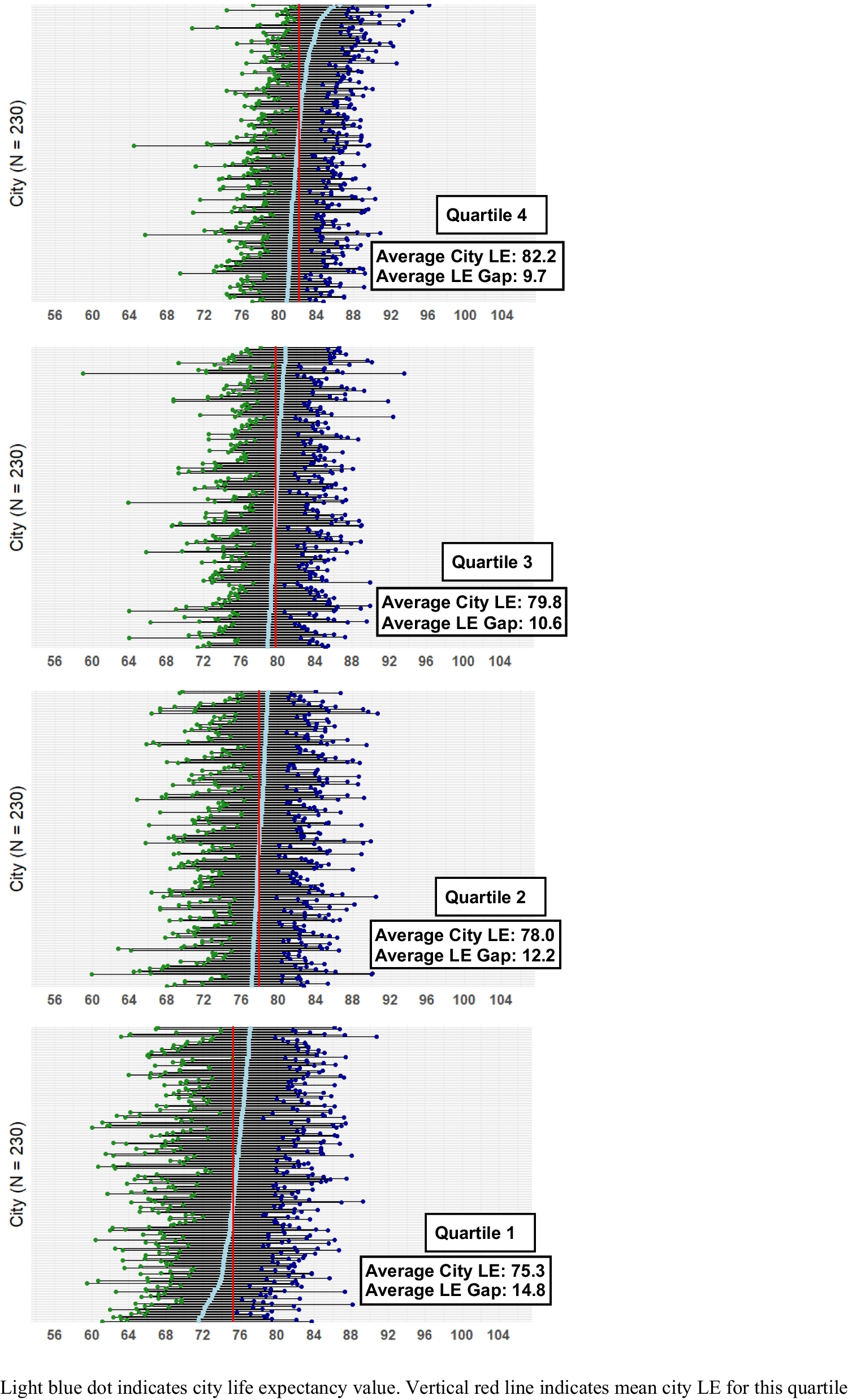
We examined LEGs as a potential measure of the “ground to cover” in setting city-level goals for health equity. LEGs were substantial across all geographic regions throughout the USA, with the highest average gap (15.0 years) observed in the East South-Central division. Even among smaller cities, where gaps are expected to be more modest due to fewer tracts and less potential for outliers, LEGs approximating a decade were commonly observed. Although LEGs decreased as city LE increased, we observed similar (decade-long) gaps in high-LE cities as well. These results are in line with prior research that has explored LEGs in a smaller number of major US [5, 6] and international cities [7] and research identifying strong associations between social drivers of health and similar mortality measures in urban geographies [8, 9]. The current study expands on this research by exploring these patterns in a larger number of US cities (including smaller-population cities) and by focusing on disparities within cities using granular spatial units rather than across demographic groups. The present research additionally suggests the potential of local urban LEGs as a useful tool for health equity goal setting.
Among social and environmental characteristics examined, the strongest correlation with LEGs was with racialized residential segregation, concordant with previous literature [10, 11]. While our descriptive analysis does not analyze potential mechanisms, it raises questions about the influences of environmental conditions, access to education and other resources, and the potential direct effects of exposure to racialized residential segregation on mental and physical health [12]. LEGs were also moderately correlated with city-level median household income and percentage of children in poverty. Substantial LEGs (averaging 9 years) were present even in higher-income cities, underscoring the need for local efforts to impact modifiable neighborhood characteristics to reduce disparities [13]. For example, initiatives to reduce food insecurity, support early childhood development, or optimize health insurance enrollment in specific neighborhoods may help to address within-city LEGs. A limitation of this analysis is that USALEEP estimates are from 2015, and LEGs may have since changed. Additionally, the income inequality variable used was calculated at the city level and so did not capture within-city variations in income inequality. This geographic mismatch between within-city LEGs and city-level income inequality may obscure potential correlation between income inequality and LEGs. Finally, particularly in larger cities, some census tracts may be outliers because of small or unique populations. Rather than asking cities whether specific outlier tracts should be excluded from analysis, as done in a preliminary analysis, our sensitivity and prior analyses suggest that outlier tracts do not skew our conclusions in this paper [14].
Several jurisdictions in the USA have begun to prioritize LEG reduction. The Cincinnati Department of Health is examining neighborhood-specific causes of premature death to inform interventions to reduce LEGs [15]. In Chicago, the Department of Health is using within-city LEGs to target strategies to reduce opioid overdose deaths [16]. The City of Boston published a report articulating similar goals in early 2025 [17, 18]. And New York City established a reduction in LEGs as a central aim of its effort to tailor health improvement strategies to specific neighborhood circumstances [19].
Our analyses demonstrate that significant LEGs exist across US cities. LEGs present a compelling target for municipal governments, health departments, healthcare systems, community organizations, and researchers to use in establishing robust health equity goals. Such efforts are beginning to take hold, and our analyses illuminate opportunities for cities to partner with communities to address neighborhood-level factors that impact LE disparities [20]. Future research can contribute to these efforts by exploring how specific drivers contribute to LEGs and by refining approaches to incorporate uncertainty in LE estimates. LEGs embody a powerful narrative that public health professionals and community leaders can and should leverage in advocating for and setting priorities to advance health equity.





Comments (0)