
Remember me


We aimed to evaluate the utility of combining Tinel’s test and CNT in the early stages of LN injury to predict whether the lesion would heal spontaneously or require surgical management.
ParticipantsThis study was performed in accordance with the Declaration of Helsinki and was approved by the Wakayama Medical University Institutional Review Board (approval number 1699). Observational data were collected from patients who visited the Wakayama Medical University Hospital with unilateral LN injury after third molar extraction between May 2014 and March 2020. The included patients had no remarkable medical history, except for the LN disorder. Written informed consent was obtained from all patients before they underwent examination. For each patient, CNT and Tinel’s test were performed at every consultation. Patients were diagnosed with severe LN disturbance based on the findings of at least two detailed examinations performed at intervals. The interval between the first examination and the second examination was at least 1 month. We advised to add more examinations after the second examination if it's convenient. It is difficult to specify the indications for surgical management, but surgical management was performed if any of the following two conditions were met:
1.If the follow-up period after tooth extraction was less than 6 months, and no improvement, worsening of the condition, or allodynia were observed.
2.If 1 year had passed since the tooth extraction and the patient condition was poor or if the patient had allodynia.
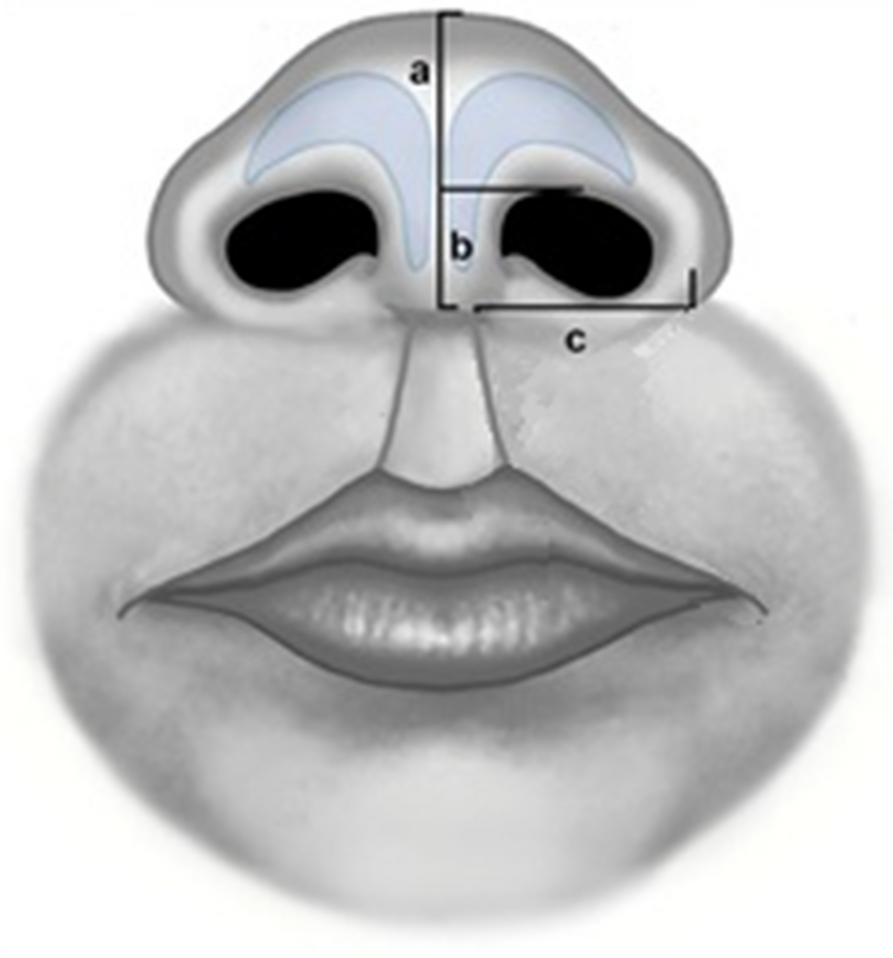
Diagnostic methods and criteriaTinel’s test involved palpation of the lingual gingiva at the extraction wound site. The earliest timing to apply the Tinel’s test is when the extracted wound has been cured after sutures removal. It is important to palpate the lesion around the lingual gingiva adjacent to the mandibular third molar extraction socket with fingertips gently and without strong pressure in all directions as indicated by the arrows in Fig. 1. In the case of positive reaction, a tingling pain can often be observed running from the tongue tip to the tongue margin, the oral mucosa and the lingual gingiva from the molar to the premolar in the affected side. In rare cases, similar pain may occur in the affected lower submandibular lesion around submandibular gland. As a control, we should similarly palpate the lingual gingiva of the unaffected contralateral mandibular third molar to remind the patient that no pain occurs on the unaffected side. This maneuver helps to elicit a distal referred tingling or hyperpathia on the side of the tongue in the region of the injury (scores: 0, no sensation was recognized; 1, some pain recognized at the target tongue region). The other hand, CNT involves a three-stage inspection method as shown in Fig. 2. The second and third levels of the CNT test are performed depending on the response to the previous level. Flow chart of CNT presented in this study suggests the rational approach of first investigating the response of the thicker nerves and later examining the response of the thinner nerves. Practically, it is often observed that the functional recovery of the nerve fibers is initiated at the thicker nerve fibers and gradually progresses to the thinner fibers. Further, CNT can be easily performed at the bedside without requiring extensive equipment. Specific evaluation criteria for each level of CNT are described below.
Fig. 1
Manipulation of Tinel test
Fig. 2
Flow diagram of Clinical neurosensory testing
Level AStatic two-point discrimination (2PD): before gentle contact with caliper tips is made on the lingual mucosae, the patient is asked to indicate when contact is felt and to identify whether that contact is of one or two points, which was then expressed in millimeters. Brush stroke directional sensation with a camel hair brush (brush) was examined by applying horizontal, vertical, and rotational stimulating movements on the lingual gingiva at the extraction wound site (scores: 0, no sensation was recognized; 1, sensations were recognized in only one direction; 2, sensations were recognized in two directions; 3, sensations were recognized during all movements).
Level BPressure pain threshold was examined using Semmens-Weinstein monofilaments (SWM) of 20 different diameters, with “1” referring to the smallest-diameter monofilament and “20” to the largest-diameter monofilament.
Level CThe pin prick test involved pricking the lingual gingiva at the wound site with a sharp needle (scores: 0, no sensation was recognized; 1, only pressure was recognized; 2, intensive pain was recognized).
Statistical analysesThe Fisher’s exact probability test analysis was performed to identify correlations between changes in the Tinel test and CNT findings (2PD, brush, SWM, and pin prick). Two-sample Student’s t test was employed to determine the differences between the means of the variables measured within test groups. For all analyses, the statistical significance was set at P < 0.05. All data were statistically analyzed for significance using R version 4.2.1 (R foundation for Statistical Computing, Vienna, Austria).
Comments (0)