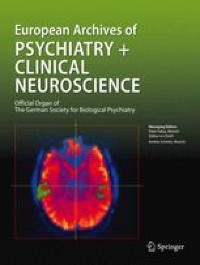
Table 3 Subgroup analysis of disease perceptionsCorrelation analysis of disease perceptions between PAT, INT and PSYWe observed marked differences in medians of health estimates between the three groups. To investigate if the health ratings correlated despite differences in medians, we created a correlations matrix for all health ratings (Fig. 2A).
Fig. 2
Correlation analyses of disease perceptions by PAT, INT, PSY between the groups, with other PROMs and objectifiable findings. Correlation matrices of disease perceptions by INT, PSY and PAT (n = 71). Correlations between the three groups and between disease perceptions and other PROMs, results of diagnostic procedures (number of all procedures or number of pathological outcomes) and other objectifiable findings were tested using the Spearman correlation. WHO environment, social relationship, psychological health and physical health refer to the respective sections of the WHOQoL-BREF. The figure shows Spearman’s R. Non-significant correlations (p value ≥ 0.050) are crossed out
Despite statistically significant differences in the quantitative grading of patients’ OH and PH, but not MH and pain, between PSY and PAT (Table 3A), the correlation analysis revealed a positive correlation for both MH and pain (Spearman’s R for MH: 0.42, p < 0.001; Spearman’s R for pain: 0.49, p < 0.001; Fig. 2A), but no significant correlation for OH and PH (Spearman’s R for OH: 0.22, p = n.s.; for PH: 0.24, p = n.s.). This suggests that pain ratings of PAT and PSY closely align. MH ratings correlated significantly, and PAT quantified their MH only slightly lower with no statistical significance than PSY do. In contrast, assessments of OH and PH did not show any relation at all between the groups.
We next focused on possible correlations between disease perceptions by INT and PAT. The dissonant gradings of patients’ OH, PH and pain (Table 3B) fully translated onto the correlation matrix, revealing no statistically significant correlation at all for any of the four health domains assessed (Spearman’s R for OH: 0.13, p = n.s.; for MH: 0.27, p = n.s.; for PH: 0.18, p = n.s.; for pain: 0.27, p = n.s.; Fig. 2A). These findings indicate that the assessments of a PC patients’ condition may completely diverge between PAT and INT.
Contrary to the discrepancies between PAT and PSY/INT, assessments of INT and PSY were more aligned: The correlation analysis showed a positive correlation with respect to the rating of all four health domains (Spearman’s R for OH: 0.41, p = 0.002; for MH: 0.46, p < 0.001; for PH: 0.34, p = 0.012; for pain: 0.39, p = 0.004; Fig. 2A). Taken together with the data from Table 3C, this indicates that INT graded patients’ OH and PH as less impaired and pain as less severe than PSY, while a positive correlation between the two observer groups was still present. MH ratings of INT and PSY aligned closely.
Of note, within the patients’ own assessments, the PAT grading of MH correlated positively with OH (Spearman’s R = 0.62, p < 0.001) and PH (Spearman’s R = 0.54, p < 0.001). However, no significant correlation between MH and pain (Spearman’s R = 0.11, p = 0.422) was found. In line with our expectations, OH and PH showed a positive (Spearman’s R = 0.82, p < 0.001), OH and pain as well as PH and pain a negative correlation (Spearman’s R for both = − 0.34, p = 0.011 and p = 0.012, respectively). This translates into OH, MH and PH all depending on each other, while OH and PH were perceived as better at low levels or in the absence of pain. Interestingly, pain and MH did not seem to depend on each other in our cohort of patients.
Disease perceptions by PAT, INT and PSY and possible correlations with other PROMs and objective findingsNext, we assessed possible correlations of disease perceptions with other PROMs and objectifiable findings (Fig. 2B). The strongest and/or most numerous correlations of health ratings were found with the psychological and physical health section of the WHOQoL-BREF, PHQ-9, FSS and Karnofsky index.
The psychological health section of the WHOQoL-BREF correlated well with the patients’ own perception of OH, MH and PH, but not pain (Spearman’s R for OH: 0.60, p < 0.001; for MH: 0.75, p < 0.001; for PH: 0.41, p = 0.002; for pain: 0.25, p = 0.066; Fig. 2B). It showed a decently positive correlation with PSY assessments of MH (Spearman’s R: 0.48, p < 0.001), but no statistically significant correlations with any other assessments by PSY or INT.
Similarly, the physical health section of the WHOQoL-BREF correlated positively with the patients’ own perception of OH, MH and PH and negatively with pain (Spearman’s R for OH: 0.60; for MH: 0.46; for PH: 0.54; for pain: − 0.66; all p values < 0.001; Fig. 2B). It showed statistically significant positive correlations with INT assessments of OH and MH (Spearman’s R for OH: 0.30, p = 0.034; for MH: 0.29, p = 0.046) and a negative correlation with PSY assessments of pain (Spearman’s R: − 0.35, p = 0.014), but no statistically significant correlations with any other assessments by PSY or INT.
The PHQ-9 score correlated negatively with the patients’ perception of their OH, MH and PH, and positively with pain (Spearman’s R for OH: − 0.50, p < 0.001; for MH: − 0.58, p < 0.001; for PH: − 0.45, p < 0.001, for pain: 0.30, p = 0.029; Fig. 2B). It also correlated negatively with PSY assessments of MH (Spearman’s R: − 0.33, p = 0.023), but no significant correlations were found regarding the remaining assessments by PSY or INT.
Just as the PHQ-9 score, albeit slightly less pronounced, the FSS correlated negatively with the patients’ perception of OH, MH and PH, and positively with pain (Spearman’s R for OH: − 0.41, p = 0.002; for MH: − 0.45, p < 0.001; for PH: − 0.30, p = 0.026, for pain: 0.40, p = 0.002; Fig. 2B). No statistically significant correlations were found with any of the assessments by PSY or INT.
Lastly, the Karnofsky index correlated well with patients’ perceptions of OH, MH and PH, but not pain (Spearman’s R for OH: 0.40, p = 0.004; for MH: 0.39, p = 0.005; for PH: 0.36, p = 0.010, for pain: 0.23, p = 0.121; Fig. 2B). Further, positive correlations were found between the Karnofsky index and INT assessments of OH and MH (Spearman’s R for OH: 0.48; for MH: 0.54; both p values < 0.001) and PSY assessments of MH (Spearman’s R: 0.28, p = 0.038). Of note, the Karnofsky index did not correlate with pain ratings of any of the groups.
Interestingly, none of the health assessments by any of the groups correlated with the overall amount of diagnostic procedures performed, not even with the number of pathological findings in diagnostic procedures (Fig. 2B). Few and/or rather weak correlations with statistical significance were found for the environment and social relationship section of the WHOQoL-BREF, working status, number of medical contacts, somatic or psychiatric diagnoses.
Comments (0)