
Remember me








We report the protocol (Version updated 6/17/2022) in concordance with the 2013 SPIRIT guidelines [26] (Additional file 1).
Study designThis is an open label, two-arm, non-blinded, randomized controlled trial designed to test the superiority of streamlined peer tele-HCV compared to enhanced usual care (EUC) to achieve HCV cure (defined as SVR12) in PWUD in rural Oregon (clinicaltrials.gov NCT04798521). In-depth qualitative interviews are conducted with a sample of study participants to better assess their treatment experiences and attitudes. Peer and clinician focus groups are conducted to identify critical intervention components and lessons learned for external replication. The Oregon Health & Science University IRB (IRB00000471) reviewed and approved the study.
OutcomesThe primary outcome is sustained virologic response as measured by an undetectable HCV RNA at 12 weeks post treatment. Secondary outcomes include: (1) HCV treatment initiation, (2) HCV treatment completion, (3) engagement with harm reduction resources, (4) rates of substance use, and (5) engagement in addiction treatment resources. Treatment completion is defined by a filled final DAA prescription and self-reported adherence of > 90% of DAA pills taken. Treatment initiation is defined as the first DAA prescription filled and self-report of taking the first pill. Participants who do not start treatment within 6 months are considered to have failed treatment (i.e., have a detectable HCV RNA level). Additional exploratory endpoints include treatment satisfaction (adapted from the single-item Medication Satisfaction Questionnaire [27]) and adherence to phone visits, defined as within 5 days before or after scheduled appointment.
Qualitative interviews are conducted by telephone with a sample of study participants to assess participants’ experiences with the telemedicine-HCV treatment intervention, including satisfaction with care, barriers to treatment initiation and adherence, and the role of peers in facilitating laboratory and telemedicine appointments, medication access, and adherence. A virtual focus group with peers assesses tele-HCV treatment barriers and facilitators, peer specialist activities, and advantages and disadvantages of tele-HCV. A virtual focus group with tele-HCV clinicians assesses peer-facilitated tele-HCV procedures; experiences engaging with specialty pharmacies, payers, peers, and patients; and clinical considerations.
Setting and participantsThis study takes place in rural communities in Oregon. The high prevalence of HCV in Oregon, significant percentage of the total population living in rural areas, and lack of specialist services outside of the Portland metro area make it an attractive location for the intervention [6]. All of the study’s peer specialists are certified by the state of Oregon, which includes completion of a week-long state-approved training program and biannual re-training and recertification. The study’s peers are also invited to participate in a monthly learning collaborative for peers statewide doing similar work (e.g. harm reduction and recovery support and linkage to hepatitis C testing and treatment) and an annual peer conference. Study peers participate in weekly full team meetings to talk through participant status and next steps, and the investigators conduct regular site visits to review documentation and observe and discuss procedures.
Peer support specialists and research assistants recruit PWUD who live in rural Oregon counties with high rates of overdose and hepatitis C infection to participate in this study. Rural counties with local syringe service programs (SSPs) providing both peer support specialist services and HIV/HCV screening are included as study sites: Douglas, Lane, Josephine, Coos, Curry, and Umatilla counties. Community-based SSPs serve as initial recruitment sites and are supplemented with community settings (e.g., parks, homeless shelters, community events). Participants are eligible for inclusion if they: live in the study area, have injected drugs, or used recreational opioids without injection in the last 90 days, are 18 years of age or older, have a positive HCV RNA, are enrolled in health insurance, and are interested in treatment. Participants are excluded if they have decompensated cirrhosis, defined as Child–Turcotte–Pugh (CTP [28]) score of 7 or greater (CTP B or C cirrhosis), or are pregnant or breastfeeding.
Participants are recruited through local SSPs, direct community outreach (e.g., parks, homeless shelters), and participant referral (respondent driven sampling). Research staff and peer coordinators encourage participants to use their personal networks to invite individuals for initial screening and participation. Participants receive cash incentives totaling $215 for survey completion and other study activities, including baseline and follow up surveys, blood draws, and treatment initiation visits.
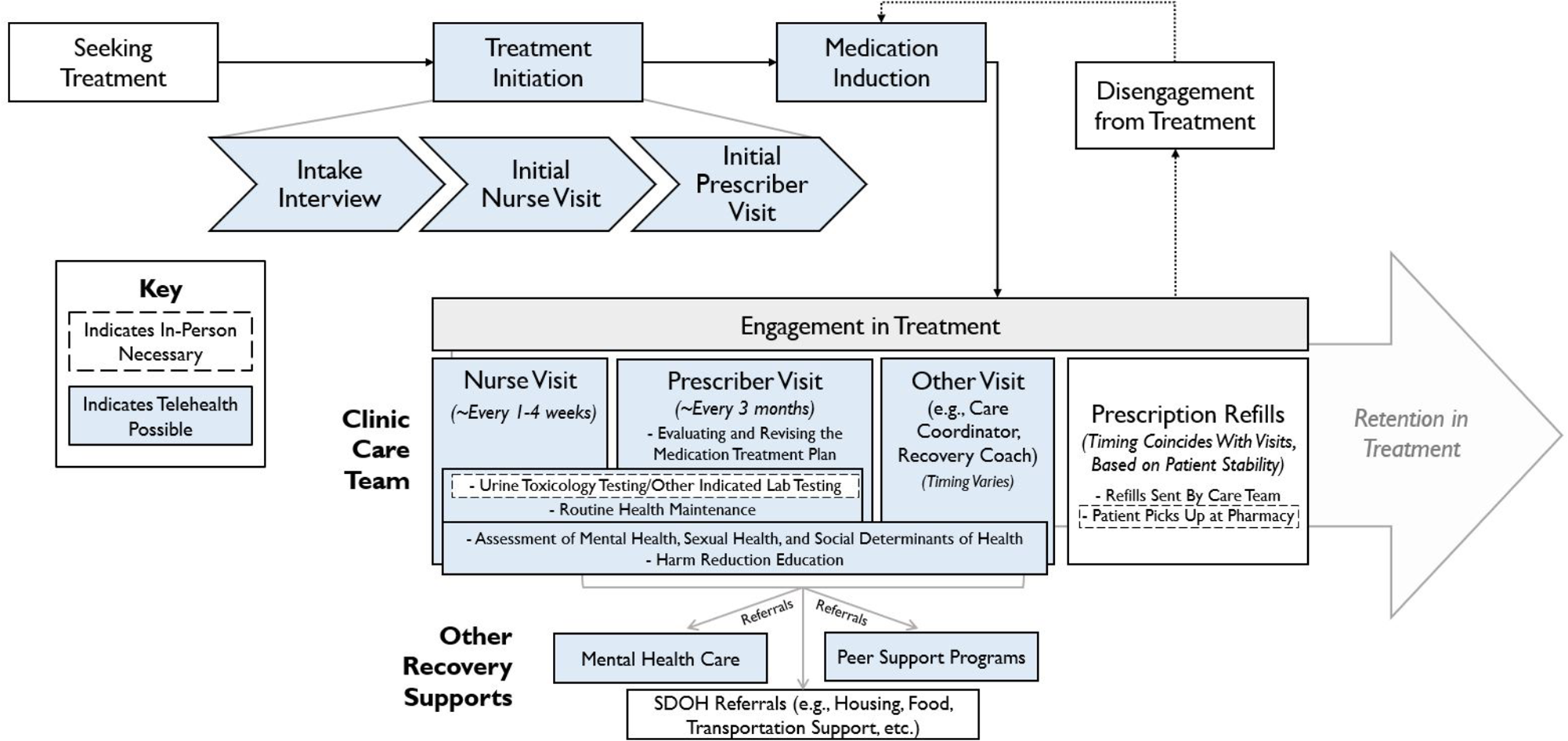
Procedures and follow-upFigures 1 and 2 depict participant procedures and study timeline. Pre-screening for eligibility includes a rapid HCV antibody test by local study staff or self-report from the participant of current HCV in addition to meeting other inclusion criteria. An Information Sheet Consent Form establishes consent for HCV rapid antibody testing during pre-screening. The OraSure® HCV Rapid Antibody test is a finger prick that can either be administered by study staff or self-administered, depending on participant or staff preference. Prior to the rapid HCV test, participants complete a full written consent form (see Additional file 2).
Fig. 1
Screening and randomization
Fig. 2
If the pre-screening HCV rapid test or self-report of chronic active hepatitis C is positive and they meet other inclusion criteria, peers complete the “Lab Form Determination” form to determine which standing order form is required (see Additional file 2: Table S1). Peers then accompany them to a local lab for confirmatory HCV RNA and additional baseline pretreatment evaluation by standing order (Table 1) to confirm eligibility. Peer support specialists can provide transportation and assist the participant in enrolling in health insurance at this time if necessary. The evaluation protocol streamlines lab testing and minimizes imaging assessments for cirrhosis to decrease barriers to treatment initiation and evaluation costs, in keeping with calls for simplified treatment evaluations [25]. Study investigators created standing lab orders for treatment naïve, treatment experienced, and women under 50, that allow for a single blood draw to assess appropriateness for DAA treatment. HCV genotypes are not routinely performed, unless the participant has a history of past DAA treatment failure. Women under the age of 50 are also screened for pregnancy. Rather than conduct imaging to assess for cirrhosis, participants with platelet counts of less than 150,000 per mcL or laboratory-based CTP score of 6 undergo a study clinician evaluation (see Additional file 2: Table S2) over the telephone exploring the likelihood of decompensated cirrhosis to determine eligibility for randomization. Participants who, in the opinion of the study clinician, have symptoms of decompensated cirrhosis, are referred for local ultrasound. All other participants are confirmed to be eligible for randomization without additional testing. Once eligibility is confirmed, all participants complete a baseline survey (Table 2) that includes questions regarding medical care history, barriers to treatment, engagement with harm reduction and substance use treatment, current substance use, perceived stigma of drug use, and HCV treatment history. Surveys assess use of non-prescribed prescription opioids, illicit opioids including fentanyl, methamphetamines, and other illicit substances, as well as the route of administration. Similar survey questions are asked at week 4 of treatment, end of treatment, at 12 weeks post treatment, and at 36 weeks post treatment. Follow-up surveys also ask about medication initiation, adherence, and changes in substance use and addiction treatment.
Table 1 Laboratory and other participant assessments collectedTable 2 Baseline surveys and sample questionsStudy data are collected and managed using REDCap electronic data capture tools hosted at OHSU [29, 30]. REDCap (Research Electronic Data Capture) is a secure, web-based software platform designed to support data capture for research studies, providing (1) an intuitive interface for validated data capture; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for data integration and interoperability with external sources. Following completion of consent and baseline assessments, participants are randomized by study staff and allocated to a study arm using a centralized random number assignment assigned through REDCap. Prescreen, baseline and follow-up surveys collected in the field or via phone are first documented on paper forms. These are then entered into REDCap by the research assistant. The source documents are kept in a locked file cabinet in a secure location. Access to de-identified data in REDcap are limited to IRB-approved study staff that interact with participants. Participants who indicate willingness to be contacted for future studies in the consent form may be contacted and offered participation in future studies. Records are routinely audited by the investigator, with the support of the National drug abuse Treatment Clinical Trials Network (CTN) Western States Node data monitoring resources.
Throughout the study, peers offer harm reduction supplies (sterile syringes and works, fentanyl test strips, and naloxone overdose rescue kits) and substance use disorder treatment linkage to participants in both study arms.
Intervention: tele-HCV armParticipants randomized to the peer tele-HCV treatment intervention arm are scheduled for telemedicine visit and HCV assessment by a study clinician (physician, nurse practitioner, or clinical pharmacist) as soon as possible following randomization, with the goal of same-day appointments. For most participants, this is also the treatment initiation visit. The peer facilitates telemedicine visits using the chosen web platform of the participant. Telemedicine visits are conducted in a private location where the participant is comfortable. This could include the SSP office where the peers work, but can also occur at any location with adequate cellular-based internet (e.g., a park, car, or the participant’s home). Peer support specialists carry a tablet with internet connectivity to access the telemedicine visit if the participant does not have their own access. If additional tests are necessary for clinical decision making, peers assist participants in navigating health system barriers and arrange a second appointment with the telemedicine HCV treatment provider.
The telemedicine study clinician performs a standard of care hepatitis C treatment initiation history and evaluation and submits a prescription for an appropriate pangenotypic DAA treatment regimen (glecaprevir + pibrentasvir or sofosbuvir + velpatasvir per Oregon Health Authority prior authorization criteria) based on comorbidities, side effects, patient preference and insurance coverage. The study pharmacist assesses barriers to adherence, reviews medications for drug-drug interactions, reviews side effects, and provides patient education. Prior authorizations are completed and submitted by the study pharmacist.
All participants initiating treatment are prescribed DAA treatment for 4 weeks at a time. Most participants require two separate dispensations at week 0 and week 4 for a total of 8 weeks of medications, with a small subset requiring a third, 4-week dispensation for a total of 12 weeks of therapy. Medications are mailed to a home address or to the SSP office to be stored in a secure locker until the participant picks up the medication. The study clinical pharmacist contacts the participant by telephone or telemedicine visit at week 0 and week 4 to (1) determine medication tolerance, (2) assess adherence and (3) dispense medications by mail or ensure medications received, depending on the participant’s insurance. If the pharmacist is unable to connect with the participant after 3 attempts, treatment will not be delayed, and the peer will continue to assist in receiving all refills. Peers assist participants in keeping telemedicine appointments and in navigating medication pick up or storage, if not mailed directly to the home. If problems or side effects arise during treatment, participants call the research assistant or peers, who connects them to a study clinician. The study clinician will evaluate for considerations for discontinuation of therapy (e.g., evidence of new decompensated cirrhosis) and advise participants on management of treatment interruptions consistent with current guidelines [31]. If there is a significant gap in therapy (≥ 21 days), SVR12 from last day on treatment is collected and included in primary care analysis. SVR12 rates for participants in both arms with partial treatment completion will also be reported separately in the results.
Peers facilitate repeat HCV lab testing at 12 weeks following the end of treatment and relay results to the participant in the SVR12 follow-up visit, along with completion of follow-up surveys. End of treatment date is defined as the day the participant last took a DAA medication, as determined in the 8 week follow up survey or earlier communication with research staff. Those successfully achieving SVR12 are counseled on ongoing harm reduction methods to avoid reinfection. Those with persistent HCV viremia at 12 weeks post-treatment are referred to telemedicine treatment providers for treatment re-initiation outside of the study. All participants are scheduled for a 36-week post end of treatment survey visit.
Control: enhanced usual careFollowing completion of full pretreatment evaluation and study inclusion, research staff refer participants randomized to the EUC arm to a local community health clinic with experience treating hepatitis C to engage in treatment. EUC patients are encouraged to engage with local primary care and health plan resources and receive an information sheet on optional clinics to attend. The information sheet includes a list of questions participants are encouraged to take with them to their visit. Research assistants outreach to participants regularly to determine if they have engaged in local health resources, schedule assessment visits, and request a bidirectional release of information. Research staff call the clinic or participant periodically to ask if the participant has initiated treatment. After 3 months of no treatment initiation, the participant begins survey and other outcome data collection as if the participant had started treatment at that time. Peers facilitate SVR12 laboratory testing at 12 weeks after actual or intended end of treatment by study convention, depending on whether treatment is initiated. Local HCV referral providers are encouraged to participate in the OHSU Hepatitis C Elimination Extension for Community Healthcare Outcomes (ECHO) program but are not study participants. The hepatitis C ECHO is an interactive education and capacity building model expanding HCV treatment expertise to rural communities [32].
In either arm, participants who do not initiate treatment by 12 weeks after randomization begin their assessment timeline, mirroring the treatment timeline for an 8-week direct-acting antiviral regimen. For these participants, the primary study outcome SVR12 is assessed at 32 weeks after randomization, corresponding with 12 weeks after completion of 8 weeks of treatment. If participants initiate therapy between 12 and 24 weeks post randomization, the follow up and SVR12 dates are regenerated. Participants who do not start treatment within 6 months of randomization will be considered treatment failures.
Comments (0)