
Remember me
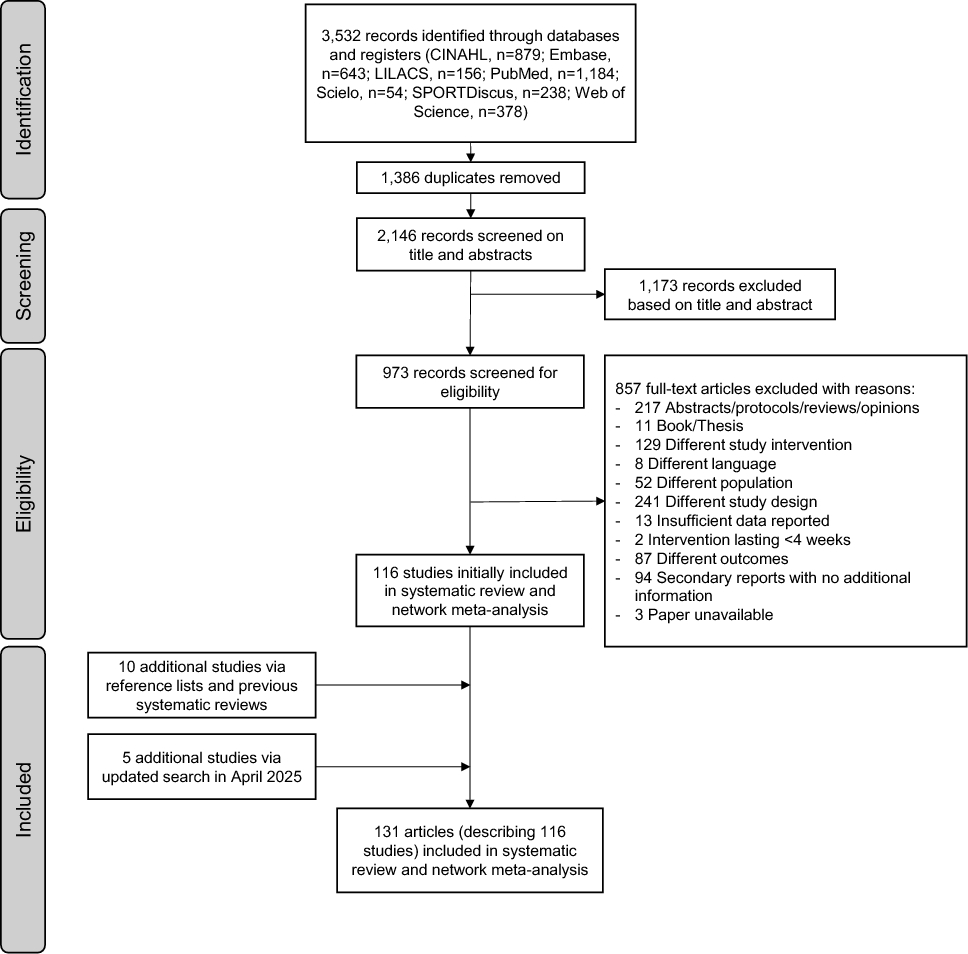
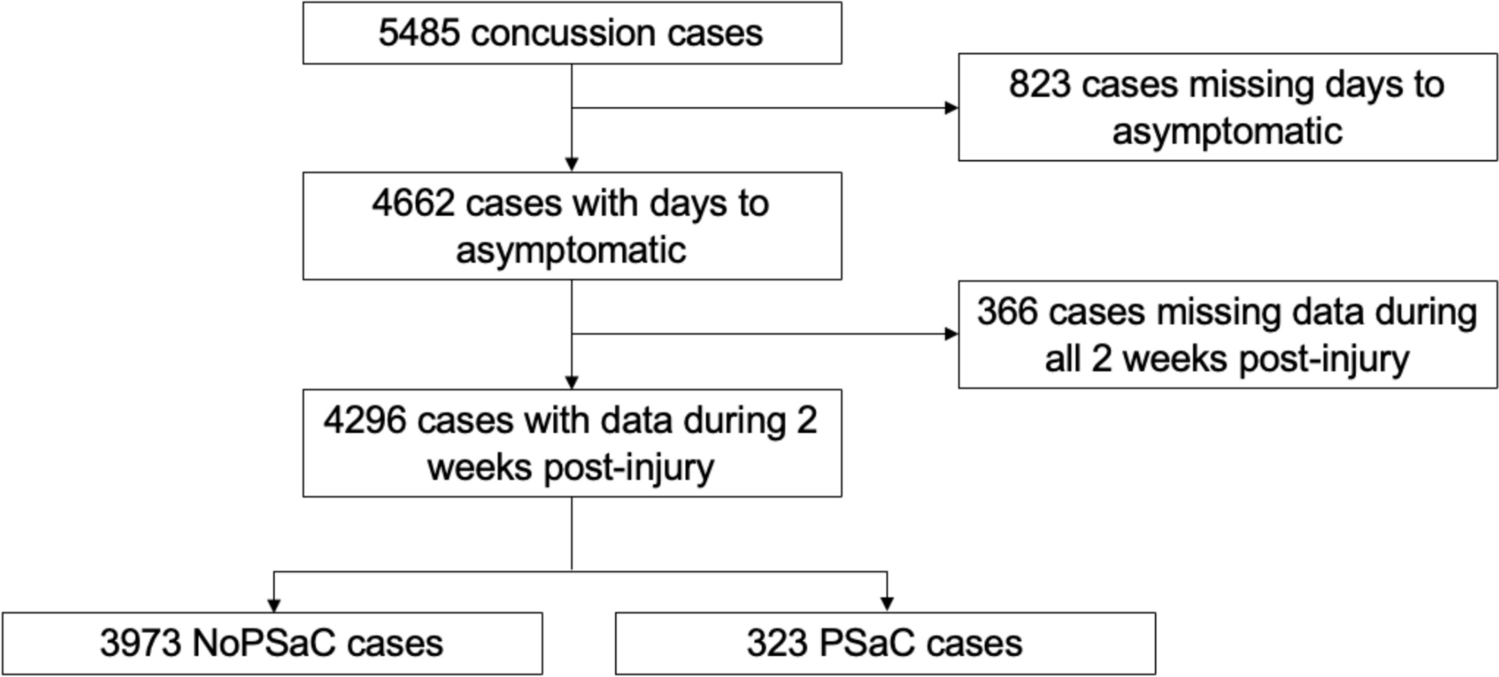
The initial database search (January 2024) returned 2188 studies; updated searches were conducted in December 2024 and November 2025 with a further 602 articles added. After 585 duplicates were removed, 2205 studies remained. The title and abstract review ruled out 2089 studies, leaving 116 studies for full text review (107 retained from title and abstract review and nine additional studies identified from citation searches). Full text review deemed 69 studies to be ineligible. Overall, 47 studies met the inclusion criteria (Fig. 1).
Fig. 1
Preferred reporting items for systematic reviews and meta-analyses. Scoping review flowchart
3.2 Study CharacteristicsThe search yielded 47 studies across seven invasion sports consisting of 18 (38%) ice hockey studies, 11 (24%) tackle football, seven (15%) rugby union, seven (15%) football, two (4%) Australian Rules football, one (2%) rugby league and one (2%) lacrosse (Table 2). Research was predominantly conducted on male athletes with this population being investigated in 35 (75%) studies. A further 11 (23%) studies reported on a mixed population, only three (6%) of which presented disaggregated male and female injury rates. There was only one (2%) study included in the review that focused exclusively on female athletes. A total of 23 (49%) studies investigated youth and adolescent athletes while the remaining 24 (51%) reported on adult populations.
Table 2 Study characteristicsOf the 47 included studies, 17 (36%) reported rule changes significantly reduced the rate or cause of injury or SRC [10, 11, 25,26,27,28,29,30,31,32,33,34,35,36,37,38,39], four (9%) reported a reduction in the rate of injury or SRC but did not report corresponding effect estimates [40,41,42,43], whilst a further seven (15%) studies reported a reduction in the rate of in-game events linked to injury or SRC (e.g., head contacts and foul play) [44,45,46,47,48,49,50]. Of the 28 studies reporting an effective in-game rule change, three of these studies also identified unintended consequences including increased injury severity [10, 35], and transferring the injury risk to an alternative match event [34]. There were six (13%) studies reporting no significant change to either the rate or cause of injury after introducing a rule change [51,52,53,54,55,56] and three (6%) that failed to report a reduction in the rate of injuries or SRC after seeing the intended player behaviour change [57,58,59]. Four (8%) studies reported a significant increase in the rate of injury [60,61,62,63] and a further four (8%) that directly explored the unintended consequences of an in-game rule change [64,65,66,67]. Finally, two (4%) studies reported on the outcome of several injury prevention rule changes over multiple seasons [68, 69]. Full details of all included studies are provided in Supplementary Material 3.
3.3 Ice HockeyOf the 18 studies evaluating ice hockey, 12 investigated male athletes while 6 examined a mixed population. There were 14 rule change studies at amateur level and 4 in an elite setting with studies predominantly focusing on the permitted age of BC and reducing head-to-head contact. Five studies evaluating adolescent BC rules found rates of injury, SRC and head contacts significantly increased for players in leagues where BC was permitted, compared with leagues where BC was disallowed [10, 35, 48, 64, 67]. Emery et al. [11, 25] evaluated this rule in 13–14 and 15–17-year-old cohorts. In leagues where BC was disallowed, they reported a reduction in injury and SRC rates for both the 13–14 [incidence rate ratio (IRR) = 0.45 (95% CI 0.27–0.77); SRC IRR = 0.59 (95% CI 0.31–1.17)] and 15–17 [IRR = 0.30 (95% CI 0.19–0.46); SRC IRR = 0.43 (95% CI 0.24–0.76)]-year-old players [11, 25]. Conversely, one of the studies investigating the unintended consequences of reducing the legal age of BC from players aged 12–13 down to age 9–10 years found no increase in the rate of injury [65]. Watson et al. [40] investigated a rule penalising players who bodychecked their opponent from behind in collegiate hockey leagues: effect estimates were not reported although the rate of head and neck injuries decreased [40].
Five studies evaluated rules prohibiting players from making direct contact to an opponent’s head. Hutchinson et al. [26] evaluated the rule in an elite adult cohort and found no significant change in the rate of SRC but did find a reduction in the rate of SRC caused by blindside bodychecking (i.e. a player is unaware of the BC prior to being struck) [26]. A similar rule change evaluated in a youth cohort initially failed to reduce the rate of head contacts [pre amendment IRR = 0.94 (0.76–1.15)] [56]. After an additional policy amendment where the level of sanction was further increased, the rate of head contacts reduced [IRR = 0.70 (95% CI 0.51–0.95)] [44]. The remaining two studies reported a significant increase in head contact or SRC as a result of implementing the head contact rule change [60, 63]. Three studies evaluated rules increasing the level of sanctions for actions including fighting, repetitive fouling and dangerous BC with all three reporting reductions in either injury or concussion incidence rate [27, 28, 41]. Morrissey et al. [68] evaluated multiple rule changes designed to reduce the rate of SRC. While rates were observed to increase, the authors suggested this may have been a result of improved SRC education, recognition and reporting [68].
3.4 Tackle FootballAll 11 tackle football studies were conducted on male athletes, with 8 studies investigating adult populations. Eight studies [29, 30, 37, 43, 47, 51, 61, 66] evaluated rule changes designed to lower the rate of head collisions. These included altering special teams plays (kick-offs (KO) and punts), banning targeting (deliberately lowering the crown of the helmet to initiate contact) and implementing a mercy rule (activating a rolling game clock in the second half when a score differential has been met to reduce athletes’ exposure time). Of these eight studies, six found a reduction in either the rate or cause of SRC [29, 30, 37, 43, 47, 66]. Baker et al. [66] and Westerman et al. [61] specifically investigated the unintended consequences of the lowering of the helmet/targeting rule. They hypothesised the rule change may cause an increase in lower extremity (LE) injuries. At elite level in the National Football League (NFL), Baker et al. [66] reported a significant reduction in the rate of SRC [IRR = 0.60 (0.50–0.73)] while LE injuries [IRR = 0.97 (95% CI 0.92–1.04)] and severe LE injuries [IRR = 1.15 (95% CI 0.99–1.33)] did not significantly increase [head contact 66]. Westermann et al. [61] found the implementation of the targeting rule in the collegiate game did not have the intended effect as the rate of SRC increased [IRR = 1.34 (95% CI 1.08–1.66)]. The rule also unintentionally increased LE time loss injuries [IRR = 1.21 (95% CI 1.06–1.36)] [61]. One study assessed a KO rule change that aimed to reduce the rate of SRC by increasing the fair catch zone from the 20 to 25-yard line [51]. The rule change did not significantly alter the rate of SRC [IRR = 1.89 (95% CI − 1.22 to 5.01)] [51].
The three remaining studies assessed knee, spinal, SRC, and overall injury rates [31, 36, 42]. Baker et al. [31] evaluated a rule disallowing the chop block, an action where the offensive player dives off their feet towards a defending player's leg in an attempt to bring them to the ground. The rate of knee injuries significantly reduced [IRR = 0.84 (95% CI 0.75–0.96)] after introducing this rule [31]. Torg et al. [42] evaluated a rule change designed to remove spear tackling and headfirst blocking. No effect estimates were reported although the rate of spinal trauma injuries for high school and collegiate athletes reduced by 70% and 65%, respectively [42]. Ruestow et al. [
Comments (0)