
Remember me



This factor asks: ‘for what purpose(s) is a formulation being developed?’. This factor is modelled as a set of non-mutually exclusive purposes. Formulation is most commonly understood as serving an explanatory purpose, whereby hypothesised explanations of the presenting problem are constructed, allowing for the targeting of treatment strategies toward causal or maintenance factors (Eells, 2015, 2025). This purpose is commonly endorsed, with a function of informing treatment seen as an integral aspect of the formulation process by 85% of surveyed UK clinicians (Thrower et al. 2024a, b). However, the relative priority given to the explanatory function of a formulation appears to differ across approaches and clinicians. Alongside an explanatory function, some approaches emphasize a depathologizing function. Humanistic approaches for example, often seek to account for a person’s difficulties in references to adverse or abnormal circumstances. A further example of a depathologizing approach is the Power Threat Meaning Framework (Johnstone et al., 2018). This approach aims to tell a person’s story with emphasis on how power, threat, and meaning have shaped their experiences, thus normalising their difficulties as understandable responses. This depathologising function appears endorsed by clinicians in the aforementioned consensus study, with clinicians agreeing that the process of formulation should be normalising and destigmatizing for clients (Thrower et al. 2024a, b). In terms of other common functions, formulations can also serve prognostic (e.g., estimating reoffending risk in forensic settings or helping determine readiness to return to work or school after mental health leave), administrative (e.g., clarifying causal factors relevant to funding decisions or assessing capacity to stand trial), or communicative functions (e.g., summarising complex histories for clients, families, or other professionals). These examples are not exhaustive.
This factor is placed first as purposes for formulating typically constrain other decisions/factors that follow. Intended functions will likely influence what is targeted, what is focused on as explanatory content, level of detail, and what form the formulation it takes. For example, if seeking to depathologize then an etiological explanation emphasising preconditions and precipitating factors outside of the individual’s control seems fit for purpose. If, however, one has limited assessment time and is trying to make efficient and targeted treatment suggestions, then focusing more on perpetuating factors that are under volitional control would be more appropriate. Protective factors seem relevant in both cases, but especially under a prognostic function.
CollaborationThis factor asks: ‘how involved is the client in the process of formulation?’. It is modelled as a continuum. Extremely collaborative, co-constructed or client-led positions (e.g., Rogerian therapy), minimise the role of therapist-as-expert, focus on joint observations and inferences, or simply facilitate the client to construct and reflect on their own understandings/formulations. Moderately collaborative approaches meanwhile, denote those that value the knowledge and skills of both the clinician and the patient, often collaborating on therapeutic ideas introduced by the therapist (e.g., CBT, Johnstone, 2018). Such approaches are reflected in well-known statements such as ‘the client is the expert in their experience, while the clinician brings scientific and professional expertise’. The didactic end of this spectrum represents approaches where formulation is understood as something developed by the professional about the client. Related to but not captured by this dimension (nor the wider taxonomy) is the idea of team-based formulations involving inter-professional collaboration (Cole et al., 2017).
Some may be surprised by the idea of a didactic formulation. 86% of respondents in the aforementioned consensus study agreed that formulations should be developed collaboratively. Interestingly though, the statement ‘It is important for the formulation to be explicitly shared with the individual’ did not reach consensus (Thrower et al. 2024a, b). The degree of collaboration imagined in agreeing to such a statement thus appears to vary. While collaboration clearly represents an ideal given the principle of autonomy, what degree of involvement a client can have in a formulation is clearly dependent on their current capacity (e.g., age, reflective capacity, impaired state). Clinicians often, explicitly or implicitly, make sense of a client’s difficulties without intentional and/or fully informed input from them. Certain approaches and styles may also simply be more didactive in nature. Examples of a didactic approach might include: psychoanalytic interpretations, formulating as a consultant, formulating risk when the client is not contactable, formulating when clients are impaired or of insufficient capacity. All of these situations involve reasonable but non-collaborative case formulation. Collaboration then, while a valid ideal, is neither always beneficial nor realistic, and clearly varies. Ultimately, how collaboratively one formulates should be a matter of clinical reasoning.
Specificity of the Target/sThis factor considers: ‘how general or specific should the target/s of a formulation be?’. Modelled as a continuum of generality to specificity, this factor captures what are considered suitable targets of a formulation, focusing on how precisely they are detected and represented in the formulation process. At the extremely general end formulations may try to encapsulate a client’s entire life story (e.g., why has X’s life taken the direction it has? ). Slightly more specified are formulations targeting ‘the presented problem’, referral questions, or a particular diagnosis (e.g., why is X depressed?, why does X struggle with emotion regulation? ). Continuing to move in a more specific direction, formulations can be targeted at clinical phenomena, identified as stable and clinically relevant features in the assessment information (e.g., frequent self-critical thoughts, anticipatory anhedonia). At an extreme of specificity, sit attempts to explain one-off behaviours, experiences, or data points (e.g., why did X cry on the way to the session, why did X score highly on a particular measure?). Each of these approaches may make sense in certain contexts and consistent with certain purposes, however, assuming an explanatory function the approach of targeting clinical phenomena is preferable. Such an approach encourages precise explanations while forestalling the risk of getting distracted by noise in available information (Bogen & Woodward, 1988; Ward et al., 1999, 2016).
Domains of RelevanceThis factor asks: ‘what domains are considered relevant to serve as explanatory elements in a formulation?’. This factor is modelled as a set of domains from which several may be seen as relevant to varying degrees. These include but are not limited to psychological, social, biological, spiritual, cultural, historical, economic, and environmental. This list is broad to maintain applicability across ontological and cultural perspectives. Ideally, domains of relevance should be informed by consideration of scientific knowledge about the problem, as well as clinical experience and knowledge of the client attained through assessment. That is, domains considered relevant should change depending on the client and problem at hand.
In practice however, approaches to formulation appear to vary for a range of different reasons including theoretical orientation and clinical habit. For example, classical CBT and psychodynamic approaches emphasise internal psychological explanatia, while family-systems approaches prioritise relational dynamics. Incorporating sociocultural factors is endorsed by clinicians, as is consideration of biological factors such as effects of medication and potential organic causes (Thrower et al. 2024a, b). It is unclear however, how consistently such factors are actually considered in practice. Considering cultural factors, especially for minority groups, is considered vital for improving treatment outcomes (Faheem, 2023). The Meihana Model for example, developed specifically to support assessment of Māori clients, prescribes consideration of factors often not included in other approaches – e.g., spiritual, intergenerational, socio-historical (Pitama et al., 2007).
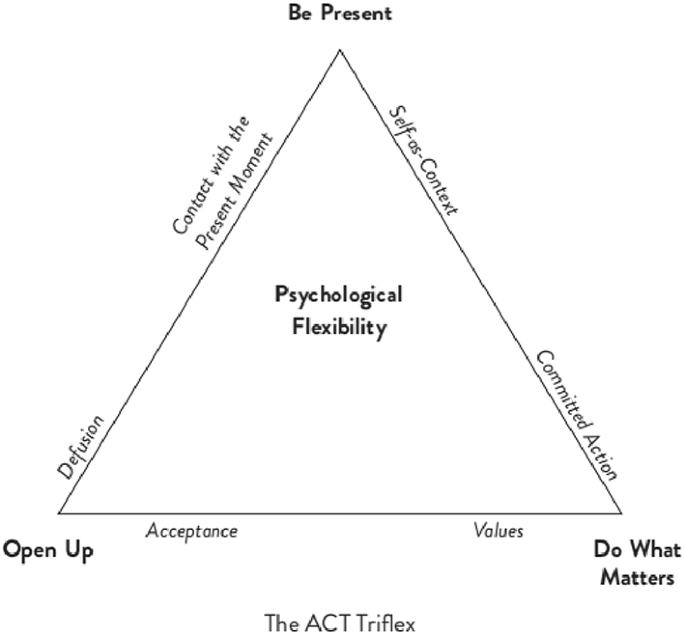
Loyalty to ModalityThis factor asks: ‘to what degree is formulation understood as being contained within a particular modality of practice (e.g., CBT, Psychodynamic, DBT, etc.)?’. A strictly loyal understanding would see formulation as being contained within a particular modality. This position strongly scaffolds formulation, providing the clinician with set tools and concepts to draw on – e.g., an ACT practitioner formulating based solely on ACT concepts such as lack of presentism and a lack of clarity around values. At the other far end of this continuum lie trans-modal approaches to formulation. Under such a view, formulation is understood as a process that stands completely independent from treatment modality (Eells, 2015). The Abductive Theory of Method (ATOM), for example, describes formulation as a logical process of enquiry and inference independent from modality or extant theory (Ward et al., 1999, 2016). Concepts from treatment modalities or explanatory theories can be utilised as content within this approach but are not given a priori privilege due to clinician modality. Instead, their inclusion/exclusion from the formulation is constrained at the level of explanatory process by evaluation of their explanatory value. Somewhere in the middle of this continuum sit eclectic approaches – i.e., those that draw on multiple frames/modalities without a clear method or set of guiding principles (e.g., someone blending elements of CBT, psychodynamic, and emotion-focused therapy). These eclectic approaches are placed here because, without such a method or set of guiding principles, formulation does not emerge as an identifiable and independent process as it does with trans-modal approaches.
Loyalty to (vs. independence from) treatment modality when formulating is not something well discussed elsewhere. This idea is useful as it allows for more precise discussion about the relationship between formulation and treatment approach. In the aforementioned consensus study, for example, no consensus (52% agreement) was reached on whether formulation should ‘stick to a model’ (Thrower et al. 2024a, b). However, it was not specified whether ‘model’ referred to a modality of practice, a method of formulation, or an explanatory model (e.g., a particular theory of depression). Participants thus appeared to understand this statement in different ways. This notion of loyalty to modality, alongside the notion of tailoring to be discussed next, should hopefully afford greater precision for professional discussions about such issues.
Tailoring of TheoryThis factor asks: ‘how tailored is a formulation or approach to the individual client, relative to extant explanatory theory?’. This may strike some readers as antithetical to the idea of case formulation which is often understood as the task of developing an individualised understanding. In practice however, across cases, contexts, and disciplines, meaningful variation appears to exist on such a factor. This factor can be understood as a continuum, analogous to the tailoring of clothing. On one end an off-the-shelf approach can be placed, whereby nomothetic explanatory models are taken wholescale and applied to an individual client. For example, after diagnosing Generalised Anxiety Disorder, a clinician simply apply Wells’ metacognitive model wholesale (Wells, 1999). An off-the-shelf approach describes a minimum amount of measurement and adjustment to the individual, with benefits of greater efficiency, standardisation, and a more direct connection to research. Under such an approach, diagnosis will substantially constrain formulation, making it less personalised. In the middle of this continuum lies a made-to-measure approach. This describes either beginning with an established explanatory theory and adjusting it meaningfully to suit a particular client (e.g., adding in case specific factors or mechanisms not alluded to in the original theory), or weaving together multiple explanatory theories. In these cases, the form and structure of the formulation is adjusted to fit the individual but is significantly constrained by the original pattern prescribed by the theories drawn upon. On the other far end of the spectrum fall bespoke approaches, whereby an entirely individualised explanation is constructed each time, with minimal predefined content or form. Much like tailoring a bespoke piece of clothing, this does not mean that skill, methodology, and established knowledge do not play a role, simply that the end product is generated de novo to suit the individual client and assessment purpose.
Conceptually this factor is partially related to modal loyalty as it speaks to how constrained/scaffolded a formulation is. While perhaps not entirely orthogonal, it is meaningfully distinct from the loyalty factor in that it can vary independently. For example, someone may formulate loyally within a CBT approach, while taking a more off-the-shelf (e.g., copy-pasting an established model), made-to-measure (e.g., personalised explanation within a classic CBT structure), or bespoke approach (e.g., freely identifying and integrating cognitive and behavioural mechanisms into an explanation). By contrast, someone may conceivably understand formulation in a disloyal/eclectic way, while also not constructing bespoke formulations (e.g., a clinician who frequently understands most psychological problems as being fundamentally about ‘needing to feel in control’).
Explanatory FormThis factor asks: ‘what form of explanation does a formulation take, or an approach to formulation encourage?’. At the simplest level this refers to the mode in which the formulation is represented – i.e., is it written, drawn, formalised as equations, discussed, imagined by the clinician? Beyond this matter, however, this factor is more centrally concerned with what kind of explanation a formulation represents. Work in the philosophy of science demonstrates that explanations can take several different forms (Woodward & Ross, 2021). Applied to formulation several examples of different explanatory forms can be identified. A narrative form focuses on capturing the historical development of a patient’s challenges, creating an accessible understanding of the origins of the problem. Less attention to contextual and originating factors is given in dispositional style explanations, which explain by identifying psychological traits – e.g., narcissism, perfectionism, thought-action fusion (Vanderbeeken & Weber, 2002). Dynamic explanations, by contrast, deprioritise underlying causes and focus on relationships between events, establishing highly localised descriptions of how the problem changes with time and relevant cues/occurrences – e.g., drawing attention to emotional patterns in emotion-focused therapy (Greenberg, 2004), or formulating with personalised network models (Roefs et al., 2022). List-based approaches – e.g., simply listing biopsychosocial factors (i.e., predisposing, precipitating, perpetuating, protective) – appear common in psychological and psychiatric formulation. Whether list-based approaches genuinely explain is debatable as factors are often not integrated. Lastly, mechanistic approaches aim to articulate how the factors established in an assessment interact to bring about and maintain the presenting problem, identifying or inferring processes that help make the problem less surprizing (Glennan & Illari, 2018; Haig, 2014).
Relatedly, a distinction can also be drawn between etiological and compositional explanations (Hawkins-Elder & Ward, 2021; Ward & Clack, 2019). Etiological approaches explain by articulating the origins and causes of the explanatory target (e.g., explaining difficulties in adolescence via maternal alcohol use during pregnancy and other disruptions to early development). A more etiological approach is relevant when there is a need to account for the origins of a problem. Compositional approaches in comparison, explain by describing how the explanatory target currently works or is maintained, often across scales (e.g., explaining the same difficulties in reference to neuro-cognitive and emotional regulation differences and impacts on social functioning). A compositionally focused approach is relevant when seeking to understand what keeps a problem going and how it might be addressed. This distinction in explanatory form thus relates strongly to the intended explanatory purpose.
This factor relating to explanatory form is not widely discussed in literature on formulation. From our perspective, the form that a formulation takes should be tailored to the nature of the problem being explained, the purpose for trying to explain it, and the pragmatic requirements for its effective communication to the intended audience (Potochnik, 2016, 2017).
StabilityThis factor asks: ‘How frequently should a formulation be updated?’. This factor is modelled as a continuum from very stable to very dynamic. On the very stable end, a formulation is seen as a consistent bedrock for therapy and decision making, constructed after assessment and not updated until further formal assessment is undertaken. Somewhere in the middle, an iterative approach describes where formulation is carefully/explicitly updated as new relevant information comes to light. On the very dynamic end sits an understanding of formulation as developping freely, perhaps from session to session. There are connections to both explanatory form and the specificity of the explanatory target here, in that dynamic approaches likely align with highly specific targets and discussed or internally represented explanations. Returning to the same consensus study, most clinicians appear endorse a somewhat dynamic, perhaps iterative approach, whereby formulation is an ongoing process and should be reviewed during the treatment process as new information surfaces (Thrower et al. 2024a, b).
The Nature of “Truth” and EvaluationThis factor concerns: ‘How true is a formulation, and on what basis can it be evaluated?’. This factor is alluded to by Johnston and Dallos (2013). This factor is modelled as a selection of illustrative positions, acknowledging they are neither exhaustive nor mutually exclusive. Taking an empiricist view, formulation would be seen as “true” in so far as it aligns with available evidence (i.e., assessment findings) and makes accurate predictions about future behaviour (i.e., accuracy is a matter of empirical fit). Relatedly but slightly more complex, from an epistemic position, a formulation would be seen as more likely to be true based on its accordance with a range of epistemic values, including but not limited to empirical fit (e.g., simplicity, specificity, lack of contradiction, coherence with wider knowledge). ATOM, described earlier, would be an example of this position (Ward et al., 1999, 2016). A pragmatist position, meanwhile, places less emphasis on ‘truth’ and instead focuses on a formulations ability to serve its intended purpose. Pragmatic perspectives incorporate a wider range of evaluative criteria beyond those primarily concerned with truth – e.g., communicability, capturing maintenance or control factors that are manipulatable (Chang, 2022; Potochnik, 2016). Finally, a social constructionist view emphasises the situated, historical, and subjective nature of all knowledge. From such a perspective a formulation is not so much making a claim to truth that needs to be evaluated, but instead concerns the compiling of different narratives/perspectives on the problem at hand (Harper & Spellman, 2006).
Summary and DiscussionWe have proposed a methodological taxonomy intended to help clinicians and researchers recognise and discuss variation in formulation practices. This taxonomy is summarised in Fig. 1. This taxonomy does not prescribe ideal practices, though in discussion we have occasionally gestured toward positions that seem advantageous for certain aims (e.g., focusing on clinical phenomena when precision is required; employing mechanistic/compositional forms when intervention design is the priority). Our primary aim has been descriptive and communicative: to provide language that might support conceptual competence, reflection, and clearer dialogue within and across disciplines (Aftab & Waterman, 2021). Some limitations are noteworthy. Firstly, this taxonomy is not intended to be exhaustive. Other relevant factors may be missing or may warrant more fine‑grained distinctions. Secondly, this taxonomy is theoretically derived and would benefit from empirical study exploring whether formulation practices do genuinely vary in the described ways.
Fig. 1 The alternative text for this image may have been generated using AI.
The alternative text for this image may have been generated using AI.A Methodological Taxonomy of Formulation Practices. A visual summary of the nine factors. The order and layout do not imply ranking or underlying dimensions, and the categories are neither exhaustive nor mutually exclusive
Despite these limitations, we hope that this taxonomy may be useful in several ways. Individually, it may prompt clinicians to locate their current habits and preferences, to ask how these align with purposes, and to consider other options. Between clinicians, it may facilitate discussion, helping to identify sources of difference and disagreement that are sometimes obscured by ambiguous terms (e.g., “model,” “collaboration”), and facilitate critical discussion regarding how organisational and contextual constraints may influence formulation practices. For training purposes, it may encourage awareness of approaches available, offering a scaffold for teaching formulation as a set of decisions. For research, we hope it will support more precise empirical work on how clinicians formulate, as well as inform greater methodological precision in frameworks that aim to guide formulation practices.
Comments (0)