
Remember me
Objective:
The aim of this retrospective cohort study was to evaluate the clinical and neonatal outcomes between day 4 and day 5 embryo transfer across different fertilization methods.
Methods:
This retrospective cohort study was conducted between January 2018 and March 2023, enrolling a total of 1,245 fresh embryo transfer cycles, including 1,023 in vitro fertilization (IVF) cycles and 222 intracytoplasmic sperm injection (ICSI) cycles. Among these, IVF cycles included 793 day 4 transfers and 230 day 5 transfers; ICSI cycles included 179 day 4 transfers and 43 day 5 transfers. The study conducted a comparative analysis of clinical pregnancy outcomes between day 4 and day 5 transfers.
Results:
In IVF or ICSI cycles, no significant differences were found in clinical pregnancy rate (CPR), implantation rate (IR), live birth rate (LBR), or other clinical outcomes between transfers of day 4 and day 5 embryos (P > 0.05). In IVF cycles with single high-quality embryo transfer, the CPR (62.72%, P = 0.026), gestational week of delivery (39 weeks, P = 0.026) of day 4 were significantly higher than day 5 (38 weeks). After controlling for potential confounding factors, the CPR of the day 4 group was also higher than day 5 (OR 0.578, 95% CI 0.352-0.949, P = 0.030). In IVF or ICSI cycles with day 4 high-quality embryo transfer, the LBR (63.06%, P = 0.006; 70.37%, P = 0.006) and multiple pregnancy rate (MPR; 53.29%, P < 0.001; 50%, P < 0.001) of transferring double high-quality embryo were significantly higher than transferring single high-quality embryo (LBR: 50.87%, 44.23%; MPR: 0%, 3.23%).
Conclusion:
In IVF or ICSI cycles, day 4 embryo transfer is considered a viable option or alternative to day 5 blastocyst transfer with no difference in clinical and neonatal outcomes. In IVF cycles with single high embryo transfer, day 4 transfer is recommended due to its significantly higher pregnancy rate compared to day 5 transfer. To reducing MPRs and preterm birth rates (PBRs), day 4 single embryo transfer is recommended if embryos achieve high-quality grade (full compaction) on day 4.
BackgroundIn the field of reproductive medicine, in vitro fertilization (IVF) is currently regarded as one of the most important treatments for infertility. Over the past few decades, IVF technology has made significant progress, yet a considerable number of patients still fail to achieve pregnancy. The method of fertilization, embryo quality, and timing of transfer are key factors influencing pregnancy success rates. Currently, many fertility clinics routinely perform day 3 and day 5 embryo transfer in vitro fertilization/intracytoplasmic sperm injection (IVF/ICSI) cycles. Multiple studies indicated that cleavage-stage embryo transfer had a lower clinical pregnancy rate (CPR) and higher miscarriage rate than blastocyst transfer (1, 2). This may be because blastocyst transfer allows for better synchronization between the endometrium and embryo growth, while also enabling the selection of higher-quality embryos (3, 4). However, other studies indicated that the cumulative pregnancy rate of blastocyst transfer was comparable to or even lower than that of cleavage-stage embryo transfer (5, 6).
Day 4 embryo transfer, however, is frequently disregarded. Compared with day 3, the silenced embryonic genome becomes active and the apoptotic system and cellular cycle checkpoints are activated (7). Hsieh et al. (8) demonstrated that day 4 embryos exhibited a higher rate of euploidy. On day 4 after fertilization, uterine contractions diminish, enhancing the receptivity of the endometrium to the embryo (9). Some studies indicated that the success rate of day 4 embryo transfer was significantly higher than that of day 3 transfer (10). In addition, under physiological conditions, the embryo enters the uterine cavity from the fallopian tube around the fourth day after fertilization. Therefore, transferring the embryo on day 4 more closely mimics the natural process. Furthermore, prolonged embryo culture leads to abnormal imprinted gene expression associated with apoptosis, oxidative stress and gap junction formation (11). Compared to day 5 transfer, day 4 transfer shortens the in vitro culture time, thereby reducing the risk of cycle cancellation due to prolonged culture duration. After day 4 embryo transfer, embryos that fail to develop into blastocysts may still develop within the uterine environment and successfully implant. In IVF/ICSI cycles that extend embryo culture to the blastocyst stage may reduce the number of embryos available for freezing and slightly increase the risk of adverse neonatal outcomes (5). Although, there is currently insufficient evidence to establish a causal relationship between the two. Furthermore, time-lapse imaging technology has now been widely adopted. This technology stabilizes environmental conditions, mitigates environmental impacts on embryos, and optimizes embryo selection processes through intelligent analysis of embryonic development, thereby reducing adverse effects of the environment on cultured blastocysts (12).
There are currently several studies on the pregnancy outcomes of day 4 and day 5 embryo transfers. Studies showed that the CPR and live birth rate (LBR) on day 4 of fresh IVF/ICSI cycles were similar to those on day 5 (13–16). Morula embryo transfer might also serve as an alternative option for clinicians in addition to cleavage stage and blastocyst stage (14–16). However, Alper et al. found that transfers of fresh embryos on day 5 were superior to those on day 4 and should be favored (17). Therefore, the superiority of day 4 versus day 5 embryo transfer in clinical outcomes remains unclear. Determining the optimal transfer timing could significantly improve implantation rates (IRs) and LBRs. Moreover, the impact of the fourth day on neonatal outcomes has rarely been reported. This study will investigate the comparison of pregnancy outcomes on day 4 and day 5, as well as the effects of day 4 transfer on newborns.
Different fertilization methods may lead to variations in fertilization and embryo outcomes. Simultaneously, the number and quality of embryos transferred are important factors influencing pregnancy outcomes. Therefore, stratified analysis of fertilization methods, the number and quality of embryos transferred is necessary. Previous studies (13, 16) have compared pregnancy outcomes between day 4 and day 5 embryo transfers, finding similar results. However, these analyses did not account for fertilization methods, embryo quality, or embryo quantity. Alper et al. (17) conducted a stratified analysis of embryo transfer numbers, but their study exclusively employed intracytoplasmic sperm injection (ICSI) fertilization techniques and did not stratify embryo quality. Moreover, their results contradicted previous studies, showing that day-5 embryos yielded superior pregnancy outcomes compared to day-4 embryos. This discrepancy may be attributable to the exclusive use of ICSI fertilization. Sun et al. (15) stratified embryo transfer numbers on day 4 and 5. No significant differences were observed between groups regardless of transferring 1 or 2 embryos. However, they did not perform stratified analysis based on fertilization method or embryo quality. These previous studies have not conducted stratified analyses for different fertilization methods, nor have they performed additional subgroup analyses based on embryo quantity and quality. Furthermore, neonatal outcomes are rarely reported. This study is the first to compare pregnancy and neonatal outcomes following day 4 and day 5 embryo transfers under different fertilization methods. Stratified analyses were also conducted based on the number and quality of embryos transferred. The advantages and disadvantages of various transfer strategies were examined, providing reference for selecting the timing of embryo transfer and developing individualized transfer protocols in assisted reproductive clinical practice.
Materials and methodsStudy design and patientsThis retrospective cohort study was conducted in the Reproductive Medicine Center of Xingtai Meihe Reproductive and Genetic Hospital. The study included patients who underwent a fresh transfer between January 2018 and March 2023, none of whom underwent preimplantation genetic testing (PGT). Exclusion criteria comprised cycles without embryo transfer, cycles with embryo transfer on day 2 or day 3, > 38 years old, endometriosis, genetic, metabolic diseases, congenital uterine abnormalities, other protocols besides gonadotrophin releasing hormone (GnRH) agonist pituitary down-regulation protocol as well as missing data in the electronic medical records.
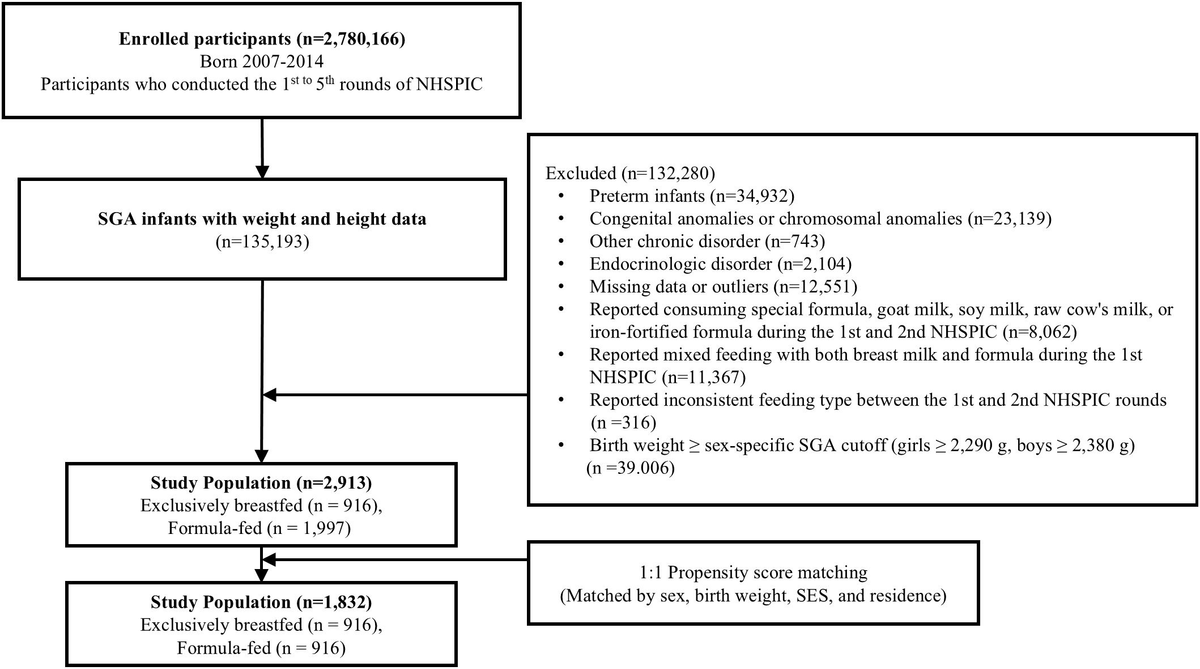
This study included 1,245 fresh transfer cycles, including 1,023 IVF cycles and 222 ICSI cycles. Among these, IVF cycles included 793 day 4 transfers and 230 day 5 transfers; ICSI cycles included 179 day 4 transfers and 43 day 5 transfers (Figure 1). The study conducted a comparative analysis of clinical pregnancy outcomes between day 4 and day 5 transfers. This study was approved by the Ethics Committee of Xingtai Meihe Reproductive and Genetic Hospital (No. 2018-09). According to the Ethics Committee of Xingtai Meihe Reproductive and Genetic Hospital, the requirement for informed consent was waived.

The flow chart of the study population.
Ovarian stimulationPituitary down-regulation protocol using GnRH agonist was administered to all patients. Long-acting Duffelin (IPsen, France) in doses ranging from 1.0 to 3.75 mg was given. Then, 100–225 IU/d of recombinant follicle stimulating hormone (r-FSH, Precon, Merck, Netherlands) were given. Follicle growth was measured by measuring blood levels of progesterone (P), Luteinizing hormone (LH), and estradiol (E2), while follicle size was periodically measured by transvaginal ultrasonography. 6000–10,000 IU of human chorionic gonadotropin (HCG, Zhuhai Lizon Pharmaceutical) was injected when at least two leading follicles measured ≥ 18 mm. After 36–37 hours, the oocytes were retrieved out by vaginal puncture under intravenous anesthesia and ultrasound guidance.
IVF procedures and assessmentIndividual embryos were cultivated in microdroplets using Vitrolife’s G1-PLUS/G2-PLUS sequential media at 37°C in an incubator with saturated humidity, 6% CO2, 5% O2, and 89% N2. One or two embryos were transferred on day 4 or day 5. The 2011 ESHRE Istanbul Consensus (18) was used in our center to score day 4 embryos, while the Gardner scoring system (19) was used for blastocysts. A day 4 embryo that had lost all blastomere boundaries was termed a fully compacted embryo. Day 4 embryos with two pronuclear fertilizations, no vacuoles, and fully compacted (16) were defined as high-quality embryos. Blastocysts were scored in accordance with the Gardner blastocyst scoring system (19) on Day 5. In our laboratory, blastocysts were recorded as high-quality if they reached at least an expansion stage 3 with A or B for inner cell mass (ICM) and trophectoderm (TE). On days 5 and 6, any blastocysts that were not used for transfer would be cryopreserved. The standard for frozen blastocysts is that they reach stage 3 or above and that their ICM score is not C. These blastocysts would then be thawed and transferred once the patient’s physical condition and endometrial environment meet the required standards. Serum β-hCG levels were measured 12–14 days after embryo transfer to determine biochemical pregnancy occurrence. Approximately four weeks post-transfer, transvaginal ultrasound was used to visualize the gestational sac, cardiac tube, and fetal heartbeat. The number of gestational sacs was recorded, and the presence of a gestational sac was considered a clinical pregnancy. Luteal support continued until 12 weeks of gestation, followed by postpartum follow-up.
Clinical outcomesThe primary outcome measure was clinical pregnancy rate. The secondary outcomes variables included rates of live birth, multiple pregnancies, ectopic pregnancy, miscarriage and cumulative live births, as well as neonatal outcomes. Neonatal outcomes included preterm birth, gestational age at delivery, proportion of males.
The clinical pregnancy rate was calculated by dividing the number of patients with at least 1 gestational sac detected by transvaginal ultrasound (performed 28 days after embryo transfer) by the number of patients transferred. A live birth was defined as a live baby delivered after 24 weeks of pregnancy. Multiple pregnancies were defined as the presence of multiple intrauterine fetuses simultaneously. Ectopic pregnancy was diagnosed using ultrasound or laparoscopic imaging of at least one ectopic pregnancy sac. Miscarriage was defined as the loss of fetal cardiac activity within 28 weeks of confirming clinical pregnancy. Preterm birth was defined as a birth before completing 37 weeks of gestation. Cumulative live births refer to the total number of live births achieved within a two-year period across all cycles following the current transfer, including the current fresh cycle and any subsequent frozen-thawed transfer cycles.
Statistical analysisAll data were statistically analyzed using SPSS 22.0 for Windows (IBM, Armonk, NY, USA). The data was examined for normality. The average value of normally distributed measures was expressed as the mean ± standard deviation, and the T-Test for two independent samples was used to compare groups. Continuous variables that did not conform to a normal distribution were expressed as the median (25th, 75th percentile), M (Q1, Q3), and were compared using the Mann-Whitney U test. Categorical variables were expressed as frequencies and proportions and were compared using the chi-square or Fisher’s exact test, P-values < 0.05 were considered statistically significant. A prior power analysis was conducted using G*Power 3.1 with the following parameters: effect size w = 0.3, α err prob = 0.05, power (1-β err prob) = 0.80, and df = 1. The calculation yielded a minimum required sample size of 88 subjects. To investigate the effect of embryonic development days on CPR stratified by fertilization method, we performed multivariate logistic regression analyses. The female age, body mass index (BMI), basal FSH, anti-Müllerian hormone (AMH), type of infertility, infertility factors, E2 on the HCG day, LH on the HCG day, endometrium thickness, the number of retrieved oocytes, embryonic development days were used as independent variables, while the CPR was used as dependent variables in a logistic regression analysis. A significance level of P < 0.05 was considered statistically significant.
ResultsMaternal and cycle characteristicsAs shown in Table 1, comparing day 4 and day 5 embryo transfers across different fertilization methods, no significant differences were observed in baseline characteristics such as female age, BMI, duration of infertility, type of infertility, distribution of infertility factors, basal FSH, basal LH, AMH, total gonadotropins (Gn) doses, Gn duration, E2 on the HCG day, LH on the HCG day, P on the HCG day, endometrial thickness, the number of retrieved oocytes, embryos transferred number and number of high-quality embryos transferred.
VariablesIVFPICSIPD4D5D4D5Cycles(n)79323017943Female age [year, M (Q1, Q3)]30.00 (28, 33)30.00 (28, 33)0.90029.00 (26, 33)29(27,33)0.502Female BMI [kg/m2, M (Q1, Q3)]24.10 (21.60, 26.80)24.20 (22.00, 26.60)0.73923.90 (21.90, 26.25)23.9(21.70,26.40)0.964Infertility duration [years, M (Q1, Q3)]3 (2, 5)3.00 (2, 5)0.5124 (2, 6)4(3,6)0.151Type of infertility (%)0.6910.528Primary infertility36.82 (292/793)38.26 (88/230)54.19 (97/179)48.84 (21/43)Secondary infertility63.18 (501/793)61.74 (142/230)45.81 (82/179)51.16 (22/43)Proportion of infertility factors (%)0.9940.641Unknown cause1.77 (14/793)1.74 (4/230)––Ovulation disorder12.74 (101/793)12.17 (28/230)11.73 (21/179)18.60 (8/43)Male factor1.51 (12/793)1.30 (3/230)58.66 (105/179)55.81 (24/43)Fallopian tube factor80.58 (639/793)80.87 (186/230)22.35 (40/179)20.93 (9/43)Others3.40 (27/793)3.91 (9/230)7.26 (13/179)4.65 (2/43)Basal FSH [U/L, M (Q1, Q3)]6.38 (5.36, 7.55)6.33 (5.17, 7.57)0.7496.33 (5.29, 7.89)6.95 (5.29, 7.96)0.633Basal LH [U/L, M (Q1, Q3)]4.20 (3.00, 6.21)4.20 (3.02, 6.77)0.5484.19 (3.17, 5.60)5.08 (3.38, 6.21)0.194AMH [ng/ml, M (Q1, Q3)]3.72 (2.53, 5.37)3.71 (2.60, 5.43)0.8364.19 (2.70, 5.88)3.76 (2.70, 5.31)0.561Total Gn doses [U, M (Q1, Q3)]2450 (2025, 3000)2475 (2025, 3000)0.5972475 (1950, 2925)2425 (1988, 2875)0.654Gn duration [days, M (Q1, Q3)]11.00 (10, 12)12.00 (10, 13)0.47412.00 (11, 13)12.00(11, 13)0.837E2 on the hCG day [pg/ml, M (Q1, Q3)]2898(1912, 4081)2892 (2000, 4086)0.5373349(2354, 4338)3676 (2587, 4439)0.470LH on the hCG day [U/L, M (Q1, Q3)]0.93 (0.69, 1.25)0.89 (0.66, 1.20)0.1300.89 (0.74, 1.15)0.98 (0.69, 1.15)0.813P on the hCG day [ng/ml, Mean ± SD]0.77 ± 0.270.77 ± 0.270.8590.79 ± 0.280.73 ± 0.220.224Endometrium thickness [mm, Mean ± SD]11.53 ± 2.2311.46 ± 2.470.68411.78 ± 2.2111.99 ± 6.820.736Number of oocytes retrieved [n, Mean ± SD]13.52 ± 4.8414.07 ± 4.860.13313.91 ± 4.6614.33 ± 4.420.597Number of embryos transferred [n, M (Q1, Q3)]2 (1, 2)2 (1, 2)0.0792(1, 2)2 (1, 2)0.600Number of high-quality embryos transferred [n, M (Q1, Q3)]1(0, 2)1 (1, 2)0.8741(0, 2)1 (0, 2)0.830Baseline characteristics of the patients among day 4 and day 5 group stratified by fertilization method.
Clinical outcomes and neonatal outcomesTable 2 provides a detailed overview of pregnancy outcomes between day 4 and day 5 embryo transfer cycles stratified by fertilization method. From these data, regardless of whether IVF or ICSI fertilization method, we found no significant differences in CPR, implantation rate (IR), LBR, miscarriage rate, multiple pregnancy rate (MPR), ectopic pregnancy rate, monozygotic twins rate and cumulative live birth rate (CLBR) between day 4 and day 5 embryo transfers. Neonatal outcomes, such as premature birth rate (PBR), stillbirth rate, cesarean section rate, gestational week of delivery, male/female ratio and live birth weight also showed no significant differences.
VariablesIVFPICSIPD4D5D4D5Cycles(n)79323017943Clinical Pregnancy rate (%)63.93(507/793)58.70(135/230)0.14865.36 (117/179)65.12 (28/43)0.976Implantation rate (%)51.09(655/1282)50.98(182/357)0.97051.49 (155/303)57.14 (39/71)0.567Live birth rate (%)53.09(421/793)48.70(112/230)0.24055.31 (99/179)51.16 (22/43)0.624Ectopic pregnancy rate (%)0.39(2/507)0.74(1/135)0.5080.85 (1/117)0(0/28)1.000Multiple pregnancy rate (%)29.59(150/507)34.81(47/135)0.24232.48 (38/117)39.29 (11/28)0.494Monozygotic twins rate (%)1.58(8/507)1.48(2/135)1.0000.85 (1/117)3.57 (1/28)0.350Miscarriage rate (%)15.58(79/507)16.30(22/135)0.83911.97 (14/117)21.43 (6/28)0.318Premature birth rate (%)16.17(82/507)16.30(22/135)0.97314.53 (17/117)7.14 (2/28)0.466Stillbirth rate (%)0(0/507)0(0/135)/0.85 (1/117)0 (0/28)1.000Cesarean section rate (%)57.99(294/507)65.93(89/135)0.09558.97 (69/117)67.86 (19/28)0.387Gestational week of delivery [weeks, M (Q1, Q3)]38(37,39)38(37,39)0.06738 (37,39)38 (37,39)0.584Male/female ratio0.99(267/273)1.18(80/68)0.3200.97 (61/63)1.31 (17/13)0.463Live birth weight [g, M (Q1, Q3)]3000(2500, 3400)2900(2550, 3388)0.6493200 (2600, 3500)3000 (2663, 3188)0.330Cumulative live birth rate (%)73.27 (581/793)71.30 (164/230)0.55668.72 (123/179)74.42 (32/43)0.464The clinical outcomes of the patients in day 4 and day 5 group stratified by fertilization method.
Clinical and neonatal outcomes in subgroup analysesTables 3-5 present a subgroup analysis evaluating the effect of the number and quality of embryos transferred on clinical outcomes. No further analysis was conducted for cycles involving the transfer of one high-quality and one non-high-quality embryo, as it was impossible to determine which embryo had successfully implanted. In addition, due to the limited number of single non-high-quality embryo transfers (IVF: 31 cycles, ICSI: 5 cycles), no further subgroup analysis was conducted. In IVF cycles with single high-quality embryo transfer, the CPR (62.72%, P = 0.026), gestational week of delivery (39 weeks, P = 0.026) of day 4 were significantly higher than day 5 (49.44%, 38 weeks) (Table 3). The LBR showed a trend toward increase but without significant difference. There was also no significant difference in CLBR. In IVF or ICSI cycles with double high-quality embryo transfer (Table 4), there were no significant difference in CPR, IR, LBR and CLBR between days 4 and 5 (P > 0.05). The same results were observed in IVF or ICSI cycles with double non-high-quality embryo transfer (Table 5).
VariablesIVFPICSIPD4D5D4D5Cycles(n)287895213Clinical Pregnancy rate (%)62.72 (180/287)49.44 (44/89)0.02659.62 (31/52)61.54 (8/13)0.899Implantation rate (%)62.72 (180/287)49.44 (44/89)0.02661.54 (32/52)61.54 (8/13)1.000Live birth rate (%)50.87 (146/287)41.57 (37/89)0.12544.23 (23/52)38.46(5/13)0.707Multiple pregnancy rate (%)0 (0/180)0 (0/44)/3.23 (1/31)0(0/8)0.607premature birth rate (%)5.56 (10/180)4.55 (2/44)1.0009.68 (3/31)12.51 (1/8)1.000Gestational week of delivery [g, M (Q1, Q3)]39 (38, 40)38 (38, 39)0.02638 (37, 39)38(38, 39)0.813Cumulative live birth rate (%)75.61 (217/287)71.91 (64/89)0.48371.15 (37/52)61.54 (8/13)0.502Outcomes of single high-quality embryo transfer on D4 and D5 stratified by fertilization method.
VariablesIVFPICSIPD4D5D4D5Cycles222635414Clinical Pregnancy rate (%)75.23 (167/222)73.02 (46/63)0.72277.78 (42/54)71.43 (10/14)0.884Implantation rate (%)57.49(255/444)59.85(76/126)0.56258.33 (63/108)57.14 (16/28)0.909Live birth rate (%)63.06 (140/222)61.90 (39/63)0.86770.37 (38/54)50 (7/14)0.263Multiple pregnancy rate (%)53.29 (89/167)65.22 (30/46)0.14950 (21/42)60 (6/10)0.828premature birth rate (%)26.95 (45/167)21.74 (10/46)0.47521.43 (9/42)10 (1/10)0.706Gestational week of delivery [g, M (Q1, Q3)]38 (36, 39)37 (37, 39)0.75038 (37, 39)37 (37, 38)0.464
Comments (0)