
Remember me
Armand Trousseau introduced “status epilepticus” (SE) in 1867 [1]. SE was largely ignored until Whitty and Taylor emphasized its severity and need for immediate treatment in 1949 [2]. Because “in the fatal cases the interval between the onset of SE and the beginning of treatment was usually much longer than in the non-fatal cases,” they recommended urgent, adequate, repetitive doses of intramuscular paraldehyde “in doses which abolish consciousness.” Initial treatment was followed by intravenous drip if seizures recurred to “adjust blood-paraldehyde level, so fits are controlled but coma is not too deep,” acknowledging balance between rapid seizure control and side effects with higher doses [2].
Current first-line and second-line antiepileptic drugs fail to control seizures in ~ 33% of SE cases (refractory SE [RSE]) and require prompt treatment escalation and supplementary second-line agents and anesthetic drugs. Treatment intensity requires a risk–benefit equation considering patient’s age, type of seizure, electroencephalographic (EEG) findings, consciousness level, seizure history, comorbid states, and potential medication side effects [3]. Anesthetic drugs require continuous EEG monitoring. Yet, the end point (i.e., seizure suppression, burst-suppression pattern (BSP), or flat recording, and its duration) remains unclear and lacks supportive data [3]. How did BSP remain relevant with neurology practitioners? This historical article tracks the roots of this EEG paradigm and discusses the evidence that allegedly support its recommendation.
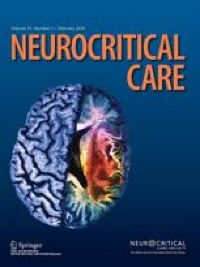
Earlier Descriptions of EEG BSPAfter EEG was introduced in hospitals, literature recognized BSP as a distinctive EEG pattern characterized by intermittent high-power oscillations alternating with isoelectric coma periods, induced by general anesthesia and hypothermia [4, 5]. Swank and Watson popularized the term in 1949 [6], but Derbyshire et al. [7] introduced it in 1936 (Fig. 1) when studying tribromoethanol, a positive allosteric modulator of type A gamma amino butyric acid and glycine receptors, on the feline cerebral cortex. The dismal prognosis of BSP/EEG in comatose patients, particularly after brain anoxia, was recognized in the 1960s [8]. Although the physiologic underpinnings of BSP are debatable, neuronal hyperpolarization (caused by depressed excitatory glutamatergic currents as high-dose anesthetic drugs targeting the type A gamma amino butyric acid transmission, enhancing inhibitory signals, and reducing excitatory neurotransmission) may induce BSP. Interplay between hyperpolarization-induced inhibition and intermittent neural-circuit reactivation produces cyclic BSP in the EEG [4]. Low-dose anesthetic drugs produce short, infrequent periods of background attenuation or suppression. Higher doses increase and prolong these periods, leading to complete background suppression [5]. This pattern reduces cerebral-metabolic rate and blood flow; it has been studied for neuroprotection for brain injuries and cardiac anesthesia [4]. In patients undergoing nonpulsatile cardiopulmonary bypass, pharmacologic BSP with propofol significantly reduced cerebral blood flow (measured with Xe clearance), oxygen delivery, and metabolic rate. No differences were found in cerebral arterial venous oxygen difference and jugular-bulb venous oxygen saturation, indicating maintained cerebral-metabolic autoregulation [9], which was confirmed in a study obtaining simultaneous intracranial pressure (ICP) and EEG data from two patients with burst suppression. Mean ICP increase after EEG bursts (0.54 mm Hg) significantly correlated with burst duration and vasodilatory index derived from ICP-pulse waveform, suggesting intact neurovascular coupling [10]. This is relevant in SE because continuous seizures increase cerebral metabolism and expose the brain to ischemic damage. Current terminology of the American Clinical Neurophysiology Society Guidelines for Critical Care EEG arbitrarily define BSP as suppression or attenuation periods in > 50% of the EEG recording [11].
Fig. 1
First EEG recording of burst suppression. The figure depicts EEG spike responses in different cerebral areas under deep Avertin (tribromoethanol). EEG, electroencephalogram
Burst Suppression as Therapeutic Goal in SEFor many years, physicians titrated available sedatives clinically, striving to suppress clinical seizure activity and avoid hemodynamic instability, particularly arterial hypotension. In 1967, Brown and Horton published their treatment of 117 patients with SE over a 16-year period using intravenous thiopentone [12]. They recommended a slow loading dose (25–100 mg) “until convulsions cease,” followed by infusion up to 72 h afterward. They felt that 48 h typically sufficed. In 1980, Young et al. [13] reported five anesthetic barbiturate-treated RSE cases and assessed anesthesia depth electroencephalographically, clinically, and by serum-barbiturate levels. The authors reported that 2-s to 7-s interburst interval patterns stopped clinical and electrographic seizures. They monitored EEG hourly in two patients using a single channel and by standard recordings in the remainder. Serum-pentobarbital levels of 2–4 mg/dl corresponded to EEG/BSP pattern. Of note, patients received fixed doses of barbiturates, not titrated according to EEG data but high enough to achieve BSP in all patients [13]. A similar pediatric report was published 2 years later [14]. The first report of continuous EEG to titrate barbiturates in RSE cases was published in 1981 [15]. These five patients had seizure refractory to diazepam and phenytoin, fulfilling the current definition of RSE. They received thiopentone load until seizures stopped, followed by a 12-h infusion after “cessation of abnormal electrical activity” and slow weaning for additional 12 h. The goal was to “keep patients free of epileptic discharges,” with no mention of BSP pattern or flat record [15].
Orlowski et al. [16] published the first detailed barbiturate anesthesia protocol in 1984, the first known report in which EEG/BSP was a therapeutic target in SE. Selecting three pediatric patients with RSE, they administered a predefined protocol including barbiturates and hypothermia. After an initial thiopental loading dosage (30 mg/kg/h), all patients received continuous infusion of 5–55 mg/kg/h, cooled to ~ 31 °C. Continuous EEG monitoring documented a BSP pattern. Dopamine counteracted barbiturate-induced hypotension. A Swan-Ganz catheter monitored cardiovascular and core-temperature status, maintaining a 2-day to 5-day barbiturate coma. All patients survived, and two returned to baseline following treatment. The rationale for achieving BSP or isoelectric EEG was its correlation with thiopental-plasma levels of 25–40 mg/dl, with “the advantage of being immediately recognizable rather than waiting hours for blood levels to be determined.” They also claimed that BSP or isoelectric EEG pattern “was assumed to correlate with maximum suppression of epileptic discharges from the brain” [16]. Previously, Bruce et al. [17] reported that serum pentobarbitone, 25–50 mg/l, was necessary to achieve EEG/BSP with equal durations of burst and suppression in patients with intracranial hypertension. In 1987, Rashkin et al. [18] reported their experience treating nine patients with RSE, defined as failure to two first-line anticonvulsants, with phenobarbital [1]. Patients received a 5 mg/kg intravenous bolus of pentobarbital and additional 25-mg to 50-mg bolus infusions at 2-min to 5-min intervals until BSP occurred every 15 s on EEG [18]. Infusion continued for 12–24 h at 5 mg/kg/h and then decreased by 1 mg/kg/h every 6 h. If seizures recurred, infusion rates returned to previous levels. Curiously, the justification for the desired depth of EEG suppression was based on a sole case reporting evolution of EEG patterns after barbiturate intoxication [19]. This approach terminated seizures in 8/9 patients within an hour of therapy. Because of underlying metabolic or structural brain lesions, ~ 80% of patients died. Hypotension, common during the loading phase, frequently required intravenous saline and dopamine. The authors concluded that pentobarbital infusion effectively suppressed seizures in RSE but with high mortality and increased morbidity.
This article established EEG/BSP as a therapeutic goal in many studies [20,21,22]. Some experts recommended even more aggressive approaches in seizures refractory to diazepam, phenytoin, and phenobarbital (e.g., Ramsay recommended sufficient drug “to produce a flat EEG”) [23]. Treatment duration varied according to clinical response: “The infusion is stopped after 4–6 h and the patient and EEG re-evaluated as the drug effect wears off,” but rationale-supporting data were not provided [23]. Of note, higher doses of anesthetic drugs, associated, however, with several systemic, dose-dependent side effects, are needed to achieve EEG suppression [24].
The Debate ContinuesOnce EEG/BSP pattern emerged in the literature as a therapeutic goal in RSE, researchers explored whether the depth of EEG suppression improved seizure control and clinical outcomes. Krishnamurthy and Drislane reported 35 patients with RSE treated with pentobarbital coma (1984–1996) [25]. Persistent seizure control was achieved in 6/12 patients achieving a BSP pattern, 17/20 with a “flat” EEG, and 3/3 with slow, nonsuppressed EEG patterns. Isolated epileptiform discharges during the infusion were unassociated with outcome, questioning the need for complete suppression. The authors concluded that deeper suppression correlated with better survival [25]. Furthermore, the depth of EEG suppression was chosen by the treating clinicians rather than according to a protocol, with the usual target being EEG/BSP. This introduces an important selection bias next to the retrospective nature of study: targeting EEG/BSP may mask cases potentially requiring less aggressive treatment. In addition, patients who achieved BSP may have been easier to suppress because of a less severe SE leading to confounding and reverse causation. Subsequently, in a systematic review of 193 patients with RSE treated with propofol (n = 54), midazolam (n = 33), and pentobarbital (n = 106), the exposures were the choices of anesthetic agent and the titration goal (seizure suppression vs. EEG-background suppression). Main outcome measures included frequency of immediate treatment failure and mortality. Mortality (48%) was not significantly associated with agent choice or titration goal. Pentobarbital was more frequently titrated to electrographic-background suppression, whereas seizure suppression was the most frequent treatment goal of midazolam and propofol. Pentobarbital treatment correlated with less short-term seizure recurrence and more frequent hypotension. Titration of anesthetic drugs to EEG-background suppression (n = 87) had fewer breakthrough seizures without differences in short-term treatment failure, withdrawal seizures, or intravenous medication change. The authors reported higher frequency of hypotension in patients treated with EEG-background suppression. Long-term functional outcomes and other important outcomes were not explored [26]. Around that time (early 2000s), two surveys revealed that BSP was the favored treatment target, phenobarbital the preferred anesthetic drug, and 48-h treatment duration the preferred choice [27, 28]. Later, another study of 127 patients with SE from two centers (RSE = 47) achieved burst suppression in 20/33 monitored episodes (61%), with outcome independent of specific coma-inducing agents or EEG/BSP level. The authors concluded that the underlying cause of SE determines prognosis [29].
Most recent studies have also failed to prove a benefit from BSP over more conservative approaches. In one retrospective study of 63 patients with RSE, seizure control without BSP correlated with a good functional outcome at hospital discharge [30]. In another retrospective study (n = 22), BSP was achieved in 27% of patients and associated with prolonged hospital stay, without mortality or outcome benefit [31]. Phabphal et al. [32] analyzed 51 cases of nonanoxic RSE and found EEG/BSP correlated with fewer breakthrough seizures and no increased risk of medical complications, mortality, or functional outcomes. Yet, these findings should be interpreted considering the retrospective analysis, small sample size, narrow inclusion criteria, insufficient SE-subtype data in each group, and imbalances between treatment groups. Muhlhofer et al. [33] studied 182 patients with RSE treated with anesthetic agents (mostly propofol), considering the hourly changes in infusion rates as a surrogate for coma depth and duration. They found that longer duration of the first therapeutic coma independently correlated with higher seizure recurrence, and higher doses of anesthetic used during the first trial independently correlated with fewer in-hospital complications and shorter-duration mechanical ventilation and total length of stay [33]. This supports deep, short-duration therapeutic comas as safer and more effective than the recommended 24–48-h treatment period. However, lack of EEG data as a sedation-depth measure is an important limitation disallowing definitive conclusions. In another study, among 61 patients with RSE, 62% had induced coma for > 48 h and 39% reached BSP. BSP was associated with poor prognosis at 1 and 2 years, and its absence was associated with better survival [34]. Lastly, in a retrospective study of 147 patients with RSE (n = 42 from cerebral anoxia) treated with intravenous anesthetics drugs, 20% achieved EEG/BSP with suppressed background > 50% of the time irrespective of persistent seizure termination, in-hospital survival, or return to premorbid neurologic function [35].
Safety ConcernsIn critically ill patients, BSP is associated with mortality, incidence, and duration of delirium [36, 37]. In a mediation analysis, Hogan et al. [38] found that BSP was primarily attributable to critical illness, being a mechanism of death, which accounted for 10% in the increase in mortality in their population. Among elderly patients who underwent general anesthesia, BSP was associated with an elevated frailty score and increased the likelihood of postoperative delirium [39].
In patients with RSE, BSP is associated with prolonged mechanical ventilation, hypotension, prolonged intensive care unit stay, and hospital stays [35]. In a retrospective case–control series of 33 patients with RSE treated with midazolam (n = 19, 5% achieved BSP) or thiopental (n = 14, 79% achieved BSP), the thiopental group had higher frequency of severe hypotension, infections, anemia, leucopenia, hyponatremia, longer intensive care unit length of stay, and worse 6-month outcomes [40]. Although EEG suppression could be a driver of outcomes, specific medications could also play a role. For example, in a small clinical trial, patients with RSE were randomly assigned to receive propofol (n = 14) or barbiturates (n = 9) titrated to BSP for 36–48 h. Barbiturates were associated with longer mechanical ventilation time [41].
EEG/BSP is difficult to achieve and sustain as evidence by a study in which BSP was achieved only 8% of the total treatment time, suggesting significant pharmacokinetic and pharmacodynamic variation [42]. It often requires incremental doses of anesthetics that cause hypotension with requirement of fluid resuscitation and vasopressors [43].
Comments (0)