
Remember me
This was a retrospective, observational study of treatment patterns and outcomes in hospitalized patients with primary IS or TIA without AF. Data were obtained from the CPRD linked with Hospital Episode Statistics (HES) Admitted Patient Care (APC) and Office for National Statistics (ONS) mortality data. The CPRD is a primary care database that includes longitudinal data from general practices and comprises a patient population that is generally considered representative of the UK population.
ParticipantsThe index date for each patient was defined as the date of the first hospitalization for IS or TIA, occurring between January 1, 2012 and March 31, 2019 (the index identification period). The patients were required to have a 12-month baseline period before the index date (baseline period). Adult patients (aged ≥ 18 years) with one or more primary diagnosis of IS or TIA in the inpatient setting during the index period were included. Patients were excluded if they had a diagnosis of AF at any time from the baseline period until 30 days following discharge or a diagnosis of IS during the baseline period (defined as the 12 months prior to the index date). Patients with any diagnosis of hemorrhagic stroke or traumatic hemorrhage at or prior to their index date or with a prescription for an oral anticoagulant at any time during the baseline period or within 90 days post-discharge were also excluded. Patients who died during hospitalization and those with zero follow-up days were also excluded. Patients were further categorized as treated and untreated. For the treated patients, the index treatment was defined as the first antiplatelet prescription for SSP in CPRD post-index date and within 90 days post-discharge. Clinical outcomes were measured following discharge for both cohorts.
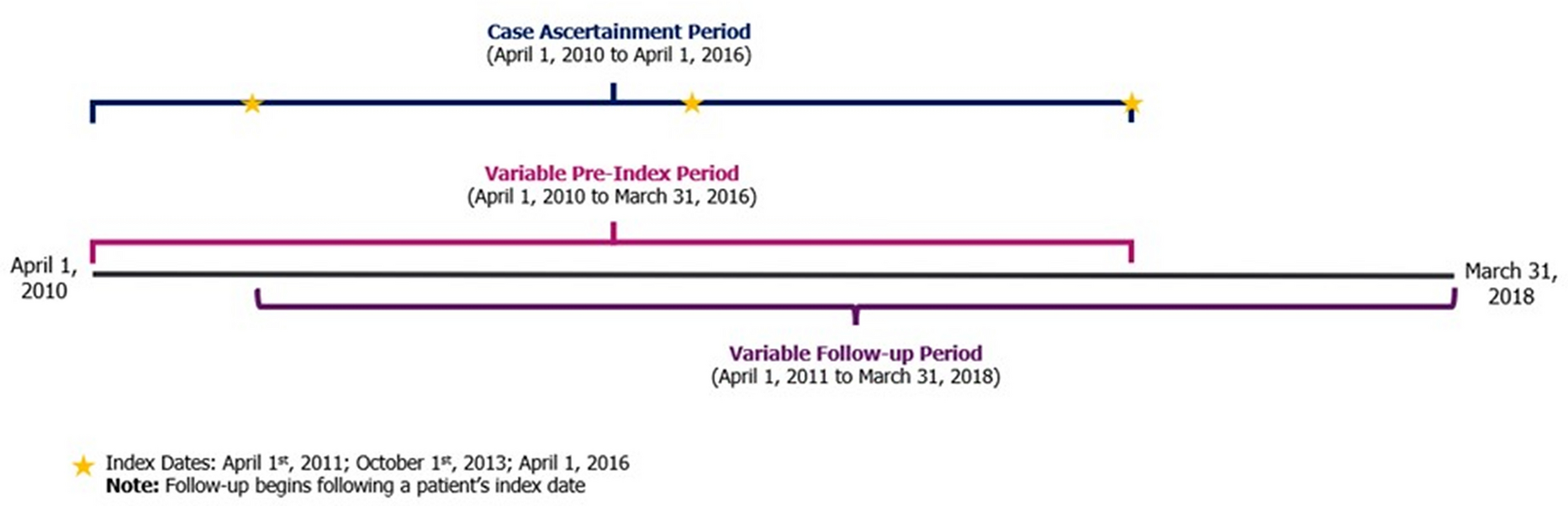
Data CollectionThe study was conducted on the data generated between January 1, 2011 and June 30, 2019 (Fig. 1). All patients were required to have ≥ 12 months of continuous CPRD and HES coverage prior to the index date (baseline period).
Fig. 1
Study design. IS ischemic stroke, TIA transient ischemic attack. aFirst hospitalization with principal diagnosis of IS or TIA between January 1, 2012 and March 31, 2019. bFirst antiplatelet treatment. cAny time from treatment index date until minimum of enrollment end, study end, discontinuation, or death
For the analysis of treatment patterns, patients were followed from the time of their index treatment to the earliest of end of enrollment, study completion, discontinuation, or death. For the analysis of treatment outcomes, patients were followed from day 1 post- discharge to the earliest of end of enrollment, study completion, death, or 30 days after treatment discontinuation. Treatment patterns and clinical outcomes were assessed at 3, 6, 12, 24, and 36 months post-discharge. For the untreated cohort, the follow-up is defined as day 1 post-discharge until earliest of end of enrollment, study completion, or death.
AssessmentsThe primary objective was to evaluate antiplatelet treatment patterns after the first hospitalization for IS or TIA. Evaluation of treatment patterns included the type of treatment (i.e., single antiplatelet therapy [SAPT], DAPT, and no treatment), duration, discontinuation, and switch. The secondary objective was to describe the post-treatment incidence rates of IS, myocardial infarction (MI), major bleeding (defined based on primary diagnosis of hospitalization records, cause of death, and transfusion records [for major bleeding only]), mortality (cardiovascular-related, all-cause), and major adverse cardiac event (MACE) 1 (IS, MI, or cardiovascular-related mortality) or MACE 2 (overall stroke, MI, or all-cause mortality).
Analyses were stratified according to treatment with clopidogrel SAPT, aspirin SAPT, clopidogrel + aspirin DAPT (patients who initiated the two antiplatelet agents on the same day), or no treatment. The stratification was determined by the index prescription record, if available. The no treatment cohort included patients with no antithrombotic prescription (i.e., no antiplatelet and/or no anticoagulant [apixaban, rivaroxaban, dabigatran, edoxaban, warfarin]) from their index date to 90 days post-discharge. Antiplatelet therapy was defined in the CPRD as aspirin, clopidogrel, dipyridamole, prasugrel, ticagrelor, or aspirin + dipyridamole (Aggrenox®).
Statistical AnalysesDescriptive statistics were applied across the study, including baseline characteristics, treatment patterns, and clinical outcomes. Baseline patient characteristics were summarized using frequencies and percentages for categorical values; means and standard deviations were used for continuous variables and to report treatment patterns. Clinical outcomes were reported in incidence rates. Only the first event of each type during the follow-up period was examined.
Ethical ApprovalThis article had been approved by the Independent Scientific Advisory Committee (ISAC), with the reference number ISAC19_240R. Although this study does not involve primary data collection from human participants, it was performed in accordance with the ethical principles set forth in the Helsinki Declaration of 1964 and its later amendments. Given that this study was based on retrospective analyses of secondary databases without enrollment of patients, all data were anonymized and de-identified prior to analysis.
Comments (0)