
Remember me






A 52-year-old woman with a past medical history of asthma, obesity (BMI > 35), abnormal uterine bleeding, anemia, and acute myeloid leukemia (AML, status post chemotherapy) presented to the emergency department for sudden onset right lower quadrant (RLQ) pain. On admission, she was found to have fever, tachycardia, and tenderness to palpation in the right lower quadrant without rebound or guarding. Laboratory testing was notable for leukocytosis (87.3 × 109 cells/L) with an elevated neutrophil count (9.5 × 109 cells/L) and left shift (immature granulocyte count 4.73 × 109 cells/L), anemia (Hb 7.9 g/dL, Hct 21.2%), thrombocytopenia (29 × 109 platelets/L), and increased circulating blasts (24% on manual differential).
She was diagnosed 1 year prior to presentation with AML with monocytic differentiation via flow cytometry of peripheral blood showing a population of 18.4–24.3% abnormal cells positive for CD13, CD33, CD34, CD117, and CD123; bone marrow aspirate demonstrating a lack of erythroid and megakaryocyte lineages and a large population of atypical monocytes; and normal cytogenetics and FISH. Further genetic testing found the blasts were positive for NPM1, DNMTA3, and IDH1 gene mutations and negative for FLT3-ITD. She was treated with induction therapy 7+3 chemotherapy regimen (cytarabine and idarubicin) with four cycles of consolidation with high-dose cytarabine chemotherapy leading to complete remission on post-treatment bone marrow biopsy. One month prior to the current presentation, she was admitted for interventional radiology–assisted bone marrow biopsy due to persistent pancytopenia. Flow cytometry from bone marrow aspirate showed 41.5% blasts positive for CD33, CD45, and CD117 suggesting relapsed AML. Due to the presence of IDH1 mutation, the patient elected to enroll in a clinical trial for an experimental oral mutant IDH1 inhibitor.
On evaluation in the emergency department, CT scan demonstrated appendiceal enlargement (1 cm at the largest extent) with fat stranding suggestive of acute appendicitis.
Repeated bone marrow evaluation found a hypercellular marrow (> 90%) with reduced trilineage hematopoiesis; 32.7% abnormal blast cells positive for CD11c, CD33, CD45, and CD117; and 35.3% monocytes. The patient was treated for suspected differentiation syndrome, a known complication of IDH1 inhibitor drugs suggested by the monocytic predominance in the bone marrow biopsy, and a laparoscopic appendectomy was performed 4 days following the initial presentation [1].
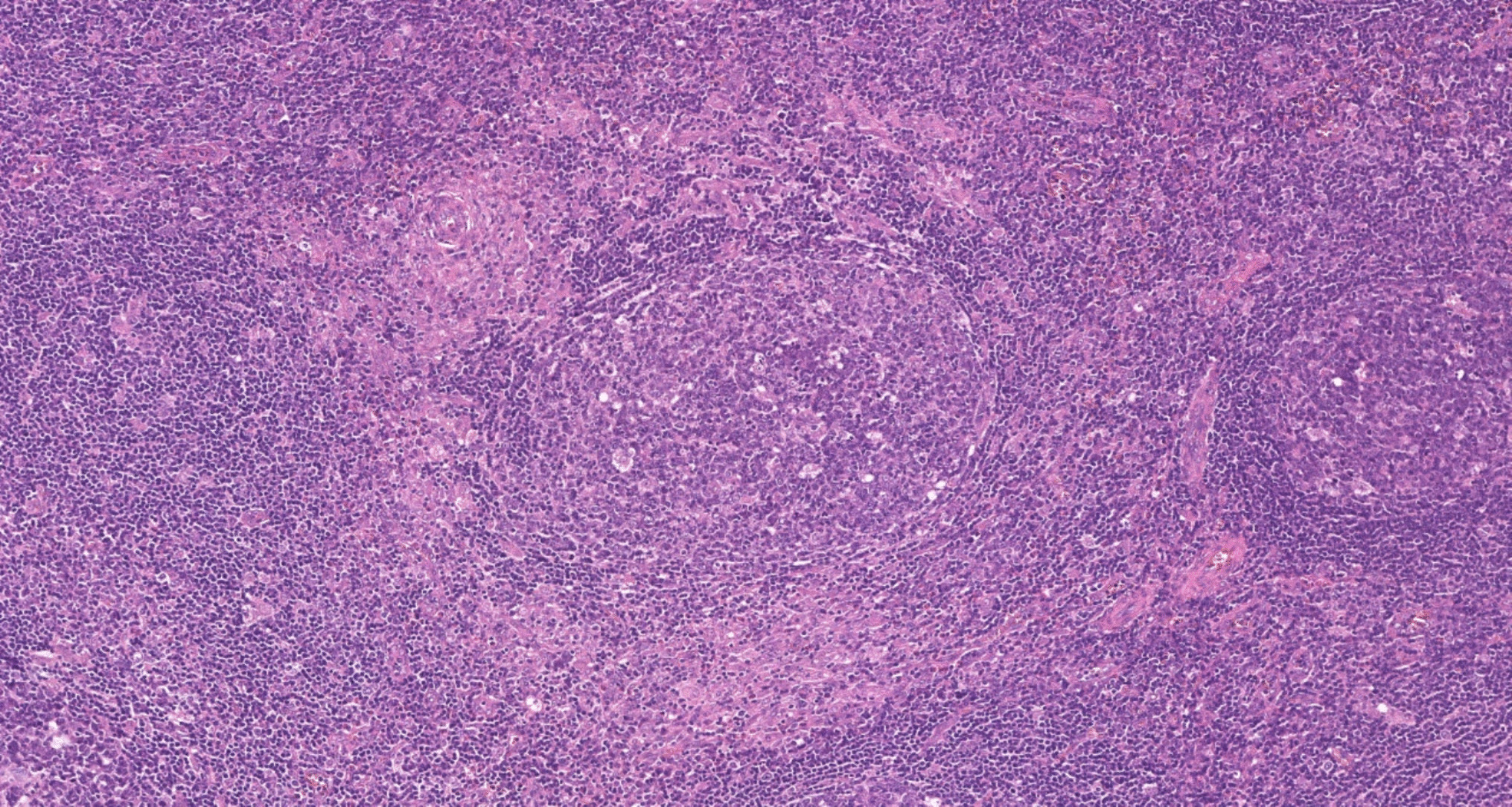
Intraoperative assessment characterized the appendix as acutely inflamed, distended, non-purulent, non-perforated, and not associated with any peri-appendiceal inflammation or free fluid in the pelvis. On pathological exam, the appendix measured 7.0 × 1.5 × 1.4 cm with the appendiceal wall up to 0.4 cm in thickness. The serosa and mucosa were tan-red, and the lumen of the appendix was filled with hemorrhagic fecal material. On microscopic exam, there was extensive infiltration of the mucosa, submucosa, and muscularis layer with atypical medium to large cells with irregular nuclear contours, delicate chromatin, and high nuclear to cytoplasm ratio. Additionally, numerous mitotic figures were noted. Notably, inflammatory changes associated with typical appendicitis were not seen (e.g., neutrophilic predominance). The atypical cells were characterized as myeloid precursors. Immunohistochemical stains confirmed this, as they displayed a similar staining phenotype to the leukemic cells in the bone marrow: they were positive for CD33, CD117, and myeloperoxidase (MPO), while being negative for CD3, CD20, and CD34 (Fig. 1). This analysis led to the diagnosis of appendicitis caused by acute myeloid leukemic cell infiltration.
Fig. 1
Cross section of the appendix. A H&E low power (×40) showing wall infiltration distinct from appendiceal lymphoid tissue. B H&E intermediate power (×100) showing atypical cells, mitotic figures, and variable nuclear to cytoplasmic ratio. Note the lack of neutrophilic infiltration. C H&E high power (×400) showing further detail. D MPO stain intermediate power (×200) showing myeloid-lineage leukemic cells in the tissue. E CD117 stain intermediate power (×200) showing immature myeloid-lineage leukemic cells in the tissue
Following appendectomy, the patient was discharged from the hospital with a plan for further chemotherapy. Flow cytometry of peripheral blood found circulating blasts (19%) and a rising FLT3-ITD mutation. Ten months after the initial presentation for abdominal pain, despite several rounds of chemotherapy, a repeat bone marrow biopsy found a high percentage of myeloblasts (> 60%). The patient’s disease was resistant to salvage chemotherapy, and she passed away 2 months later.
Comments (0)