
Remember me

Primary aldosteronism (PA) is the underlying cause in 6% to 18% of patients diagnosed with hypertension.1 Patients with primary aldosteronism are at higher cardiovascular risk than patients with essential hypertension.2 However, less than 1% of patients with expected primary aldosteronism are ever formally diagnosed and treated.3 Recommended preoperative workup4–6 includes CT-scan and selective adrenal vein sampling (AVS) for all patients over 35 years of age and those with bilateral adrenal tumors to distinguish unilateral forms of primary aldosteronism amenable to surgery.
The need for AVS sampling has been well confirmed in a recent large retrospective study.7 However, recent publications still question its systematic use.8–10
Adrenalectomy for lateralized forms of primary aldosteronism results in complete resolution of hypertension (no antihypertensive drug and normal ambulatory blood pressure) in about one-third of the patients and complete biological success (normal kalemia and aldosterone/renin ratio) in 94% of the cases.11 These results are mainly drawn from large retrospective surgical series from expert centers with limited follow-up times (from months to 1 year usually).5,12–14 Predictive factors for the resolution of hypertension have been identified, but mostly from North American and Asian populations and none specifically in a representative national study.15 European series are scarce.16
The aims of the present work were (1) to describe the preoperative workup, (2) surgical results, (3) long-term results regarding clinical and biological success of adrenalectomy, and (4) variables associated with biological and clinical success in a French multicentric study using the Eurocrine® registry.
METHODS Study DesignThis is a multicentric nationwide retrospective cohort study using the Eurocrine® Registry (www.eurocrine.eu).
Eurocrine is an endocrine surgical quality registry. It is used to register operations for thyroid disease, primary and secondary hyperparathyroidism, adrenal surgery, paraganglioma, and neuroendocrine tumors of the gastrointestinal tract. Data are registered according to predefined data fields.
They include preoperative settings, diagnostic workup, surgery, hospital stay, pathology results, and up to 2 follow-up visits with clinical/biological assessments.
Data has been audited in Sweden and Switzerland and found to be valid and reliable17
All participating centers were notified 3 months before the extraction of the database and agreed to complete their data collection.
SettingData from 10 French medical centers (AFCE members) of patients who underwent adrenalectomy for unilateral PA from January 1, 2010 to December 31, 2020 were extracted.
The diagnostic criteria for PA were left to the discretion of each center. Data extraction from the Eurocrine platform was performed on September 24, 2022.
Exclusion criteria were surgery for another adrenal condition, lack of any follow-up data, and duplicates.
Database Quality ControlQuality assessment of the database was carefully conducted. The distribution of each variable was plotted; aberrant results were tracked. Duplicates were searched for using an anonymous database ID and by combining age, sex, date of surgery, center, and number of preoperative antihypertensive treatments.
Statistical AnalysisData analysis was performed using the R software version 4.0.3 (2020-10-10).
Statistical comparison between groups used χ2 for categorical variables and Student t test for numerical variables. A generalized linear model was used for multivariate analysis. P values <0.05 were considered significant. We did not adjust our P value thresholds for multiple comparisons.
Handling of Aldosterone and Renin DataAll aldosterone values were converted in pg/mL, and renin in mIU/L or ng/mL/h. Aldosterone/renin ratios (ARR) were normalized by an appropriate threshold value (according to units used) for primary aldosteronism, as described in French guidelines.4,18
Criteria for the use of AVSEach participating center was contacted to specify its criteria for using AVS.
DefinitionsComplete clinical success, and complete biological success were defined according to an international consensus from the PASO study.11
Briefly, complete clinical success (CCS) was defined as postsurgery normal blood pressure (systolic <140 mm Hg and diastolic <90 mm Hg) without the aid of antihypertensive medication; complete biological success as normokalemia and normalization of the ARR (should be measured postsurgery).
Antihypertensive medication was defined as the number of different classes of drugs, regardless of daily dose.
Obesity was defined as a body mass index (BMI) greater or equal to 30 kg/m2.
French Administrative DatabaseThe technical agency of the hospital stay information website (https://www.atih.sante.fr) was queried for adrenal surgery (surgical procedure) and primary aldosteronism (main diagnosis) from 2010 to 2020, leading to an average of 83 procedures/year.
Missing DataThe number (n) of data available for each variable is mentioned when different from the whole population.
The use of the Eurocrine® registry has been registered at ClinicalTrials.gov: NCT03410394.
This paper has been written following the STROBE checklist for cohort studies (https://www.strobe-statement.org/checklists/).
RESULTSOf the 769 French patients included in Eurocrine® Database for adrenal surgery, 385 (35/year on average) from 10 centers could be used for further analysis (Fig. 1). Reasons for exclusion were other indications for surgery (295 patients), lack of follow-up data (18 patients), and duplicates (32 patients).
 FIGURE 1:
FIGURE 1: Flowchart – Management of patients registered in the Eurocrine® database.
All patients underwent total unilateral adrenalectomy.
According to the French administrative database (https://www.atih.sante.fr), these 385 patients account for >40% of adrenalectomies performed in France each year (83/year average) for PA.
Patients were mainly women (57%), with a 5-year median history of hypertension. Thirty three percent were obese, 12% had a history of cardiovascular event (including stroke, myocardial infarction or ischemia, deep vein thrombosis or pulmonary embolism), 27% had normal blood pressure under antihypertensive medication, 43% were taking potassium supplementation, and 89% had an ARR above the threshold for primary aldosteronism (according to French guidelines).18 Patients’ full characteristics are presented in Table 1.
TABLE 1 - Baseline Characteristics of 385 Patients Variable N (%) Age at surgery, mean (SD), y 50 (11) Women 219 (57) American Society of Anaesthesiologists (ASA) score (n=293) 1 50 (17) 2 202 (69) 3 41 (14) 4 0 Current smoker (n=285) 52 (14) Body mass index (BMI), mean (SD), kg/m2 (n=355) <25 114 (32) [25–30] 124 (35) [30–35] 83 (23) [35–40] 24 (7) >40 10 (3) Dyslipidaemia (n=312) 51 (16) Type 2 diabetes (n=382) 42 (11) requiring insulin therapy (n=308) 11 (4) Previous cardiovascular event (n=312) No previous cardiovascular event 277 (88.5) Stroke 16 (5) Myocardial infarction or ischemia 13 (4) Deep vein thrombosis 7 (2) Pulmonary embolism 2 (0.5) Duration of hypertension, median [interquartile], y (n=328) 5 [2;12] Preoperative blood pressure, mean (SD), mm Hg (n=229) Systolic 148 (23) Diastolic 89 (13) <140/90, No. (%) 61 (27) Nb Antihypertensive drug before surgery (n=350) 0 6 (2) 1 120 (34) 2 97 (28) 3 74 (21) 4 39 (11) 5 12 (3.5) 6 2 (0.5) Including antialdosterone (spironolactone or eplerenone) 198 (57) Kalemia, mean (SD), mmol/L (n=330) 3.5 (0.7) <3.6 171 (52) Potassium supplementation (n=346) 148 (43) Serum creatinine, mean (SD), µmol/L (n=241) 81 (39) Serum aldosterone, median [interquartile], pg/mL, (n=283) 329 [210;520] >200 220 (78) <90 7 (2) Serum ratio aldosterone/renin>threshold (n=226) 201 (89)Patients’ characteristics.
The number of available data is mentioned at the end of the variable’s name when different from the whole population.
N: number of patients.
%: percentage.
Intervals are specified using [].
Preoperative workup details were available for 343 patients. All of them had a cross-sectional imaging. In all, 319 patients had a unilateral adrenal lesion and 99 of them had AVS. It was consistent with imaging in 77 patients, contradictory for 5 patients, and inconclusive in 17 patients. When imaging showed bilateral lesions or no lesion, AVS was almost systematic (12 over 15 patients and 8 over 9, respectively). We have no information on whether another imaging modality was used and how the side to be operated on was determined when AVS was not performed or inconclusive in these patients. In summary, lateralization workup (CT or MRI, and AVS when needed) was fully consistent with guidelines6 for only 137 (40%) patients. (Fig. 2).
 FIGURE 2:
FIGURE 2: Preoperative workup.
Each center was contacted to specify its criteria for using AVS. There was great heterogeneity between centers, some of which hardly ever used it, others which limited its use to specific situations (bilateral lesions on imaging, small lesions on imaging, large number of preoperative antihypertensive treatments), and others which strictly adhered to French recommendations. (Supplementary Table 1, Supplemental Digital Content 1, https://links.lww.com/SLA/E766).
Indeed, the use of AVS was associated with male gender, the number of preoperative antihypertensive treatments, and the size of the lesion on imaging (P<0.001) (Supplementary Table 2, Supplemental Digital Content 2, https://links.lww.com/SLA/E767). The use of AVS was not associated with an increase in CCS.
Pathology results found a cortical adenoma in 97% of the cases.
The last follow-up visits occurred at a median delay of 75 days after surgery. Mean blood pressure (mm Hg) was significantly reduced from 148 to 131 in systolic (P<0.001), as well as the mean number of antihypertensive medications from 2.2 to 0.9, and potassium supplementation from 57% to 3% patients. (Table 2).
TABLE 2 - Surgical Outcomes at Last Follow-up Visit Preop. Last follow-up Variable N (%) N (%) P (univ.) Time since surgery, median (interquartile), d 75 [43–514] — Cardiovascular event (n=312) (n=282) — No cardiovascular event 277 (88.5) 271 (96) — Stroke 16 (5) 2 (0.7) — Myocardial infarction or ischemia 13 (4) 2 (0.7) — Deep veinous thrombosis 7 (2) 1 (0.4) — Pulmonary embolism 2 (0.5) 0 — Other − 7 (2.5) — Ambulatory blood pressure, mean (SD), mm Hg (n=229) (n=271) — Systolic 148 (23) 131 (15) <0.001 Diastolic 89 (13) 80 (12) <0.001 <140/90 61 (27) 197 (76) 0.01 Nb Antihypertensive drug (n=350) (n=326) — 0 6 (2) 156 (48) — 1 120 (34) 91 (28) — 2 97 (28) 46 (14) — 3 74 (21) 20 (6) <0.001 4 39 (11) 11 (3) — 5 12 (3.5) 2 (0.6) — 6 2 (0.5) − — Including antialdosterone (spironolactone or eplerenone) 198 (57) 22 (5.7) — Kalemia, mean (SD), mmol/L 3.5 (0.7) 4.3 (0.5) <0.001 <3.6 171 (52) 7 (2.9) — Potassium supplementation 148 (43) 6 (3.1) — Complete clinical success (n=321) − 101 (31.5) — Complete biological success (n=69) − 51 (74) —The number of available data is mentioned at the end of the variable’s name when different from the whole population.
N: number of patients.
%: percentage.
P value is mentioned when significant (<0.05).
Finally, CCS was achieved in 31% of patients. (Table 2)
There was postoperative biological data available for only 69 patients, of which 74% (51) displayed complete biological success.
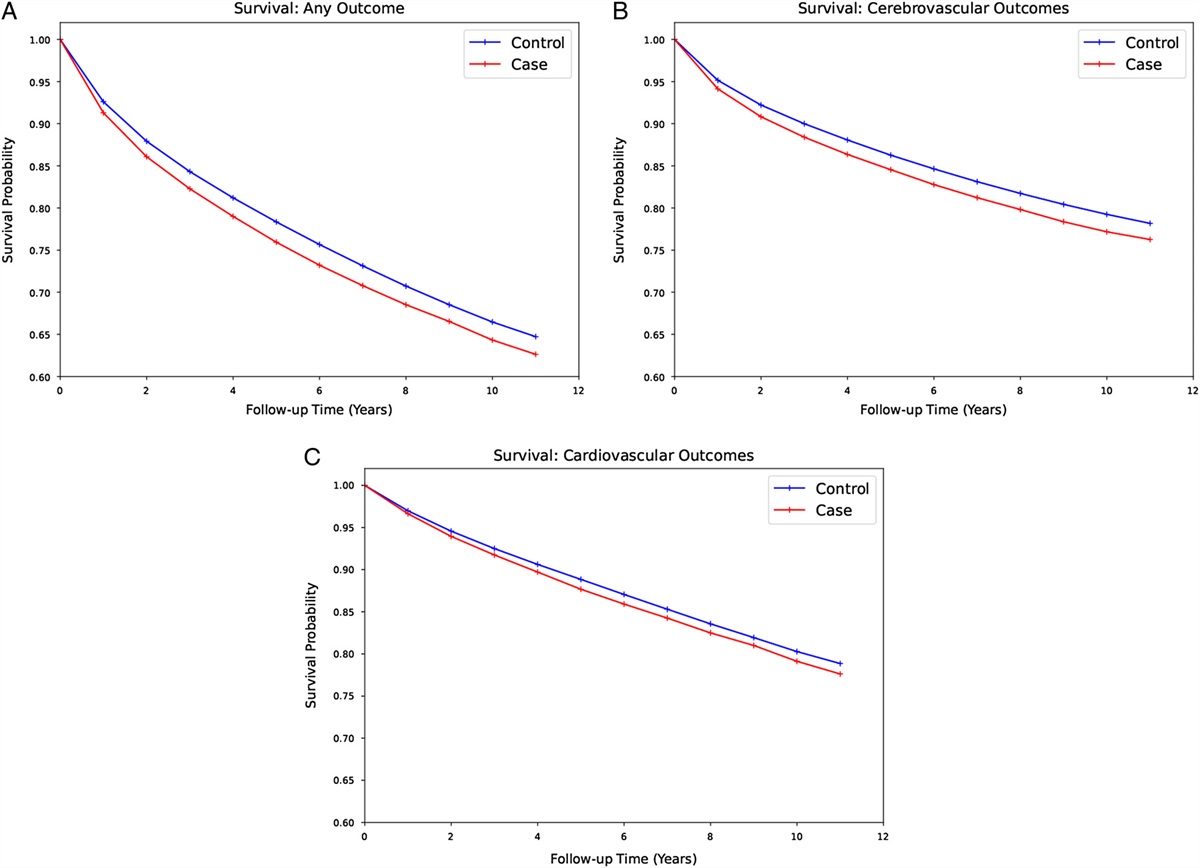
There were 12 cardiovascular events (2 strokes, 2 myocardial infarctions, 1 deep vein thrombosis, and 7 other events, mainly atrial fibrillation) during follow-up.
CCS at successive follow-up visits were not fully persistent (Fig. 3). Of the 92 patients considered as CCS at the first follow-up (median 43 d), 15 had contradictory results at the second follow-up (median 377 d) due to the resumption of antihypertensive treatment. In contrast, of the 208 patients that were not considered CCS at the first follow-up, 20 were estimated CCS at the second follow-up. On average, for patients with 2 informative follow-up visits, clinical status (success or not) was not persistent for one-fifth of patients.
 FIGURE 3:
FIGURE 3: A Complete clinical success persistence. N/A not available: complete clinical success could not be assessed due to missing data. Follow-up delays are given as Median [interquartile]. B Preoperative indicators of complete clinical success. Univariate P values are displayed when <0.1 and considered significant <0.05. Multivariate analysis was performed using generalized linear model including age, body mass index (BMI), duration of hypertension, number of antihypertensive drugs before surgery, and serum creatinine. In all, 189 patients with the full data set for these variables were available for analysis. Dyslipidaemia and systolic blood pressure were considered associated with BMI and the number of antihypertensive drugs and were not included in the analysis.
We finally sought to identify the original factors associated with CCS. On univariate analysis, younger age, lower BMI, less dyslipidaemia, shorter duration of hypertension, lower systolic blood pressure, lower number of antihypertensive drugs, and lower serum creatinine levels were associated with complete clinical success. On multivariate analysis, BMI and dyslipidaemia, blood pressure, and the number of antihypertensive drugs were considered to interact, and only BMI and the number of antihypertensive drugs were used in the regression. On multivariate analysis, only BMI, duration of hypertension, and the number of antihypertensive drugs remained significantly associated with CCS.
DISCUSSIONThis nationwide retrospective cohort study describes the French practice of surgery for primary aldosteronism over the last 11 years.
Preoperative AVS was “adequately” performed in only 40% of patients, according to the French guidelines. The median follow-up was only 75 days, while complete clinical success was lost for 20% of patients between follow-up at 1 month and 1 year. Biological success is rarely evaluated, even though it is the most reliable marker of the success of the surgery, by suppression of the hormone secretion syndrome.
This low adherence to the guidelines has several explanations. Only 1 randomized study compared CT-scan alone with AVS and CT-scan for the characterization of lateralized primary aldosteronism.8 It showed no significant difference in success after surgery regarding clinical and biological outcomes. Interestingly in this study, CT-scan and AVS were both performed in the AVS group, and a 50% discordance in lateralization was observed. Other studies reported a 36% discordance19 of CT-scan compared with AVS, 2% being a change in lateralization and 24% affirmation of lateralization when CT-scan failed to do so. The recent AVIS-2 study7 showed a difference in outcomes after adrenalectomy when AVS was performed (40% CCS vs 30.5% P=0.027). This study's inclusion criterion was AVS realization rather than surgery, and it suffers less selective bias than retrospective surgical studies.
In the present work, there was no correlation between CCS and the completeness of preoperative workup (40% vs. 32% P=0.23) even though these results are similar to those reported by Rossi et al. A lack of power in our study could explain the difference (385 vs. 1625 patients in the AVIS-2 study). Moreover, AVS use was biased towards patients with risk factors of hypertension persistence (male gender, high number of antihypertensive drugs), making it difficult to assess its relevance. We had only a few changes in lateralization due to AVS, but we are missing all the patients that did not go to surgery due to such contradictory results. After discussion with participating centers, there was a trend to use medical treatment as the first line in patients with normal imaging, without performing AVS to look for lateralization, which could explain the low level of patients with no lesion on imaging in our study.
As expected, surgery was associated with significant improvement in ambulatory blood pressure, kalemia, and the number of antihypertensive drugs. CCS at last follow-up was achieved in 31% of patients, consistent with previous reports.11,20 Interestingly, for patients with 2 follow-up visits (usually early postsurgical evaluation and 1-year follow-up), there was a change in clinical status for one-fifth of patients. This is contradictory with recent results21 questioning the need for routine follow-up in referral centers. In the study from Suurd et al, defined daily doses of antihypertensive drugs were found to be stable from 1 month to 1 year postoperatively. Nevertheless, of the 20 patients with no treatment postsurgery, 11 had to restart antihypertensive medication during follow-up.
Predictors of complete clinical success on multivariate analysis were BMI, the duration of hypertension, and the number of hypertensive drugs. Several studies have shown various predictors of complete clinical success.12–15 They variably found sex, age, BMI, duration of hypertension, number of antihypertensive drugs, and serum creatinine as factors associated with CCS, and none of these models were developed in a homogenous European population, and they lacked performance when applied to a French population.16 Surprisingly, no study has yet used these predictors to refrain surgery.
Using models predicting complete clinical success to choose between surgery and medical treatment should be considered with caution. Adrenalectomy, when feasible, has shown, over the year, its superiority over medical treatment for the prevention of major cardiovascular events, all-cause mortality, and improvement of quality of life.22,23
Most predictors of clinical success are only risk factors of essential hypertension, probably concomitant with primary aldosteronism.24 Biological success (ie, a normal postsurgery ARR) should be the most regarded parameter. Indeed, patients with primary aldosteronism (medically treated) matched with patients with essential hypertension showed similar incidences of cardiovascular events only if antialdosterone treatment was sufficient to achieve plasma renin activity >1 µg/L/h).25 Surgeons should conscientiously check biological success to ascertain the benefit of the surgery and quickly restart antialdosterone regimen when needed.
Future cohort studies should assess the clinical significance of complete clinical success versus complete biological success in light of incident cardiovascular events over long follow-up periods. Hypertension has always been used and described in the context of essential hypertension as a surrogate of cardiovascular events, with a 10 mm Hg decrease in systolic pressure corresponding to a 20% risk reduction in major cardiovascular events.26 However, when matched for hypertension, primary aldosteronism patients had more cardiovascular events.2 The intuitive correlation between mortality and blood pressure does not necessarily hold in the context of primary aldosteronism. Other surrogates of cardiovascular risk, independent of hypertension, should be identified to better assess the beneficial effect of adrenalectomy for primary aldosteronism.27
This cohort accounts for >40% of surgery for primary aldosteronism over the study period in France. Given the prevalence of hypertension in France (31% in 2006 for people between 18 and 74 years old),24 the French population between 18 and 74 years old (47 million in 2022, according to the INSEE), the 6% to 18% underlying PA in patients with hypertension, and the 14% patients with PA with found lateralization when AVS is performed,20 there are over 100 000 patients with primary aldosteronism that remain to be identified and properly handled.
There is an urgent need for public health policies to detect and treat all these patients.28
Our work has several limitations. The number of missing data is substantial, often because it was not recorded in the patient’s file, rather than a lack of data collection in the database. Follow-up is very limited. There is a selection bias because participating centers were all tertiary centers and members of the French-Speaking Association of Endocrine Surgery. Only patients that underwent surgery are available for analysis, and we have no information regarding medical treatment and AVS use for patients that are sometimes treated medically without complete lateralization assessment. AVS use was often biased with no consensual indication.
CONCLUSIONThis large retrospective nationwide study reliably reflects French practice. Preoperative workup was consistent with French and international guidelines for only 40% of the patients. Complete clinical success at the last follow-up was achieved in 31% of patients, and complete biological success in 74% of patients, with only a few data available. Complete clinical success between consecutive follow-up visits was not consistent for one-fifth of patients, which calls for long-term follow-up to early detect and treat hypertension and/or primary aldosteronism relapse. Biological success was insufficiently evaluated and should be part of routine postoperative workup.
DISCUSSANT Elisabeth JM Nieveen van Dijkum (Amsterdam, The Netherlands)The data are well analyzed, and reported results included some 40% adherence to preoperative workup protocols, and a clinical/biological success in 31/74% of patients. The study concluded that the preoperative workup should be improved, and the long-term follow-up should be implemented to detect a relapse of hypertension. It is important to note that only limited reflection is shown towards the data quality assessment in this study. Probably, some discussion on the registry and the completeness of the data set could have been added. Therefore, this discussion will highlight 3 important points that can be addressed with the quality of the data in mind.
The first point concerns the low number of patients (around 100,000 in 10 years) diagnosed and operated for primary hyperaldosteronism. As is stated, that only 83 patients are operated per year in France for primary hyperaldosteronism. The 10 clinics included in this study performed 3.5 operations per clinic per year. Studies on rare diseases are always limited by the lack of volume. Many studies describe a correlation between volume and outcome with different volumes per year, per intervention. It is unclear whether the data from hospitals performing 3.5 interventions per year can be considered as high-quality data. Regionalization and centralization are the main important incentives to facilitate less centers, and thereby, high-volume centers. High-volume centers are known to improve outcome for patients with rare diseases, for example, by low failure-to-rescue rates. High-volume centers will also influence the reliability of the data, mainly because of more standardized workflows. The lack of standardized workflows is pointed out, with only 40% of patients having the properative workup as described in international guidelines. The authors state that this might be explained by the relatively low level of evidence supporting the guidelines on preoperative workup. However, is low adherence to the protocol not also an indication of low-volume centers? Irrespective of the clinical outcome, this lack of standardization shows the heterogeneity of the clinics and the data. This also raises the question of whether combining heterogeneous data provides a solid basis for outcomes.
The second point to be discussed is the outcome measure for clinical and biological success. Patients operated on because of primary hyperaldosteronism were defined as a “complete clinical success” if they had a normal blood pressure without any anti-hypertension medication. The hypertension outcome is known to be a very difficult outcome parameter, often with missing values and missing information on the measurements. Possibly, the aldosterone/renin ratio (ARR) is a more reliable outcome measure, especially since current insights describe aldosterone levels to be associated with cardiovascular risk. Therefore, the clinical success normotension might not be the preferred outcome for all patients. It is probably more important to measure normalization of the aldosterone/renin ratio (ARR), as was defined in the biological outcome. Only 69 of the 385 (18%) patients were analyzed for biological success, with a biological success of 51/69 (74%). The importance of data registration is once more shown by these outcome measures. For example, if the methods section of the study had included a data quality measure, the measure that at least 80% of the primary outcome data should be available, this outcome would not have been included in the analysis. As for the clinical success rate, this was available for only 300/385 (78%) patients 32 to 55 days after surgery and for 168/385 patients (44%) after 1 year. Biological outcome measurements were available for 18% of patients.
The final point of this discussion concerns the efforts of all clinicians, students, researchers, nurses, and all other data handlers, who dedicated time to include patients in the registry. The transfer of data is still a process of people typing the data from one record into a registry, with chances of mistakes, misinterpretations, and missing data. This study highlights the enormous amount of work that it takes to include 385 patients, with only 78%, 44%, 40%, and 18% of data completeness on the primary outcomes (clinical complete response in the short- and long-term/peroperative workup and biological response, respectively).
For prospects, one would first hope for the number of clinics performing adrenalectomies to be reduced, which would improve patient care and data standardization. These high-volume clinics would then publish their data, based on international standards, yearly on their websites. This would facilitate outcome measures to be reported straight from the hospital data records without copying data. If the outcome of all high-volume hospitals is published in a standardized way, the use of a registry is no longer necessary, reducing the heavy workload and effort for the data transfer. Alternatively, if we wish to keep registries, then data should be directly obtained from hospital records, again reducing the amount of effort currently required.
This French study on adrenalectomy for primary hyperaldosteronism provides some insight into current practice and provides clear data for improvements. The clinics involved in this study, and clinics all over the world performing this operation, are invited to discuss centralization and regionalization, thereby improving the documentation of diagnosis and treatment outcomes. Endocrine surgeons are also invited to define the preferred outcome parameter for adrenalectomy in primary hyperaldosteronism, with the knowledge that current outcome measures are troublesome. All described efforts will be beneficial for improved patient care.
Response From Timothee Vignaud (Nantes, France)Thank you very much for your constructive comments. To answer your first point, we checked whether AVS (adrenal vein sampling) use was correlated with the number of procedures performed at each center. There was no correlation. We had a few high-volume centers that didn’t perform it at all, while some small centers that followed the guidelines meticulously. I agree that centralization in high-volume centers would enable us to publish high-quality, standardized data; however, adrenalectomy for primary hyperaldosteronism is not a very challenging intervention. Centers also often perform the intervention for pheochromocytoma or adrenocortical cancer. This means that the 3.5 interventions per year can mask that they are also performing many adrenal surgeries for other diseases. I don’t think that surgery for Conn disease is the problem; instead, having a good selection of patients, added to the fact that AVS is not easily available everywhere, are the real issues. It’s true that we should have centers that are able to perform a proper diagnostic workup.
Regarding your second point about the long follow-up and importance of biological over clinical success, I completely agree with you. In fact, when starting this study, our hope was to have cardiovascular events and biological success data to make a correlation between the two. So, the purpose would indeed be to have these results in the long-term, especially when it comes to biological success. The factors that are found to be correlated with the lack of complete clinical success are also associated with the risk of idiopathic hypertension. We show that the patients we failed to clinically cure of their primary aldosteronism were likely to have an underlying idiopathic hypertension. This is not a good outcome. Biological outcome should be preferred.
We also have a new tool for confirming the effectiveness of surgery. According to the new WHO classification for primary hyperaldosteronism, it is now required to perform an immunostaining, which can prove that the lesion was producing aldosterone. I think that this will also be a breakthrough.
Menno Vriens (Utrecht, The Netherlands)Thank you for this beautiful study. It’s clear that the guidelines should be changed. However, with all the knowledge that you have gained, what would your ideal workup be? For example, should we perform adrenal vein sampling for everyone? Second, can we make the follow-up much shorter than what it is now? Of course, if you have existential hypertension issues, clinical success is not able to gain, but if you have both biological and clinical success, then, in my opinion, you could stop the follow-up within 6 months. Third, did all patients receive a total adrenalectomy, or were there also patients who received a sub-total adrenalectomy?
Response From Timothee Vignaud (Nantes, France)I will start with your third question. They all had a total adrenalectomy. Regarding the ideal workup and the follow-up duration, I think that we shouldn’t change both things at the same time because, if we reduce the follow-up, but still have centers that are not doing the diagnosis properly, we won’t be able to draw proper conclusions. I think we should perform AVS for everyone. There is a randomized trial, which studied CT-scan alone or CT-scan plus AVS, but in the latter arm, you had both. You could tell which ones were operated on with AVS and which ones would have been operated on according to CT-scans only. You only had a 50% concordance for the patients operated on, which is puzzling (Dekkers, Lancet Diab Endoc, 2016). They still had good clinical and biological success in the CT-scan alone group because, from what we know in the CT-scan and AVS group, the patients that would have been wrongly operated on with CT-scan alone were people that had bilateral aldosterone production on AVS. So, maybe it is worth removing half of the adrenal volume in these patients. They won’t be cured, but at least, there will be an improvement. If you only have a CT-scan as the preoperative workup, I suggest a longer follow-up because you have a risk of bilateral aldosterone production that is somewhat masked postoperatively. If we succeed in having a proper preoperative workup, then we can move to shorter follow-ups, if we have proven that a longer period is not necessary.
Andrea Frilling (London, United Kingdom)Thank you for showing us your data, and even more importantly, for showing us that there is much room for improvement in the management of this rare disease. If I understood you correctly, surgical cure was only achieved in about 32% of your patients. Bearing this number in mind, what is your opinion on nonsurgical procedures, such as endoscopically guided radiofrequency ablation or percutaneous ablation of a nodule in the adrenal gland? Do you have any experience with these technologies?
Response From Timothee Vignaud (Nantes, France)No, I don’t. The problem is that we can obtain a response with the adrenal vein sampling on the side, but we can have a non-producing adenoma in an adrenal unilateral hyperplasia, and then, we don’t know what to target with selective treatments. So far, we don’t have a strong enough pathology result to know how often it happens. Maybe the new WHO pathology classification will answer this question.
References 1. Baguet J-P, Steichen O, Mounier-Véhier C, et al. SFE/SFHTA/AFCE consensus on primary aldosteronism, part 1: epidemiology of PA, who should be screened for sporadic PA? Ann Endocrinol (Paris). 2016;77:187–191. 2. Monticone S, D’Ascenzo F, Moretti C, et al. Cardiovascular events and target organ damage in primary aldosteronism compared with essential hypertension: a systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2018;6:41–50. 3. Liu Y-Y, King J, Kline GA, et al. Outcomes of a Specialized Clinic on Rates of Investigation and Treatment of Primary Aldosteronism. JAMA Surg. 2021;156:541–549. 4. Amar L, Baguet JP, Bardet S, et al. SFE/SFHTA/AFCE primary aldosteronism consensus: Introduction and handbook. Ann Endocrinol (Paris). 2016;77:179–186. 5. Funder JW, Carey RM, Fardella C, et al. Case detection, diagnosis, and treatment of patients with primary aldosteronism: an endocrine society clinical practice guideline. J Clin Endocrinol Metab. 2008;93:3266–3281. 6. Wu J, Tian W, Zhang L, et al. Assessing the quality of guidelines for primary aldosteronism: which guidelines are worth applying in diverse settings? Hypertension. 2019;37:1500–1512. 7. Rossi GP, Rossitto G, Amar L, et al. Clinical outcomes of 1625 patients with primary aldosteronism subtyped with adrenal vein sampling. Hypertension. 2019;74:800–808. 8. Dekkers T, Prejbisz A, Kool LJS, et al. Adrenal vein sampling versus CT scan to determine treatment in primary aldosteronism: an outcome-based randomised diagnostic trial. Lancet Diabetes Endocrinol. 2016;4:739–746. 9. Thiesmeyer JW, Ullmann TM, Stamatiou AT, et al. Association of adrenal venous sampling with outcomes in primary aldosteronism for unilateral adenomas. JAMA Surg. 2021;156:165–171. 10. Rossitto G, Amar L, Azizi M, et al. Subtyping of primary aldosteronism in the AVIS-2 study: assessment of selectivity and lateralization. J Clin Endocrinol Metab. 2020;105:dgz017. 11. Williams TA, Lenders JWM, Mulatero P, et al. Outcomes after adrenalectomy for unilateral primary aldosteronism: an international consensus on outcome measures and analysis of remission rates in an international cohort. Lancet Diabetes Endocrinol. 2017;5:689–699. 12. Wachtel H, Cerullo I, Bartlett EK, et al. Long-term blood pressure control in patients undergoing adrenalectomy for primary hyperaldosteronism. Surgery. 2014;156:1394–1402; discussion1402-1403. 13. Utsumi T, Kamiya N, Endo T, et al. Development of a novel nomogram to predict hypertension cure after laparoscopic adrenalectomy in patients
Comments (0)