
Remember me


The Japanese Society of Temporomandibular Joints first defined and recognized MMTAH in 2008. MMTAH is a relatively newly identified disease entity characterized by trismus due to contracture of the masticatory muscles, resulting from hyperplasia of tendons and aponeuroses [2, 3]. According to previous reports, MMTAH is highly prevalent among female patients over a wide range of ages.
In this case, the patient was examined at the Department of General Medicine for suspected polymyositis due to simultaneous lower limb pain and trismus.
Although rheumatoid arthritis and scleroderma, classic connective tissue diseases, rarely cause severely limited mouth opening [5], limited mouth opening has been reported in patients with polymyositis and dermatomyositis. However, these reported cases were due to muscle inflammation, which spread to the surrounding tissue. In addition, histological findings in these cases showed chronic inflammation, fibrosis, and disappearance of muscle fibers [6, 7]. In this case, muscle inflammation was not found on CT or MRI. In addition, the administration of serum anti-Jo-1 antibody in this patient did not support the diagnosis of polymyositis.
Crincoli et al. also reported that bruxism, which was similar to the habit of clenching in this case, was not reported in patients with idiopathic inflammatory myopathies, such as polymyositis and dermatomyositis. They concluded that this could be explained by a condition of muscle weakness caused by loss of muscle mass and impaired intrinsic contractility [8].
The histopathological findings of this case revealed hyperplasia of thick muscle cells with diameters of approximately 60 μm, while normal cells were in the range of 20–40 μm as previously reported by Tsuneki et al. [9]. Masseter muscle hypertrophy is a relatively rare and benign enlargement of the unilateral or bilateral masseter muscles [10]. However, the etiology of masseter muscle hypertrophy remains under discussion. This asymptomatic persistent muscle enlargement has been reported to be initiated by bruxism, clenching, or heavy gum chewing [11, 12]. Although Martensson also indicated the relationship between the deformity and the so-called work hypertrophy [13], some reports have doubted this theory [14,15,16]. Beckers reported in his case reports that seven of 17 patients (41.2%) exhibited signs that seemed to support the work hypertrophy theory, such as bruxism and occlusal imbalances [17].
Work hypertrophy caused by exertion results in muscle enlargement. An increase in muscle fiber diameter from 20 to 60 μm has been reported to be the cause of increased masseter size [11, 18].
In our case, immunohistochemical findings revealed that these muscle cells were positive for calcineurin A, which has been reported to be relevant to muscle hypertrophy due to overload.
Studies using bite-opening rats proposed that calcineurin signaling [19], a calcium/calmodulin-regulated protein phosphatase that acts on the transcription factors of the nuclear factor of activated T-cell family, was an important molecular mechanism inducing masseter muscle hypertrophy [20].
Therefore, there might be a possibility that the overload of muscles of the master and lower limbs during her office time caused a series of symptoms in this patient.
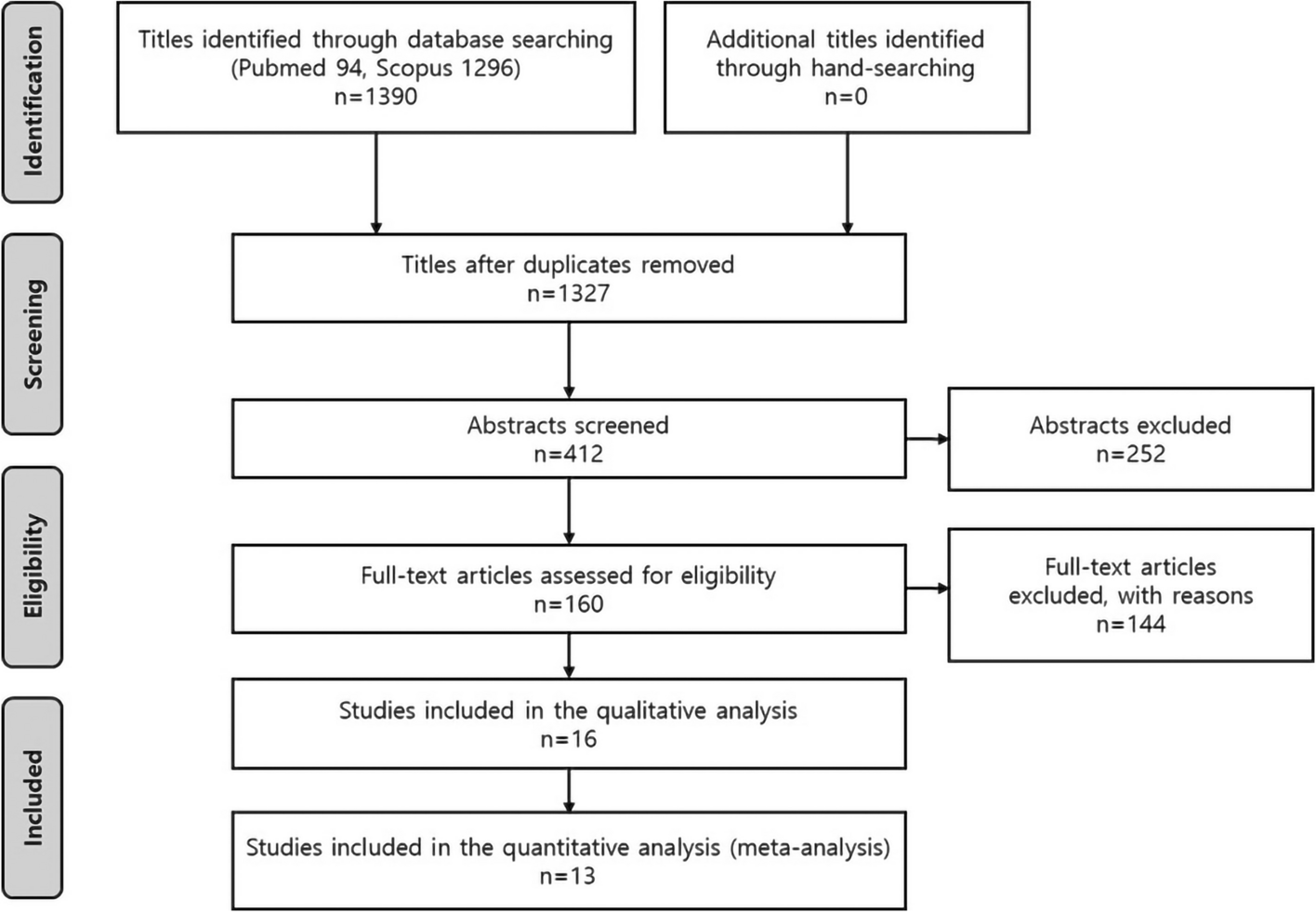
To the best of our knowledge, 47 cases, from 5 reports, have been diagnosed with MMTAH and reported in English-language journals since 2008 [3, 21,22,23,24].
Coronoidectomy or coronoidotomy to remove the temporalis muscle tendon was performed to treat MMTAH in all cases. Aponeurectomy and excision of the masseter muscle were performed to remove hyperplastic tissue. However, mandibular anglectomy was performed in only three cases, according to these reports. This seems to be the case because it is now chosen for esthetic reasons, particularly for square mandibles [25, 26].
Botulinum toxin type A, which is a powerful neurotoxin produced by the anaerobic organism Clostridium botulinum, is one of the other treatment procedures for masseter muscle hypertrophy (MMH). Injecting botulinum toxin type A into a muscle causes interference with the neurotransmitter mechanism, producing selective paralysis and subsequent atrophy of the muscle [27,28,29]. However, there have been no reports on the use of botulinum toxin type A for treatment of MMTAH.
The biggest limitation of botulinum toxin therapy is that the treatment effect wears away within 6 months and the original condition recurs. Unlike surgical excision of muscular tissue, which reduces the actual number of muscle cells, botulinum toxin type A only temporarily reduces muscle volume [29]. Therefore, patients must be informed of the recurrence rate after the procedure.
Postoperative mouth-opening rehabilitation is an important factor for good prognosis. Using MRI at 1 year after surgery, Sato et al. revealed that the temporal muscle reattached to the resected stump of the bone [30]. Many studies have reported that mouth-opening training was performed for 6–24 months after surgery for MMH and MMTAH.
In our case, because the patient visited our clinic constantly, the maximum mouth opening reached 48 mm 6 months and 44 mm 12 months after surgery using the mouth guard during her work time to remove negative factors, such as clenching, and obtain a more sufficient training effect (Figs. 7E and 8 A, B). Based on our review of previous reports, as far as we can summarize, the data from 24 cases of maximum mouth opening during the first year after surgery are shown including our case [3, 21,22,23,24]. Although the maximum mouth opening was reduced 1 month after surgery, it was thought to be due to an inflammatory reaction. However, the maximum mouth opening became stable 6 and 12 months after surgery (Fig. 9).
Fig. 9
Summary of the mouth opening after the surgery from the previous reports. Gray dots indicate the data from 24 cases of maximum mouth opening before and during surgery and 1, 6, and 12 months after surgery. The gray line shows the average of these cases. The black dots and lines show the maximum mouth opening in each period in our case
Comments (0)