
Remember me
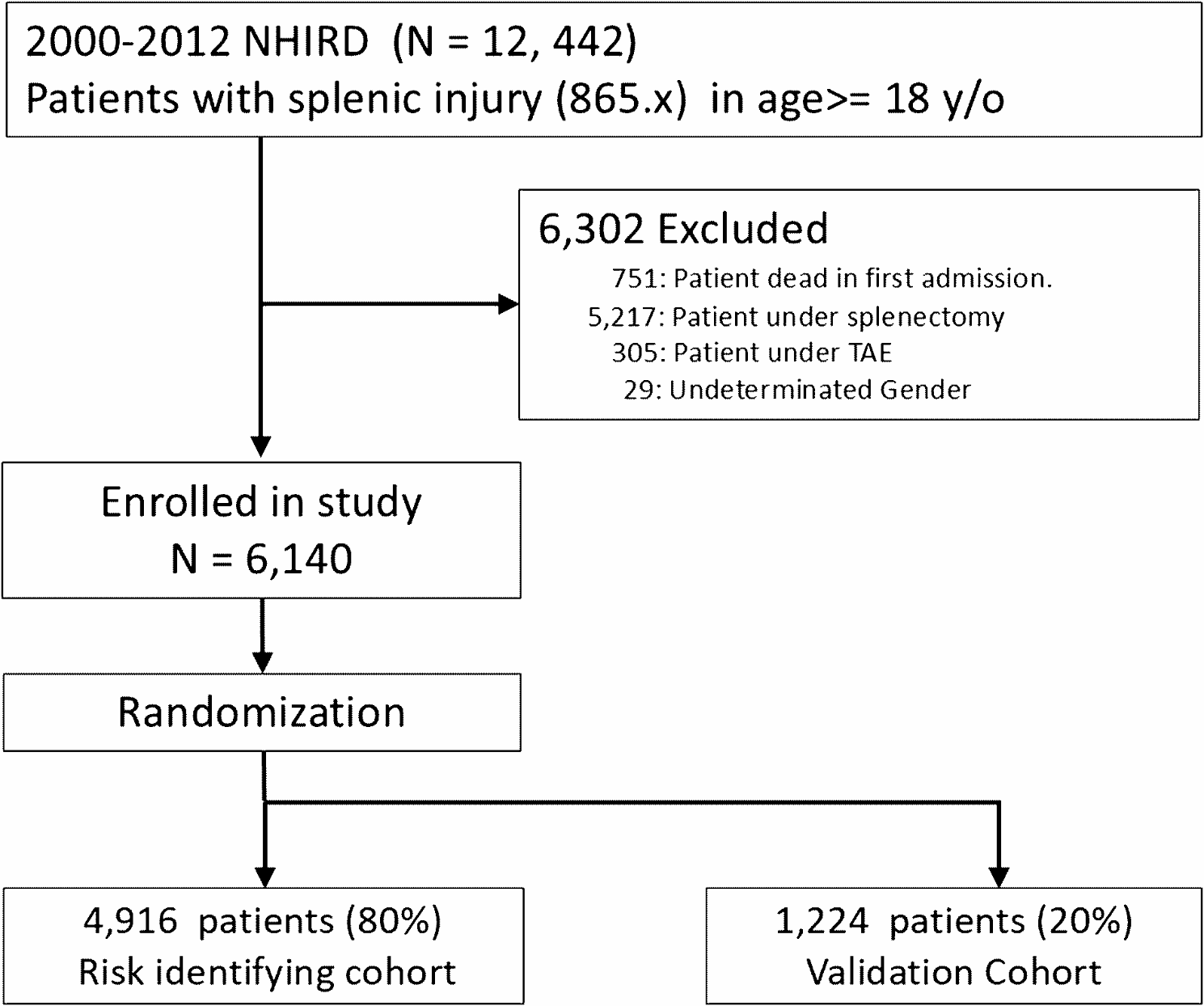
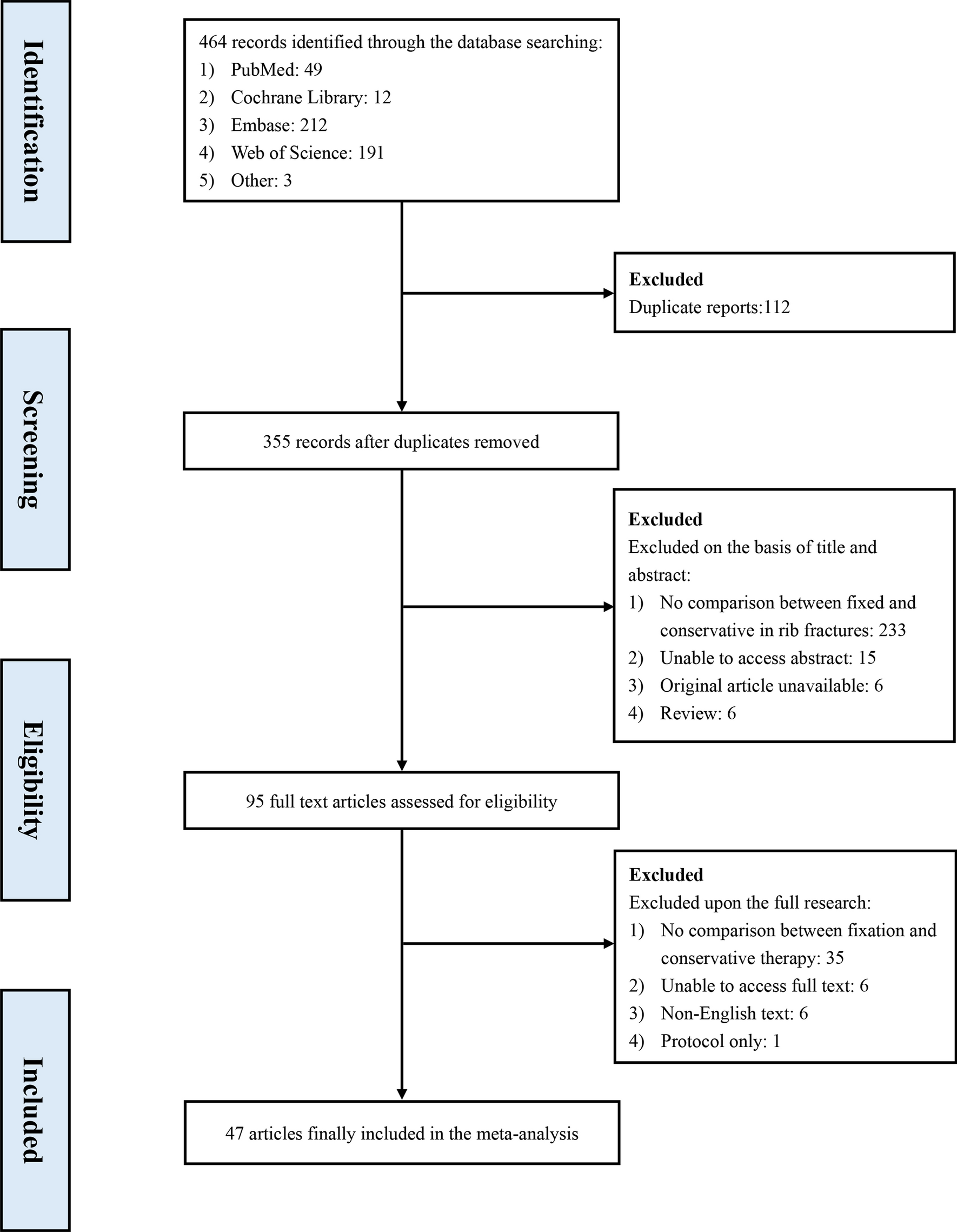







Electronic database searching found 564 records (titles and abstracts), of which 25 were eligible for inclusion in this SR. In the full-text review, three studies were excluded, leaving 22 articles for inclusion. After conducting a snowball scanning of the references cited in these 22 articles, five additional references were found. Therefore, twenty-seven articles were finally included in the SR [14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40]. Of these, four were comparative studies, of which three were evaluated as appropriate to combine in meta-analyses [19, 37, 40]. Figure 1 shows the PRISMA diagram for the selection of the studies.
Fig. 1 Characteristics of the included studies
Characteristics of the included studiesAs shown in Table 1, the 27 articles included in this SR were published between 1995 and 2022. Of these, eleven recruited participants are from the USA. Fifteen were from Europe: Italy (n = 4), France (n = 4), UK (n = 4), Spain (n = 2), and Germany (n = 1); the remaining study was from Canada. More than half (n = 15, 55%) of the articles were case reports, eight (30%) were case series, and four (15%) were comparative studies.
Table 1 Study level data (study characteristics and patients’ information)Additional file 1: Table S1 presents each study’s objectives. This information reveals that the studies were homogeneous regarding the populations and the aims for which TIPS were created. In all studies, TIPS was placed as a preoperative adjunct to achieve portal decompression under the assumption that portal pressure reduction would diminish the risk of intraoperative and postoperative complications.
Characteristics of participantsThe studies in this SR recruited 426 patients. Of these patients, 264 underwent perioperative TIPS creation. The remaining patients were controls without TIPS, of which 15 were reported in a case series of patients with refractory ascites and hernia requiring surgery. However, no comparisons were made between groups in this case series [38]. Of note, in two studies reporting data from 27 patients with TIPS, eight subjects (n = 8) underwent postoperative TIPS creation, immediately after surgery. Therefore, 256 patients underwent preoperative TIPS to achieve portal decompression in anticipation of surgery.
As shown in Table 1, most patients were near or at the age to be classified as “senior adults” (60 years and above) and had cirrhosis of different etiologies, of which alcohol-related cirrhosis was the most frequent.
Additional file 1: Table S2 overviews portal hypertension features (including HVPG) and LREs. Overall, patients had clinical signs of clinically significant portal hypertension by either documented endoscopic proof of esophageal varices or previous episodes of variceal bleeding (see Additional file 1: Table S2 for detailed data). Moreover, 23 studies reported a history of a previous LRE, reflecting a high burden of decompensated cirrhosis in the included studies.
As mentioned above, 256 patients underwent preoperative TIPS, but not all TIPS insertions were performed pre-emptively to surgery. Of these patients, 70% (n = 179) underwent preoperative TIPS placement in a bridge to surgery. In contrast, 77 underwent preoperative TIPS placement as a therapeutic tool for an LRE that was present/in progress when surgery was schedule/planned, most commonly ascites and/or variceal bleeding (Table 1). Information regarding the type of stent used for TIPS creation was available in 12 studies. The use of a non-covered (Wallstent®) and an expanded polytetrafluoroethylene (ePTFE)-covered stent (Viatorr®) were reported in 6 and 3 studies, respectively. The remaining three studies reported using both types of stents (either Wallstent® or Viatorr® stent). The proportion of patients using one or another stent type was not available.
The conditions requiring surgery and the surgical interventions performed are detailed in Table 1. Also, as shown in Fig. 2, there were abdominal, thoracic, gynecologic, and vascular/endovascular procedures performed with preoperative TIPS. Tumor resection surgery was the most common, followed by non-oncologic gastrointestinal procedures, including hernia repair. In addition, there were cases of aortic aneurysm repair (n = 2), aortic valve replacement (n = 3), and coronary artery bypass (n = 2).
Fig. 2
Types and percentages of surgical interventions performed
Risk of biasThe results of the methodological quality assessment of the studies included in this SR are available in the Additional file 1: Figs. S1 and S2.
Overall, the case series and comparative studies were at risk of selection bias due to their retrospective nature and biased evaluation of endpoints. However, most of them presented a clearly stated aim and defined appropriate endpoints to the study’s aims. Regarding the comparative studies included in the MA, the intervention and comparison groups were contemporary, and it was likely that the groups had baseline equivalence.
The more common methodological pitfalls found across studies were the absence of prospectively collected data and the issues associated with study endpoints’ definition and evaluation. Also, in four studies, it was unclear whether the follow-up period was appropriate for the captured and reported outcomes (see Additional file 1: Fig. S1).
Outcomes and meta-analysisSurgery attainment/execution after TIPS was reported in 231 (90%) out of the 256 patients that underwent preoperative TIPS. From the 231 surgical procedures performed with preoperative TIPS, 38 (16%) were classified as emergency surgeries.
Four studies had control group data. However, one study [15] included seven patients that underwent perioperative TIPS in the postoperative period. This study was not considered for MA. In the remaining three comparative studies, patients who underwent preoperative TIPS were compared to controls with cirrhosis who underwent surgery without TIPS. Relevant clinical and outcome data from these articles are available in Table 2.
Table 2 Data from comparative studies included in the meta-analysisRandom effects MA showed significantly lower odds of postoperative ascites if preoperative TIPS was created (2 studies: OR = 0.40, 95% CI 0.22–0.72; I2 = 0%) (Fig. 3). We acknowledge that the data combined for the MA of ascites came from studies that used propensity score matching techniques as the method for selecting controls.
Fig. 3
Forest plot for ascites (TIPS vs. non-TIPS)
In contrast, random effects MA (Fig. 4) found no significant differences in 90-day mortality (3 studies: OR = 0.76, 95% CI 0.33–1.77; I2 = 18.2%) (Fig. 4a), perioperative transfusion requirement (3 studies: OR = 0.89, 95% CI 0.28–2.84; I2 = 70.1%) (Fig. 4b), postoperative hepatic encephalopathy (2 studies: OR = 0.97, 95% CI 0.35–2.69; I2 = 0%) (Fig. 4c) and postoperative ACLF (3 studies: OR = 1.02, 95% CI 0.15–6.8, I2 = 78.9%) (Fig. 4d).
Fig. 4
Forest plots for the outcomes of interest: a 90-day mortality; b Perioperative transfusions; c Postoperative hepatic encephalopathy; d Postoperative ACLF
Comments (0)