
Remember me

Intestinal transplantation (ITx) is a life-saving procedure for patients suffering from intestinal failure (IF) and complications of long-term parenteral nutrition (PN). However, the outcome remains hampered by surgical complexity, graft susceptibility to ischemia/reperfusion, and rejection.1–3 Living donation (LD) holds the potential of improving ITx outcome by better graft quality and HLA-matching, reducing cold ischemia time and suppressing waiting time.4,5 Gruessner and Sharp described the first standardized procedure for intestinal LD and transplantation in 1997.6 Since then, the technique has spread worldwide.5,7 Most of the literature on LD-ITx originates from case reports or single-center series until recently. Gruessner reported the first descriptive analysis of an international LD-ITx cohort based on literature.8
The International Intestinal Transplant Registry (ITR) was created by the Intestinal Transplantation Association in 1985 to centralize global ITx-activity. In 2014, the ITR was estimated to capture 95% of ITx-experience, from more than 27 countries.9 No matched comparison has been performed between LD and deceased donation (DD)-ITx. We aim to provide a descriptive analysis of the worldwide LD-ITx–experience and compare it with a propensity-matched DD-ITx cohort.
METHODS Study-design and PopulationThe data of this retrospective, multicenter, observational and matched-cohort analysis were extracted from the ITR after approval by the Intestinal Rehabilitation and Transplantation Association (IRTA) (May 17, 2019). In all, 4156 ITx were performed between January 9, 1987 and April 17, 2019, divided into different graft types: isolated ITx, combined liver-ITx (cLi-ITx), multivisceral (MvTx), and modified multivisceral. Exclusion criteria were unknown donor type and unreliable data.
Descriptive AnalysisData collected for descriptive analysis were: geographical distribution, donor/recipient age, waiting-list duration, recipient body mass index, recipient sex, pretransplant status, ABO compatibility, HLA mismatches (donor/recipient discrepancy for HLA-A, -B, -DR), graft type, simultaneous kidney transplant, indication, hospitalization, immunosuppression (induction/maintenance), acute rejection, 1-/5-year patient and graft survival, renal replacement therapy (RRT), serum creatinine level (last follow-up), posttransplant lymphoproliferative disease (PTLD) and infection. In addition, 2 subanalyses within the LD cohort were performed: (1) pediatric (<18 y) versus adult recipients; and (2) low-volume (N=1) versus medium-volume (N=1-6) versus high-volume (N≥6) centers (N=total volume/center).
Propensity-score MatchingFrom a total of 76 LD-ITx, 64 (86%) were isolated ITx. To reduce confounding, only this graft type was selected for matching. The other graft types [ITx-colon (n=7), cLi-ITx (n=5)] were excluded. The propensity score was calculated using the following data: recipient age, sex, weight, region, indication, graft number, pretransplant status [home, hospitalized, intensive care unit (ICU)], ABO compatibility, immunosuppression (induction/maintenance) and transplant year.
A multiple imputation model compensated for missing data: 100 imputed data sets per missing data were created based on matching variables and outcomes (patient survival and graft removal) to obtain a mean propensity score for each patient. Using a greedy matching algorithm with 0.7caliper, LD patients were matched to DD through the log-it of their mean propensity score (1:4 fashion).
OutcomePrimary outcome included acute rejection and 1-/5-/10-year patient survival. Secondary outcomes were patient status (last follow-up), graft function, cause of graft removal, 1-/5-/10-year graft survival, RRT, serum creatinine level (last follow-up), PTLD, and infection. Patient status was defined as alive (with functioning graft or graft removed) or dead/lost to follow-up. Graft function was defined as dependence (/not) on PN/intravenous fluids. Causes of graft loss/removal were patient death, rejection, PTLD, poor graft function, infection, surgical complications, and other.
StatisticsDescriptive data were analyzed using GraphPadPrism9.3.1. Matched-cohort analysis was performed using SAS9.4. Continuous variables were reported by median (min-range) for posttransplant hospitalization by mean±SD. Categorical variables were characterized using absolute numbers/frequencies (%). Groups were compared using 2-sample t-test for continuous and χ2/Fisher exact for categorical variables. Statistics were 2-sided and assessed at a significance level of 0.05. No adjustments were made for multiple comparisons.
Among the analyzed outcomes, acute rejection, patient status, graft function, and reasons for graft removal were compared using χ2 test. Patient/graft survival was assessed using Kaplan-Meier and log rank. Patients who survived with functioning grafts were censored at the last follow-up.
RESULTS Study Population (Supplemental Digital Content, Figure 1, https://links.lww.com/SLA/E824)The ITR recorded 4156 ITx, of which 69 were excluded for unknown donor type and 46 for unreliable data (LD cohort: 6 MvTx, 1 duodenum-inclusive graft, 1 unknown graft type; DD cohort: 21 unknown graft types, 17 grafts without ITx). The 4041 remaining were divided according to donor type: 76 LD-ITx (2%), 3965 DD-ITx (98%).
Demographic Analysis of Overall Living versus Deceased Donation Cohort (Supplemental Digital Content, Table 1, https://links.lww.com/SLA/E822)Among 76 LD-ITx, 43 (57%) were performed in North America (31 in Illinois, Chicago), and 19 (25%) in Middle-East/Asia (see Figure, Supplemental Digital Content 1, https://links.lww.com/SLA/E781 geographical distribution). Donor age [31.5years (18 to 61)] was higher compared with the DD cohort [(8 (0 to 65); P<0.001)]. Recipient age was similar for LD and DD [17.8 y (0.6 to 60) versus 16 (0 to 73.3); P=0.746]. Waiting-list time for LD was shorter compared with DD (0 months (0 to 32) versus 3.8 (0 to 131); P=0.012). Regarding pretransplant status, 39 (51%) LD recipients were home and 37 (49%) were hospitalized [3 (4%) in ICU]. In contrast, a larger proportion of DD cohort (71%) were home (P<0.001). Eighty-one percent of LD/recipient pairs were ABO-identical versus 85% in the DD cohort (P=0.432). Ninety-five percent of the LD/recipient pairs had ≤3 HLA mismatches versus 13% in the DD cohort (P<0.001). In the LD cohort, 71 (93%) received an isolated ITx (7 with colon) and 5 (7%) cLi-ITx. In contrast, 62% of the DD cohort received combined grafts (29% cLi-ITx, 22% MvTx, 10% modified multivisceral), whereas 38% underwent isolated ITx (6% including colon) (P<0.001). No kidneys were included with the LD versus 207 (5%) in the DD cohort (P=0.032). Leading transplant indications in LD were short bowel syndrome (SBS) 75% versus 59% in the DD cohort (P=0.004); and motility disorders 13% versus 14% in the DD cohort (P>0.999). Most frequent maintenance immunosuppression in LD were calcineurin inhibitors (86%) and steroids (82%) versus calcineurin-inhibitors (95%) (P=0.057) and steroids (79%) in DD (P=0.246). Three LD recipients (4%) were off immunosuppression versus 1% in the DD cohort (P=0.03).
Posttransplant hospitalization was 114 days (±162) in the LD cohort versus 75 (±75) in the DD cohort (P=0.008). The acute rejection rate was 50% in LD versus 44% in DD (P=0.444). One-/5-year patient survival was 74%/52% for LD versus 74%/54% for DD (P=0.986/0.779). One-/5-year graft survival was 61%/44% for LD versus 68%/46% for DD (P=0.155/P=0.335). No significant difference was observed between the 2 cohorts regarding renal function posttransplant (RRT: 9% vs. 6% (P=0.485); creatinine level: 0.88mg/dl versus 1.3mg/dl (P=0.223); for LD cohorts and DD cohorts, respectively). PTLD and infection rates were similar between both groups.
Pediatric versus Adult Recipients (Supplemental Digital Content, Table 2, https://links.lww.com/SLA/E823)Of 76 LD, 39 (51%) recipients were pediatric (<18 y). Donor age was 27 years (19 to 56) and lower than in adult recipients (34 (19.2 to 60); P=0.005). Children were more often hospitalized pretransplant compared with adults (72% vs. 24%; P<0.001) and received less ABO-identical organs (68% vs. 93%; P=0.036). All 5 cLi-ITx recipients were pediatric. The main transplant indication was 72% SBS in pediatrics versus 78% in adults (P=0.6), followed by 15% motility disorders versus 11%, respectively (P=0.737). Posttransplant hospitalization was 192 days (±214) in pediatrics versus 47 (±39) in adults (P=0.006). The acute rejection rate was 48% in pediatrics versus 52% in adults (P>0.999); 1-/5-year patient survival for pediatrics and adults was 71%/52% versus 78%/52% (P=0.444/P=0.684); and 1-/5-year graft survival was 59%/46% versus 64/41%, respectively (P=0.580/P=0.794). Dividing the study-period in 3 era, short-term outcomes improved over time (see Table/Figure, Supplemental Digital Content 2, https://links.lww.com/SLA/E781 survival according to transplant-era).
LD-ITx Center Volume (Supplemental Digital Content, Table 2, https://links.lww.com/SLA/E823)The LD-ITx–activity was distributed among 21 centers. From 76 LD-ITx, 8 (11%) were transplanted in 8 low-volume, 37 (49%) in 12 medium-volume, and 31 (41%) at a single high-volume center(s) (Illinois, CA). One-/5-year patient survival was 75%/50% for low-volume, 77%/53% for medium-volume, and 71%/50% for high-volume center(s) (P=0.891/P=0.951). One-/5-year graft survival was 37%/25% for low-volume, 67%/41% for medium-volume, and 61%/51% for high-volume center(s) (P=0.375/P=0.373).
Propensity-matched AnalysisSixty-four LD-isolated ITx were matched with 1215 DD-isolated ITx (1:4 fashion). Within the LD-ITx cohort, 37 patients had 4 matches, 4 had 3 matches, 4 had 2 matches, 18 had 1 match, and 1 had no match (excluded), resulting in 63 LD-ITx versus 186 DD-ITx, for propensity-matched analysis. Demographic variables, indications and immunosuppression were similar between both cohorts (Table 1).
TABLE 1 - Propensity-Matched Cohort Analysis of Intestinal Transplantation From Living Versus Deceased Donors Statistic LD-ITx (N=63) DD-ITx (N=186) P Variables used for matching Age at transplant (y) Median (min–max)(n) 20 (0.6–57)(63) 20 (0–73)(186) 0.406 Weight at transplant (kg) Median (min–max)(n) 42 (5–93)(43) 45 (5–107)(126) 0.775 Recipient gender — — — 0.954 Female n/N (%) 26/63 (41) 76/186 (41) — Male n/N (%) 37/63 (60) 110/186 (59) — Region — — — 0.447 Europe n/N (%) 6/62 (10) 13/180 (7) — North America n/N (%) 38/62 (61) 126/180 (70) — Middle-East/Asia n/N (%) 18/62 (29) 41/180 (23) — Indication Short bowel syndrome n/N (%) 53/63 (84) 143/186 (77) 0.286 Motility disorder n/N (%) 5/63 (8) 20/186 (11) 0.633 Tumor n/N (%) 3/63 (5) 2/186 (1) 0.105 Other n/N (%) 1/63 (2) 12/186 (6) 0.194 Mucosal Defect n/N (%) 1/63 (2) 5/186 (3) >0.999 Retransplant n/N (%) 0/63 (0) 4/186 (2) 0.575 Graft Number — — — 0.972 1 n/N (%) 57/60 (95) 167/176 (95) — 2 n/N (%) 3/60 (5) 9/176 (5) — Pretransplant status — — — 0.138 Home n/N (%) 33/63 (52) 112/185 (60) — Hospitalized n/N (%) 29/63 (46) 73/185 (40) — ICU n/N (%) 1/63 (2) 0/185 (0) — ABO Compatibility — — — 0.838 Identical n/N (%) 37/41 (90.2) 98/110 (89) — Compatible n/N (%) 4/41 (9.8) 12/110 (11) — MIS None n/N (%) 3/63 (5) 5/186 (3) 0.420 Anti-Lymphocyte n/N (%) 19/63 (30) 49/186 (26) 0.557 Mycophenolate Mofetil Cept/Myfortic n/N (%) 18/63 (29) 38/186 (20) 0.181 Tacrolimus n/N (%) 52/63 (82) 159/186 (86) 0.574 Orthoclone n/N (%) 6/63 (10) 12/186 (6) 0.416 Cyclophosphamide n/N (%) 3/63 (5) 3/186 (2) 0.159 Cyclosporine n/N (%) 3/63 (5) 6/186 (3) 0.572 Steroids n/N (%) 51/63 (81) 143/186 (77) 0.501 Rapamycine n/N (%) 6/63 (10) 17/186 (9) 0.928 IL-2 Antagonist n/N (%) 9/63 (14) 25/186 (13) 0.866 Other n/N (%) 14/63 (22%) 35/186 (19%) 0.557 Year of tranplant — — — 0.231 ≤ 1994 n/N (%) 2/63 (3) 10/186 (5) 1995–1999 n/N (%) 15/63 (24) 32/186 (17) 2000–2004 n/N (%) 23/63 (36) 51/186 (27) 2005–2009 n/N (%) 14/63 (22) 56/186 (30) 2010–2014 n/N (%) 5/63 (8) 30/186 (16) 2015–2019 n/N (%) 4/63 (6) 7/186 (4) — Variables not used for matching Height at transplant (cm) Median (min–max)(n) 160 (61–185)(41) 157 (58–193)(118) 0.730 BMI at transplant (kg/m²)(>18y) Median (min–max)(n) 20 (14–29)(24) 22 (14–37)(65) 0.139 HLA mismatch — — — <0.001 ≤3 n/N (%) 36/39 (92) 21/112 (19) — >3 n/N (%) 3/39 (8) 91/112 (81) — Primary outcome Acute rejection n/N (%) 16/34 (47) 25/49 (51) 0.723 Patient Survival — — — 0.826 1 y Est. (95% CI) 74 (61;83) 80 (74;85) — 5 y Est. (95% CI) 50 (36;62) 48 (40;55) — 10 y Est. (95% CI) 46 (32;58) 39 (31;46) — Secondary Outcome Patient status — — — 0.920 Alive (functioning graft) n/N (%) 17/63 (27) 55/186 (30) — Graft removed n/N (%) 12/63 (19) 33/186 (18) — Death/Lost to follow-up n/N (%) 34/63 (54) 98/186 (53) — Graft function — — — 0.127 Full function n/N (%) 21/30 (70) 56/103 (54) — Partial or no function* n/N (%) 9/30 (30) 47/103 (46) — Cause for graft removal — — — 0.082 Rejection n/N (%) 13/18 (72) 45/51 (88) — PTLD n/N (%) 1/18 (6) 2/51 (4) — Poor graft function n/N (%) 1/18 (6) 2/51 (4) — Infection (non-PTLD) n/N (%) 0/18 (0) 1/51 (2) — Surgical n/N (%) 0/18 (0) 1/51 (2) — Other n/N (%) 3/18 (17) 0/51 (0) — Graft Survival (nonsensitized to death) — — — 0.956 1 Year Est. (95% CI) 60 (47;71) 69 (62;75) — 5 Year Est. (95% CI) 41 (28;52) 36 (29;43) — 10 Year Est. (95% CI) 33 (21;45) 26 (20;34) — Kidney function — — — — Need for RRT n/N (%) 2/24 (8) 3/60 (5) 0.621 Dialysis n/N (%) 1/2 (50) 1/3 (33) >0.999 Kidney transplant n/N (%) 1/2 (50) 2/3 (67) >0.999 No RRT described n/N (%) 0/2 (0) 0/3 (0) >0.999 Creatinine at follow-up (mg/dl)(>18y) Median (min-max)(n) 0.88 (0.25–4.3)(11) 1.1 (0.58–3.05)(13) 0.768 Complications PTLD n/N (%) 1/38 (3) 7/116 (6) 0.680 Infection n/N (%) 5/63 (8) 8/186 (4) 0.324*Dependence on parenteral nutrition or intravenous fluids.
BMI indicates body mass index; CI, confidence interval; DD-ITx, deceased donation intestinal transplantation; ICU, intensive care unit; IL-2, interleukin 2; ITx, intestinal transplantation; LD-ITx, living donation intestinal transplantation; MIS, maintenance, immunosuppression; PTLD, posttransplant lymphoproliferative disease; RRT, renal replacement therapy.
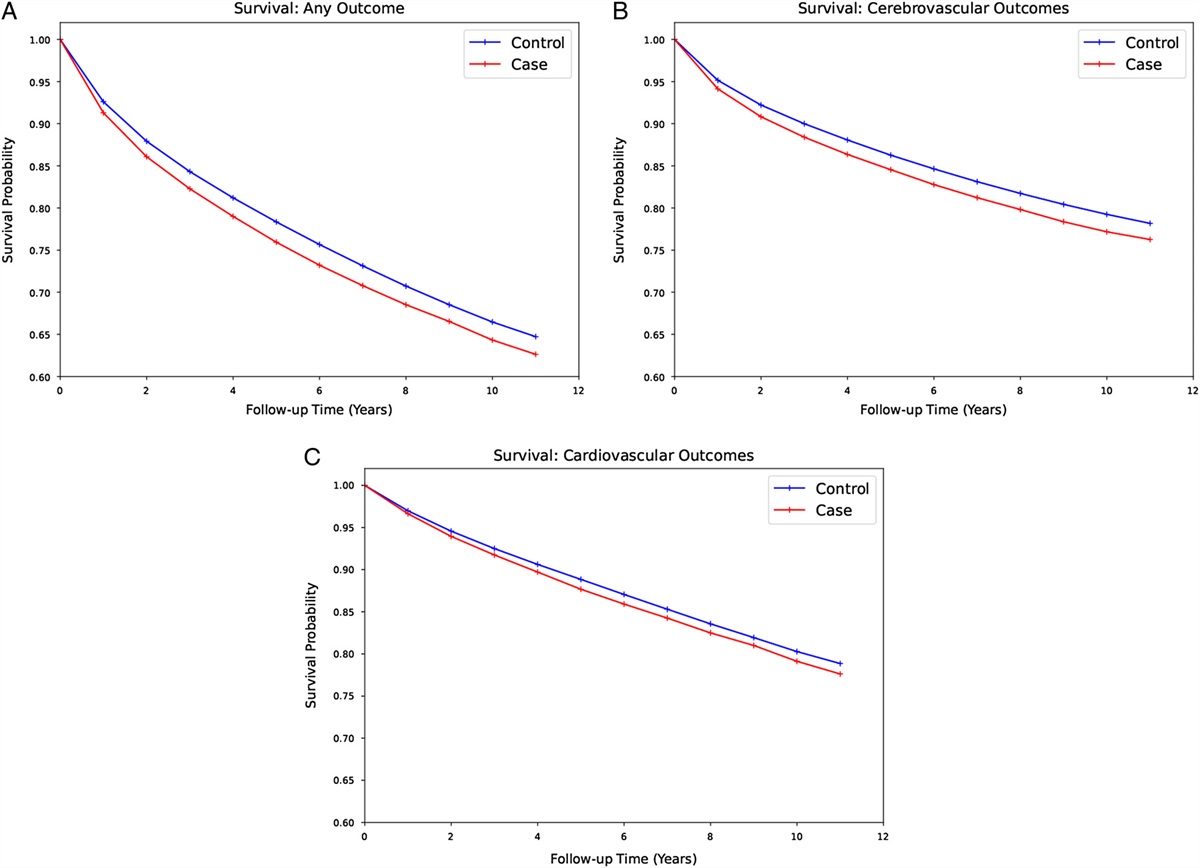
Primary outcome: Acute rejection rate was similar between both cohorts: 47% in LD-ITx versus 51% in DD-ITx (P=0.723). One-/5-/10-year patient survival for LD and DD were 74%/50%/46% versus 80%/48%/39%, respectively (P=0.826) (Fig. 1A).
 FIGURE 1:
FIGURE 1: Patient and graft survival of matched living and deceased intestinal transplantation cohorts (Kaplan-Meier). Patient survival (A). Graft survival (non-sensitized to death) (B).
Patient status at last follow-up was identical between LD and DD: patients alive with functioning graft 27% versus 30%; alive with graft removed 19% versus 18%; and dead/lost to follow-up 54% versus 53%, respectively (P=0.920). No difference in graft function was observed (full function accounting for 70% in LD-ITx versus 54% in DD-ITx; P=0.127). Graft rejection was the first cause of graft removal in both groups (72% in LD versus 88% in DD; P=0.082). One-/5-/10-year graft survival was 60%/41%/33% for LD versus 69%/36%/26% for DD (P=0.956) (Fig. 1B). RRT was similar between both cohorts (8% LD vs. 5% DD; P=0.621) as well as creatinine level (0.88mg/dl LD vs. 1.1 mg/dl DD; P=0.768). No difference was shown regarding PTLD and infection.
DISCUSSIONIn this ITR propensity-matched analysis, 63 LD-ITx were compared with 186 DD-ITx. Outcomes were similar for acute rejection, graft function, 1-/5-/10-year patient, and graft survival. This global experience suggests that LD is a valuable alternative (however not superior) to DD-ITx.
In 1964, one year after the first liver transplantation (Starzl, Pittsburgh, PA), Deterling transplanted at Boston Floating Hospital (USA) an ileal segment from a mother to a child who suffered from mesenteric thrombosis.10,11 This case was the first transplanted extrarenal LD organ.8 The child died early posttransplant.8,12,13 Another case of LD-ITx was done by Fortner (New York, USA) in 1970 between 2 sisters. The recipient was the longest survivor (79 days) after ITx in the pre-cyclosporine era.13,14 In 1988, Deltz (Kiel, Germany) reported on a 42-year-old female with mesenteric thrombosis who received an intestinal graft from her identical sister. She became PN-free and survived 5years.15
The technique of LD was standardized in 1997.6 After preoperative evaluation of the vascular pedicle,7,16 60 cm (<2 y) up to 180 to 200 cm (adults) of ileum is procured. The last 30 to 40 cm of ileum and ileocecal valve are left intact to maintain vitamin-B12 and bile salts resorption,7 avoid diarrhea, and bacterial overgrowth. Ileum is preferred over the jejunum for vascular anatomic reasons and for its adaptative capacity.17–21
In the recipient, the ileal graft artery and vein are anastomosed end-to-side to the aorta and caval vein, and intestinal continuity is restored under the protection of an ileostomy.8 Several single-center reports and even combined segmental liver and bowel LD were described.22,23 The ITR included 7 cases (1 before 1997) in which a colon segment was co-transplanted, which is not recommended given the importance of preserving the donor´s ileocecal valve.
Data on LD-ITx outcomes remain scarce, apart from 11 LD-ITx reported by Benedetti24 and recently 40 by Wu.25 The latter included 15 children and 25 adults (6 identical twins LD-ITx). This series (not captured by ITR) reports a 1-/5-year patient and graft survival of 80%/66.7% and 72.4%/60%, which compares favorably to the ITR data.25 The largest single-center analysis on DD-ITx, including 500 ITx/MvTx in 453 patients (1990-2008), reported 1-/5-/10-year survival of 85%/61%/42%.26 In the long-term, these data seem comparable to the ITR survival.
All ITR LDs were adults. The relationship between LD and recipients is not captured, but it will be in the future. The main indication for LD-ITx was SBS with life-threatening PN complications, similar to the DD cohort. The registry included 5 pediatric cLi-ITx with severe intestinal and liver failure in urgent need of transplant.8,23,27 Pediatric LD-ITx were more frequently in-hospital at the time of transplant and had a longer posttransplant hospital stay, suggesting that they were sicker compared with adults. No difference in rejection or patient/graft survival was observed between pediatrics and adults. Interestingly, no difference in outcome was seen between different volume centers. Most probably, centers with limited LD-ITx have well-established DD-ITx programs.
LD has intrinsic benefits that could lead to a better outcome. An LD graft is of excellent quality and does not suffer from additional trauma associated with brain death. Like for all LD-transplant procedures, the cold ischemia time (not captured by ITR) can be very short.24 Another advantage of an elective LD-ITx is that the recipient may receive immunosuppression or desensitization protocols pretransplant.28 Graft-recipient size-matching data were missing, but it can be anticipated that LD-ITx in adults will result in a better size-match since only one-third of the small bowel is transplanted, probably causing less difficulties to close the abdominal wall.23,29,30 In the case of LD-ITx, it is possible to enlarge the abdominal domain of the recipient pretransplant (eg, tissue expanders).31 Despite these theoretical benefits, our propensity-score analysis did not reveal a superior outcome (regarding rejection, graft function, graft, and patient survival).
The fact that HLA-matching would improve outcome was not supported by our analysis. Despite a better HLA-matching, the rejection rate was 47% in the LD cohort, and remained the leading cause of graft removal. However, Wu et al observed no acute or chronic rejection in 6 LD-ITx with fully HLA-matched donors. Therefore, it can be argued that LD should strongly be considered when a full HLA-matched donor is available, even pre-emptively.25 Of note, 15 cases of successful LD-ITx between HLA-identical donor/recipient pairs have been reported (see Table, Supplemental Digital Content 3, https://links.lww.com/SLA/E781 overview reported HLA-identical LD-ITx).13,14,21,24,25,32–37
Our data may suggest the utilization of LD-ITx in more ill patients, given their increased hospitalized status. It may represent the best option for infants who need a liver and intestine and may succumb before finding a size-matched DD. In clinical scenarios of immunodeficiency, bone marrow transplant and LD-ITx from the same donor may result in sustained graft tolerance.
Finally, LD may represent the only option for IF patients with no/limited access to DD-ITx. This probably explains the proportion of Asian LD-ITx, where DD is generally less supported for cultural/religious reasons.8,30,38
The ITx field has tremendously changed with the widespread use of autologous reconstruction resulting in better long-term survival.39 The introduction of GLP-2 analogues have significantly improved intestinal rehabilitation and will further increase the number of patients who can be weaned-off PN and avoid transplantation.40 However, both strategies offer no solution for patients suffering from life-threatening PN complications that have always been the indication of ITx with its inherent risks of alloimmunity and long-term immunosuppression.
This study does not address donor safety since only limited ITR data are available. However, based on the reported series, the overall risk of intestinal donation (segmental bowel resection) is limited and probably lower than that for kidney/liver donation. No simultaneous living kidney and intestinal donation was reported, probably by concern for donor safety.41,42 There have been no reported deaths or major complications.43–48 Wu et al reported in 40 donors 1 intraoperative bleeding, 1 small bowel obstruction (conservatively treated), and 1 incisional hernia.48 Donor´s weight decreased during the first months postoperatively, but was restored at 1 year. The most prevalent discomfort was an increase in bowel movements in 2 donors (5%) who were occasionally on antidiarrhea medication after 1year. Vitamin-B12 was reduced until 3 years postdonation without clinical repercussion, and in some donors, a better metabolic profile was observed, confirming the experience of 25 LD-ITx published by Ghafari et al47 and our own observation (Leuven). These results tend to confirm the safety of LD-ITx for the donor in the short term and long term.
This study – the first propensity-matched analysis on LDITx – has limitations inherent to its retrospective nature. Although the propensity
Comments (0)