
Remember me
Inclusion criteria: ① Age 65–75 years old; ② Primary knee osteoarthritis (Kellgren-Lawrence grade III-IV); ③ First unilateral total knee arthroplasty (TKA); ④ Knee valgus 0–15° and AORI Type I; ⑤ Complete clinical data and completed relevant follow-up.
Exclusion criteria: ① History of knee surgery; ② Active infection or inflammatory joint disease; ③ Severe bone defect; ④ Severe systemic disease; ⑤ Neuromuscular disorder; ⑥ BMI > 35 kg/m².
Doctor qualifications and training1 junior doctor: 5 years or less of joint surgery experience, and the number of primary TKAs performed by the lead surgeon before RA-TKA was less than 100 cases.
1 senior doctor: 15 years or more of joint surgery experience, and the number of primary TKAs performed by the lead surgeon before RA-TKA was more than 1000 cases.
All participating doctors completed the manufacturer’s standardized training for the used robot system (Huawei HURWA) (the first 5 RA-TKAs performed). This setting ensures that the surgeon and the surgical team have an initial adaptation to the robot. All research cases were handled by the same group of 3 orthopedic physicians and 2 senior specialist nurses as fixed assistants to control for the confounding effect of assistant experience [5].
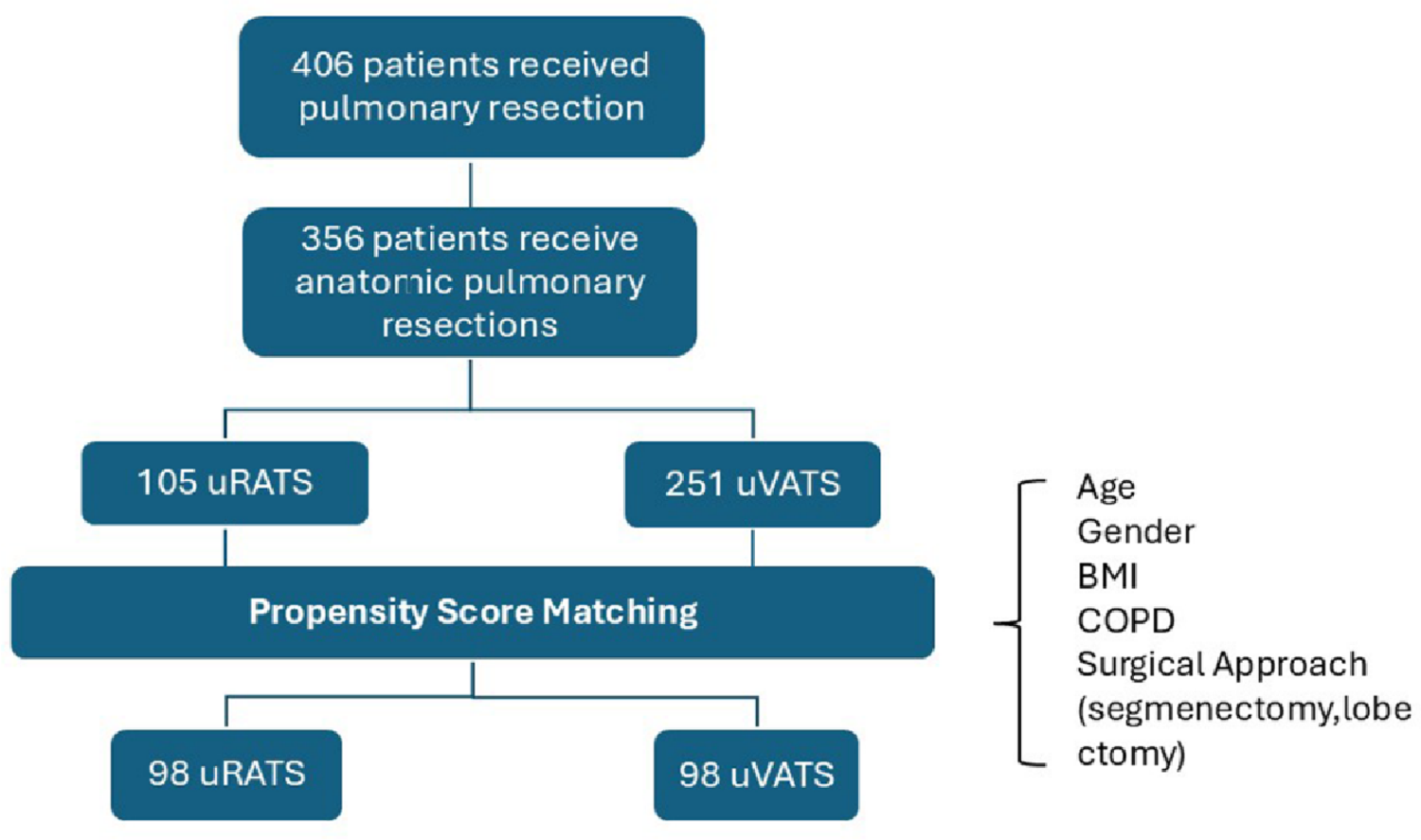
Clinical dataThis study retrieved cases of knee osteoarthritis that underwent total knee arthroplasty at our center from January 2023 to December 2024. According to the inclusion and exclusion criteria, 25 patients from each group were selected from the case database in chronological order:
A-CTKA group: junior doctors + traditional TKA (25 cases of CTKA before RA-TKA);
A-RA-TKA group: junior doctors + RA-TKA (25 consecutive cases of RA-TKA);
B-CTKA group: senior doctors + traditional TKA (25 cases of CTKA before RA-TKA);
B-RA-TKA group: senior doctors + RA-TKA (25 consecutive cases of RA-TKA).
Surgery and perioperative managementAll surgeries were performed under general anesthesia combined with nerve block, with the use of tourniquets. The traditional TKA group adopted standard intramedullary/extra-medullary positioning and gap balance techniques. The RA-TKA group followed the standard procedure of the system: preoperative CT three-dimensional planning, intraoperative optical tracker registration, and mechanical arm-assisted osteotomy. After the osteotomy was completed and the gap balance was achieved, pulse irrigation of the surgical area was performed, followed by the implantation of the prosthesis, 2 − 0 barbed sutures were used to suture the joint capsule, 1 − 0 barbed sutures were used to suture the subcutaneous tissue, skin staples were used to close the incision, and pressure bandaging of the knee joint with dressings was applied. The surgery was concluded.
NoteThe HURWA system is based on preoperative hip-knee-ankle CT. Traditional TKA uses femoral intramedullary positioning + tibial extra-medullary positioning. The alignment strategy for all cases of the knee joint was mechanical alignment (target HKA was 180°), and the balance of the inside and outside of the joint and flexion-extension relied on joint release. When the lateral and medial gaps were significantly abnormal, the HKA was allowed to deviate from the target by 3° or less. All cases used the Aikang PS type prosthesis.
All patients were managed according to the same enhanced recovery after surgery (ERAS) pathway: ① Antifibrinolytic regimen: 2 g tranexamic acid was intravenously infused before the operation, 3 g was infused into the joint cavity after joint capsule suture, and 1 g was intravenously infused again at 3 h, 6 h, and 24 h after the operation; ② Anticoagulation regimen: rivaroxaban was orally administered 10 mg daily for 30 days; ③ Infection prevention: cefuroxime sodium 0.75 g was intravenously infused within 24 h after the operation; ④ Analgesic regimen: 0.1 g celecoxib was taken orally before and after the operation, and oxycodone was added when the pain was unbearable after the operation; intraoperative local injection of ropivacaine 100 mg + compound betamethasone 7 mg + 40 ml normal saline was performed; ⑤ Rehabilitation regimen: professional rehabilitation therapists guided knee joint functional exercises on the first day after the operation, and patients were instructed to return to the hospital for follow-up visits regularly after discharge.
 Evaluation indicatorsPrimary endpoint
Evaluation indicatorsPrimary endpointLower Limb Alignment: Hip-Knee-Ankle Angle (HKA), with the target being 180°, the proportion of patients whose HKA angle is within ± 3° after surgery is regarded as the primary imaging endpoint [9].
Secondary endpointsImaging: The proportion of FFC, FTC, and LTC within ± 3° (target 90°); the mean absolute deviation from the target value for each angle. Clinical Function: KSS, VAS, and ROM at 3 days after surgery (early rehabilitation) and 1 year after surgery (long-term efficacy).
Surgical comparisonSurgical Efficiency: Total operation time (from incision to suture), robot-specific operation time (from installing the tracer to completing the robot-assisted osteotomy).
Perioperative Indicators: Incision length, intraoperative blood loss (weighing method using gauze and suction device).
Complications: ① Intraoperative popliteal artery injury, postoperative foot drop (peroneal nerve injury); ② Postoperative incision infection or exudation for more than 5 days; ③ Venous thrombosis in the affected limb within 1 week after surgery (all cases underwent lower limb vascular color Doppler ultrasound复查 1 week after surgery); ④ Knee lateral DR at 1 day after surgery suggesting anterior cortical depression (NOTCH) of the femur༛ ⑤ Reoperation rate within 1 year due to infection, loosening, stiffness, pain, etc.
Postoperative DR images were measured by two independent orthopedic physicians who were blinded to the groups. To evaluate the measurement reliability, 20 sets of complete images of patients were randomly selected, and two physicians conducted two measurements 2 weeks apart. The intraclass correlation coefficient (ICC, two-factor random effects model, absolute consistency) was used to evaluate the inter-observer and intra-observer reliability. The results showed that the inter-observer ICC of all imaging angles (HKA, FFC, FTC, LTC) was 0.92–0.98, and the intra-observer ICC was 0.95–0.99, indicating excellent reliability of the measurement. The final results were the average of the first measurements by the two physicians for statistical analysis.
Statistical analysisStatistical analysis was conducted using SPSS 26.0 software. For continuous variables, the Shapiro-Wilk test was used to assess normality. All variables were found to follow a normal distribution. Categorical variables were expressed as frequencies (percentages). For age, BMI, preoperative HKA angle, operation time, robot-specific time, incision length, and intraoperative blood loss, these measurement data were presented as (x̅ ± s), and comparisons between groups were performed using the independent sample *t* test. For the proportion of patients with a deviation of ≤ 3° in the postoperative hip-knee-ankle angle (HKA) from the target value of 180°, as a binary variable, the risk difference (RD) and its 95% confidence interval (CI) were analyzed. For comparisons of continuous variables (angle deviation values, KSS, VAS, ROM), the mean difference (MD) and its 95% CI were reported along with the x̅ ± s and P values. Among these, KSS, VAS, and ROM at different time points (3 days post-operation, 1 year) were evaluated using repeated measures variance analysis. For comparisons of categorical variables (such as gender, K-L classification, complication rate), the chi-square test was used; when the expected frequency in any cell was < 5, the Fisher’s exact probability method was employed. To control the Type I error inflation caused by multiple comparisons, the significance level for multiple secondary imaging endpoints (FFC, FTC, LTC outlier ratio) was corrected using Bonferroni (corrected α = 0.017). The significance level (α) was set at 0.05, and a two-sided P < 0.05 was considered statistically significant.
Comments (0)