
Remember me
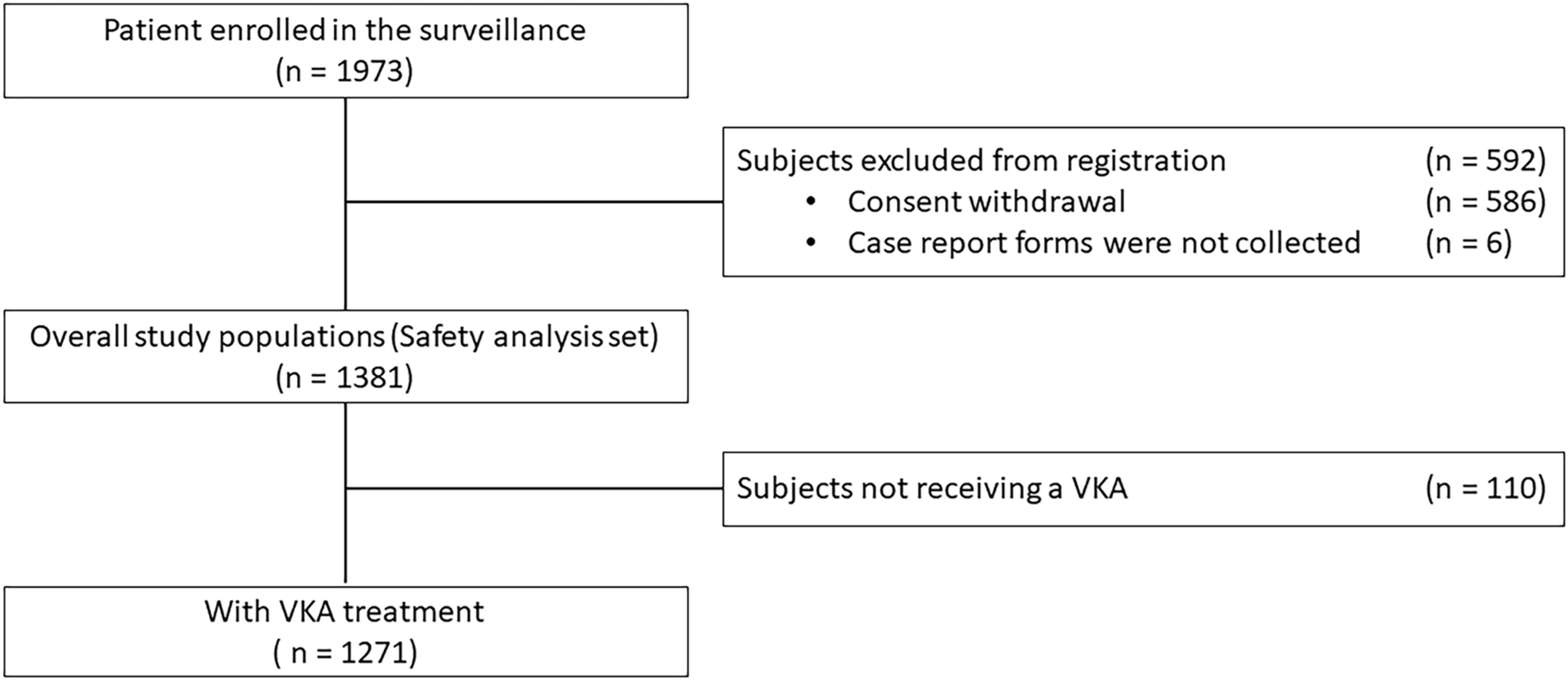
Between September 2016 and November 2020, a total of 1393 patients were enrolled across 697 medical institutions (Fig. 1). CRFs were collected for 805 patients across 494 medical institutions by April 2019, of which 804 forms were validated. The safety analysis set included 804 patients: 542 in group A and 240 in group B; 16 patients were included in both group A and group B (shown as group A + B), and six patients were classified as “Other” as determined by the investigators. The effectiveness set included 793 patients: 541 in group A, 236 in group B, and 16 in both group A and group B; 11 patients were excluded from the effectiveness set due to off-label use, no treatment with dabigatran, or no all-effectiveness data (Fig. 1).
Fig. 1
Patient disposition. CRF case report form, PMDA Pharmaceuticals and Medical Devices Agency. *CRF required for cases in which idarucizumab was used from the time of approval of idarucizumab (September 2016) through April 14, 2019. After consultation with the PMDA, a CRF was no longer required after April 15, 2019. †One CRF could not be validated
Baseline characteristics of the patients are shown in Table 1. The median age of the patients was 78 years and 67% were male. Most patients had reduced renal function (among evaluable patients, 62% had a creatinine clearance of < 80 ml/min, with 12% having a creatinine clearance of < 30 ml/min). Median time from last dose of dabigatran to the first infusion of idarucizumab was 9.2 h in group A and 9.7 h in group B. A baseline coagulation test was performed in 78% of patients.
Table 1 Patient characteristics at baselineIdarucizumab IndicationsAmong the 558 patients in group A and group A + B (group A/A + B), idarucizumab was indicated for the reversal of dabigatran due to intracranial hemorrhage in 208 patients (37.3%), gastrointestinal (GI) bleeding in 133 patients (23.8%), and intrapericardial bleeding in 106 patients (19.0%) (Fig. 2). Other bleeding sites were mainly in the chest, such as pulmonary hemorrhage in 21 patients (3.8%), and intrathoracic bleeding in ten patients (1.8%). In group A/A + B, 134 patients (24.0%) had trauma-related bleeding, including 86 of 208 patients (41.3%) with intracranial hemorrhage. In an assessment of bleeding severity, 108 patients (19.4%) in group A/A + B had ongoing blood loss and were hemodynamically stable, whereas 171 patients (30.6%) had ongoing blood loss and were hemodynamically unstable. Changes in the reasons for using idarucizumab on or before April 15, 2017, through April 15, 2019, are shown in Supplementary Table S1.
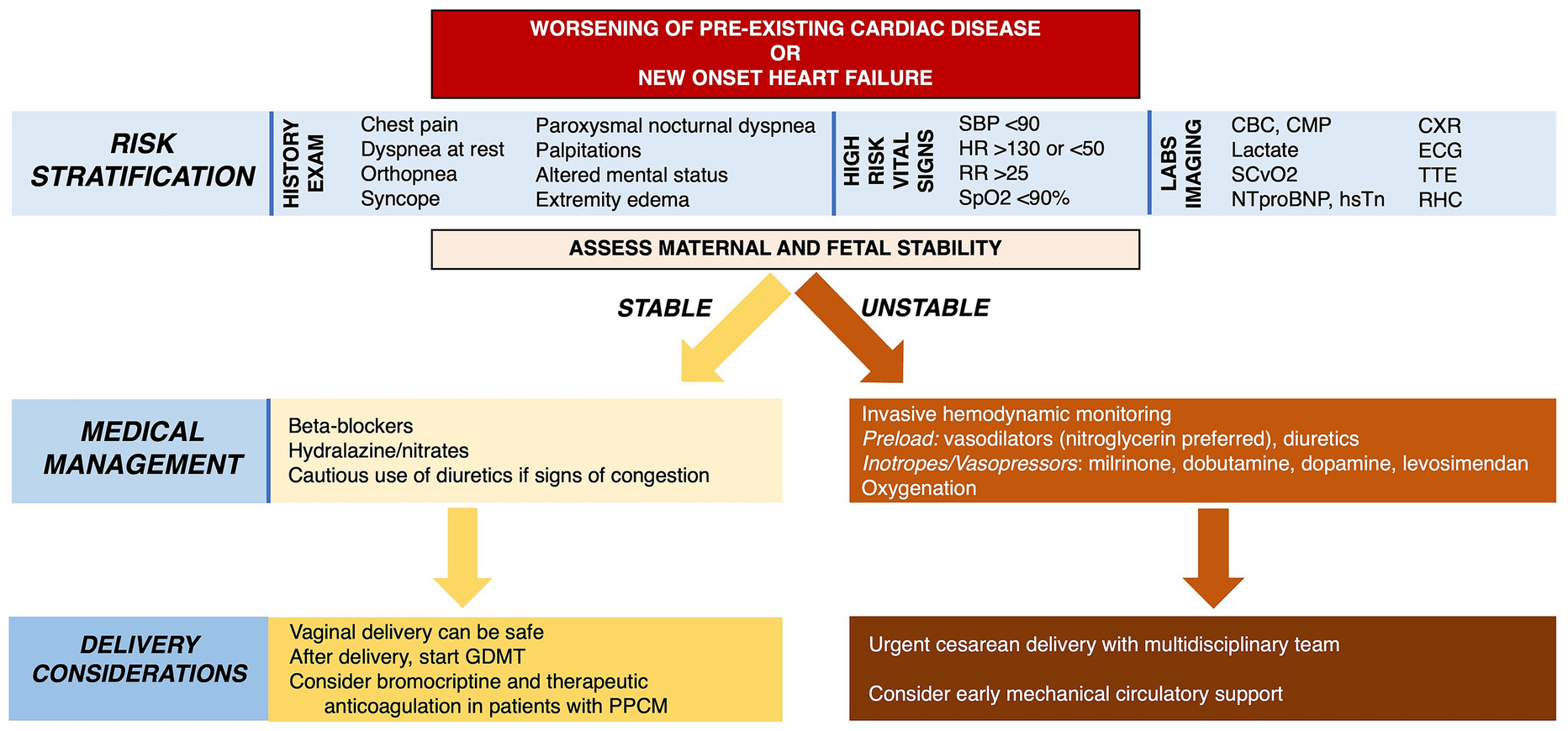
Fig. 2
Idarucizumab indication for reversal effect of dabigatran. a Location of bleeding events in group A/A + B (N = 558) and b types of surgery/procedures in group B/A + B (N = 211). Patients may have experienced more than one type of bleeding and thus the percentages in a exceed 100%. Among 208 patients (37.3%) with intracranial bleeding, the locations of intracranial bleeding (N, %) were intracerebral (139, 24.9%), subdural (78, 14.0%), and subarachnoid (55, 9.9%). Among 133 patients (23.8%) with gastrointestinal (GI) bleeding, 61 (10.9%) had lower GI bleeding only, 53 (9.5%) had upper GI bleeding only, 5 (0.9%) had both lower and upper GI bleeding, and 14 (2.5%) had an unknown GI bleeding location. In b, the types of surgery or procedures and number of patients for each were: Neurological—intracranial hemorrhage (78), cerebral infarct (23), hydrocephalus (3), abscess (2), for diagnosis (2), other (4); Vascular—aortic dissection/ruptured aortic aneurysm (24), cardiac tamponade/pericardial effusion (4), intracardiac thrombus (3), coronary artery disease (2), valvular disease (2), other (5); Abdominal–cholecystitis/cholangitis (12), gastrointestinal perforation (9), bowel obstruction (8), incarcerated hernia (4), other (5); Orthopedic—fracture (5), other (3); Respiratory—pneumothorax (2), other (5); Gynecological-urological—dialysis (2), other (4)
In group B/A + B, the most frequent emergency surgery/intervention required by the patients was neurological (53.1%), followed by vascular (19.0%), abdominal (18.0%), orthopedic (3.8%), respiratory (3.3%), and gynecological-urological (2.8%) (Fig. 2). Among the 16 patients in group A + B, 11 had intracranial hemorrhage and required surgical intervention.
SafetyAdverse Drug ReactionsADRs during the entire study period were reported in 17 patients (3.1%) in group A and 12 patients (5.0%) in group B, of which 14 (2.6%) and nine (3.8%) were considered serious (Table 2). ADRs during the idarucizumab treatment period (i.e., within 5 days of idarucizumab treatment) were reported in 13 patients (2.4%) in group A and ten patients (4.2%) in group B, which were serious in 11 (2.0%) and eight (3.3%) patients, respectively (Table 2). No ADRs were reported for patients included in group A + B.
Table 2 Summary of safety outcomesThe ADRs reported in group A and group B are listed in Supplementary Table S2. The most commonly reported ADRs were in the system organ class of nervous system disorders – six patients (1.1%) in group A and five patients (2.1%) in group B. Four of the five patients in group B experienced a cerebral infarction, compared with one patient in group A. The second most commonly reported ADRs by system organ class were vascular disorders—four (0.7%) in group A and one (0.4%) in group B. GI disorders occurred in two patients in each group. All of the ADRs reported as nervous system disorders (11) or as vascular disorders (five) were considered serious. Two patients in group B experienced a subdural hematoma. All other serious ADRs occurred in one patient in each group, including a patient in group A who experienced a serious GI disorder—rectal ulcer hemorrhage. ADRs by bleeding location and type of surgery/procedure are listed in Supplementary Tables S3 and S4, respectively.
AEs led to death in 73 patients (13.5%) in group A and 24 patients (10.0%) in group B, of which 58 (10.7%) and 16 (6.7%) occurred within 5 days of idarucizumab treatment (Table 2). A list of the AEs that led to death within 5 days of idarucizumab treatment for each patient is provided in Supplementary Table S5. The most common AEs that led to death were subdural hematoma (ten patients in group A and zero patients in group B), pneumonia aspiration (six patients and two patients), cerebral hemorrhage (six patients and one patient), hemorrhagic shock (five patients and zero patients), multiorgan dysfunction syndrome (three patients and one patient), brain herniation (one patient and three patients), pulmonary alveolar hemorrhage (three patients and zero patients), brain edema (two patients and one patient), cerebral infarction (two patients and one patient), cardiac failure (two patients and one patient), hemorrhage (one patient and two patients), peritonitis (one patient and two patients), pneumonia (one patient and two patients), and malignant neoplasm progression (one patient and two patients).
Thrombotic Events and HypersensitivityThrombotic events (ischemic stroke, myocardial infarction, pulmonary embolism, deep vein thrombosis, systemic embolism) were reported in 22 patients (4.1%) in group A and 15 patients (6.3%) in group B, of which nine (1.7%) and 11 (4.6%) patients, respectively, experienced thrombotic events within 5 days of idarucizumab treatment (Table 2). Of these thrombotic events, five (0.9%) in group A and five (2.1%) in group B were reported as ADRs. The details of thrombotic events are provided in Supplementary Table S6. Hypersensitivity (including shock and anaphylaxis) occurred in four patients (0.7%) in group A and five patients (2.1%) in group B—circulatory collapse (one and two patients, respectively), rash (two patients in group B), shock (two patients in group A), urticaria (one patient in each group), and drug eruption (one patient in group B). One additional patient experienced a hypersensitivity-related AE after receiving idarucizumab again following restart of dabigatran. Thrombotic events and hypersensitivity by bleeding location and type of surgery/procedure are listed in Supplementary Tables S7 and S8, respectively.
EffectivenessIn the effectiveness dataset (N = 793), 78 patients in group A and 26 patients in group B had both aPTT data at baseline and within 4 h of idarucizumab administration; in these patients, the median maximum percentage reversal within 4 h of idarucizumab administration was 100% (Table 3). Cessation of bleeding was confirmed in 146 of 208 patients (70%) who had intracranial hemorrhage, 271 of 349 patients (78%) who had non-intracranial hemorrhage, 104 of 132 patients (79%) who had any GI bleed, and 86 of 106 patients (81%) who had intrapericardial bleed (Table 4). Median time to recorded cessation of bleeding was 13.4, 3.3, 8.9, and 1.3 h in patients with intracranial hemorrhage, non-intracranial hemorrhage, any GI bleed, and intrapericardial bleeds, respectively (Table 4).
Table 3 Reversal of anticoagulation as measured by aPTTaTable 4 Time to cessation of all bleeding – group A/A + BAmong 252 patients in group B/A + B, 211 (84%) underwent surgery or had a procedure; 205 of the 211 patients who underwent surgery or required a procedure had at least one hemostasis assessment. Periprocedural hemostasis was normal in 166 of 205 patients (81%). The median time from administration of the first vial of idarucizumab to surgery or a procedure was 1.24 h (interquartile range, 0.50–2.50). For patients who required neurological surgery/procedure, vascular surgery/procedure, or abdominal surgery/procedure, the median times were 1.05, 1.40, and 1.43 h, respectively (Table 5). Many patients received transfusions and other blood products (48% in group A and 34% in group B), including packed red blood cells (37% in group A and 25% in group B), fresh frozen plasma (21% in each group), and platelets (7% in group A and 14% in group B). The use of blood products and volume expanders is described in Supplementary Table S9.
Table 5 Median time to surgery or invasive procedure after idarucizumab – group B/A + BThe 30-day mortality rate, estimated by the Kaplan–Meier method, was 12.0% in all patients included in the safety dataset. In group A/A + B, the mortality rate was 13.1% at day 30. At day 30, the mortality rate was 14.1% for patients who had intracranial hemorrhage, 16.7% for patients who had GI bleeding, and 4.8% for patients who had intrapericardial bleeding. In group B/A + B, the estimated mortality rate at day 30 was 10.4%. Patients who underwent neurological, vascular, or abdominal surgery/procedures had mortality rates of 8.4, 15.3, and 5.3% at day 30, respectively.
During the 4-week follow-up period after idarucizumab treatment, anticoagulation therapy was restarted in 329 patients (59%) in group A/A + B and 173 patients (69%) in group B/A + B, of which > 50% received dabigatran in each group (Table 6). After idarucizumab administration, median time to the restart of any anticoagulation therapy was 3.6 days in group A/A + B and 2.5 days in group B/A + B (Table 6). Restart of anticoagulation therapy and median time to restart of any anticoagulation therapy by bleeding location and type of surgery/procedure are provided in Supplementary Tables S10 and S11, respectively. Seven patients received idarucizumab again after dabigatran was restarted (Supplementary Table S12). One patient received an additional 5 g of idarucizumab before dabigatran was restarted, for a total of 10 g.
Table 6 Restart of anticoagulation therapy
Comments (0)