
Remember me








As global populations age, the increasing proportions of older adults pose various risks and challenges for individuals and families, and for social, economic, and health care systems. The need for preventive health care strategies to reduce, delay, or prevent chronic diseases while maintaining independent living has become important []. The age-related loss of muscle mass, strength, and function is influenced by aging, disease, and other lifestyle factors. Physical inactivity, malnutrition, unhealthy habits, and chronic diseases further increase the risk of sarcopenia, leading to decreased survival rates, prolonged hospitalization, falls, fractures, metabolic disorders, and cognitive impairment, finally diminishing the quality of life []. In addition, aging is associated with sensory decline and cognitive deterioration, severely influencing independence, self-care abilities, and overall well-being among older adults. However, increased physical activity and structured exercise interventions can mitigate the adverse effects of aging, thereby improving the quality of life [].
Regular exercise interventions enhance physical fitness in older adults, reduce fall risks, improve mobility, and prevent certain conditions, including cardiovascular diseases, cognitive impairment, osteoporosis, and muscle weakness, all of which enhance the quality of life []. Moreover, age has a significant impact on the quality of life among older adults, whereas engagement in physical activity contributes to enhancing their quality of life, thereby promoting healthier lifestyles and greater personal independence []. Compared with other types of exercise-based interventions, previous studies have indicated that resistance-based interventions are the most effective for enhancing physical activity and strength; however, age and sex may act as confounding factors influencing these outcomes []. Therefore, in the context of global aging, maintaining health-related physical fitness is essential for delaying muscle loss, preventing falls and injuries, and mitigating chronic diseases, all of which improve the quality of life. Exercise programs, consequently, play an indispensable role in promoting healthy aging.
With rapid technological advancements, active video games and exergames provide older adults with diverse training options beyond traditional fitness programs. Wii Fit (Nintendo) exercise games enhance balance functions in community-dwelling older adults while improving their self-perceived confidence, with high acceptance rates among older populations []. Based on the experiences and needs of older adults, exergames are perceived as enjoyable and engaging. In addition to promoting physical activity, they can help alleviate feelings of loneliness and are not constrained by specific usage conditions. The development of well-designed exergames may therefore provide valuable support for this population []. Compared with traditional exercise methods, Kinect-based (Microsoft Corporation) exergames have demonstrated superior efficacy in improving executive function, cognitive performance, and functional fitness []. In addition, exergames enhance motivation for physical activity, enabling older adults to experience exercise benefits engagingly and enjoyably []. Compared with conventional exercise training, exergames not only improve physical fitness but also provide cognitive and psychological benefits. Therefore, exergames are a promising strategy for health promotion and wellness among the aging population.
Recent meta-analyses have consistently reported that exergame interventions in older adults produce small-to-moderate improvements in balance, mobility, and engagement [,]. A more recent systematic review further highlighted that home-based exergames are generally well accepted and improve mobility-related outcomes such as the Timed Up and Go test []. These findings underscore the potential of gamified training to enhance functional fitness; however, most previous protocols have focused on platforms such as Wii or Kinect, often emphasizing balance or general mobility with limited attention to agility. In contrast, the present exploratory trial used a novel “stampede” agility-focused exergame delivered twice weekly via the mat exercise, integrating multidirectional stepping, reaction-based tasks, and functional movements. The specified exergames, such as Wii and Kinect, can be integrated with motion-sensing technology and have demonstrated applications beyond entertainment, extending to therapy, rehabilitation, and health promotion. However, as both Wii and Kinect have been discontinued, their long-term applicability is limited, underscoring the need for developing updated platforms tailored for diverse populations. However, assessing movement quality remains a critical concern in implementing exergames, because inappropriate compensatory movement patterns may impact both effectiveness and safety [].
Therefore, this study seeks to introduce an exercise mat training program led by a certified coach and to investigate its effectiveness within a 10-week comprehensive training regimen designed within the exergame framework. This protocol design addresses agility and dynamic balance more directly than the majority of exergame interventions previously synthesized in meta-analyses, thereby contributing new evidence on the scope and feasibility of agility-oriented exergaming for older adults. We aimed to evaluate functional fitness in older adults using both the standard Senior Fitness Test and the sport technology–based AFAscan fitness assessment. Furthermore, we intended to explore overall physical activity levels and quality of life. We hypothesized that a well-designed exergame program incorporating novel exercise mat training may enhance not only physical fitness but also physical activity and quality of life.
In this exploratory trial, we recruited older adults aged 60-80 years from the University Social Responsibility program at National Taipei University of Nursing and Health Sciences University (Taipei City), and used a randomized parallel design. A total of 32 participants were randomly assigned to either the experimental (n=16) or control group (n=16) through simple randomization using a random number table, with an allocation ratio of 1:1. The personnel (research assistant) responsible for enrolling participants and those (principal investigator) managing the random allocation sequence were distinct, ensuring that the allocation process remained blinded and minimizing the potential for allocation bias. A pre- and postintervention design was implemented. The intervention consisted of a 70-minute exergame-based mat training session conducted twice weekly for 10 consecutive weeks. Each session included a 10-minute warm-up, approximately 45 minutes of primary training, and a 15-minute cooldown and stretching routine (). Participants completed the International Physical Activity Questionnaire (IPAQ) and the World Health Organization Quality of Life questionnaire (WHOQOL-BREF, Taiwanese Version) before and after the intervention. In addition, the Senior Functional Test and AFAscan fitness assessment (Scanleader, Scanleader Technologies Co. Ltd.) were conducted. Participants in the control group were instructed to maintain their usual daily activities without any additional structured exercise intervention during the study period. A no-intervention control condition was selected to provide a natural reference for functional fitness and quality-of-life changes without training. This approach allowed us to better isolate the effects of the exergame-based mat training and is consistent with previous exercise trials involving older adults.
Table 1. Training schedule, objectives, and equipment of the exergame-based mat program.WeekWarm-upMain course (training objectives)CooldownIndicator light modeEquipment1Stretching exercise and built-in programFlexibility, agility, upper and lower limb strength, core muscles, cardioStretchingAll light on, circle light on, 4 cornersMedicine ball2Stretching exercise and built-in programAgility, balance, lower limb strengthStretchingAll light on, circle light on, 4 cornersMedicine ball3Stretching exercise and built-in programAgility, cardio, upper and lower limb strength, flexibilityStretchingAll light on, circle light on, 4 cornersMedicine ball4Stretching exercise and built-in programLower limb strength, cardio, flexibilityStretchingAll light on, circle light on, 4 corners, 2 lines, diamondElastic band, medicine ball5Stretching exercise and built-in programUpper and lower limb strength, balance, core musclesStretchingAll light on, circle light on, 4 corners, 2 lines, diamondElastic band, medicine ball, kettlebell6Stretching exercise and built-in programCore muscles, upper and lower limb strength, agilityStretchingAll light on, circle light on, 4 corners, 2 lines, diamondElastic band, medicine ball, kettlebell7Stretching exercise and built-in programCore muscles, upper and lower limb strength, cardioStretchingAll light on, circle light on, 4 corners, 2 lines, diamondElastic band, medicine ball, kettlebell8Stretching exercise and built-in programUpper and lower limb strength, core muscles, agilityStretchingAll light on, circle light on, 4 corners, 2 lines, diamondElastic band, medicine ball, kettlebell9Stretching exercise and built-in programUpper and lower limb strength, core muscles, balanceStretchingAll light on, circle light on, 4 corners, 2 lines, diamondElastic band, medicine ball, kettlebell, balance cushion10Stretching exercise and built-in programUpper and lower limb strength, lower limb explosive strength, balance, core musclesStretchingAll light on, circle light on, 4 corners, 2 lines, diamondElastic band, medicine ball, kettlebell, balance cushionaThe lighting modes of the mat serve as visual cues, guiding participants to step on specific areas to turn off the lights as part of the exercise protocol.
bThe built-in program comprises five regular exercise games (lights out game, jumping jacks, reactions, two-way jumping jacks, and whack-a-mole).
A randomized parallel-controlled clinical trial was conducted. A total of 32 eligible participants were randomly assigned to 2 groups: control group and experimental group. The participants completed questionnaires (the IPAQ and WHOQOL-BREF), along with physical fitness assessments (Senior Fitness Test and AFAscan Fitness Assessment), before and after the intervention. Finally, 30 participants completed all experimental procedures required for data analysis.
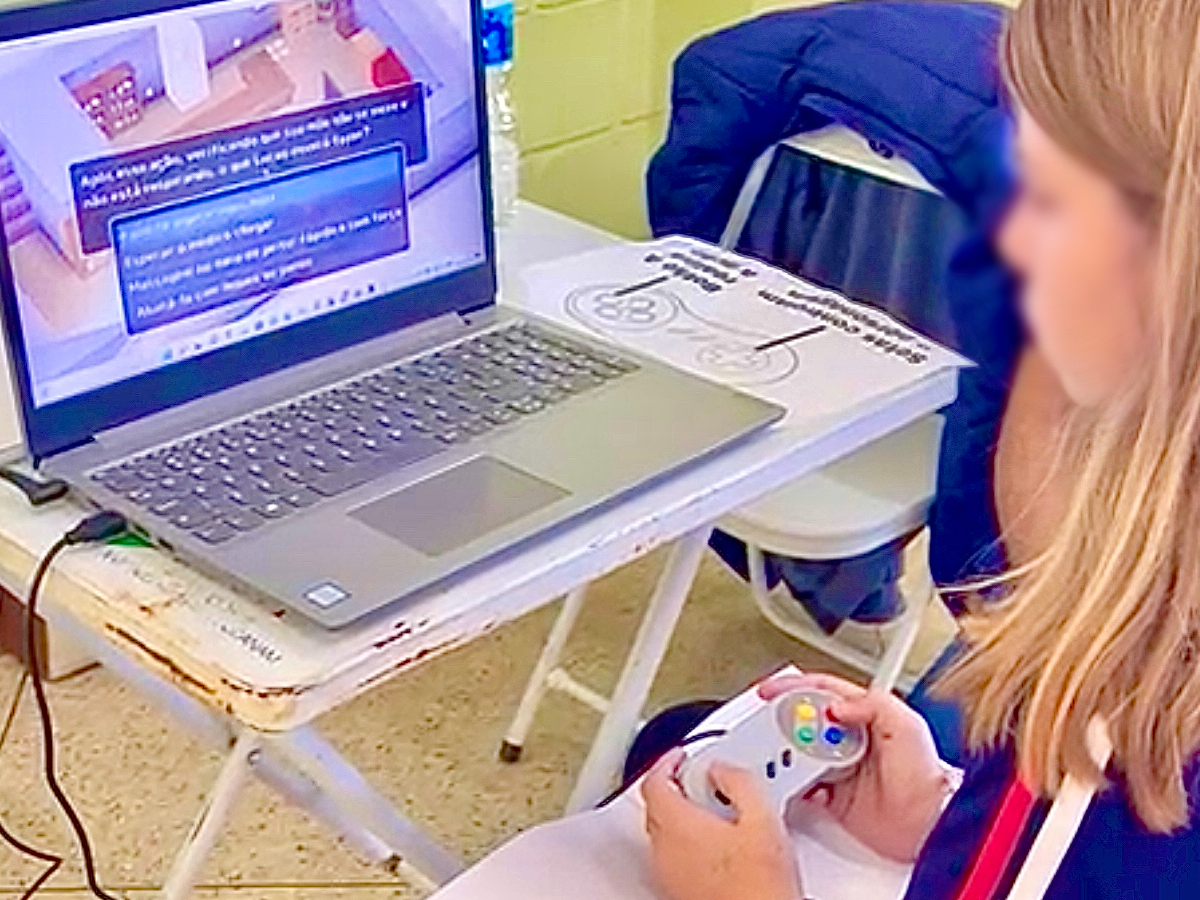
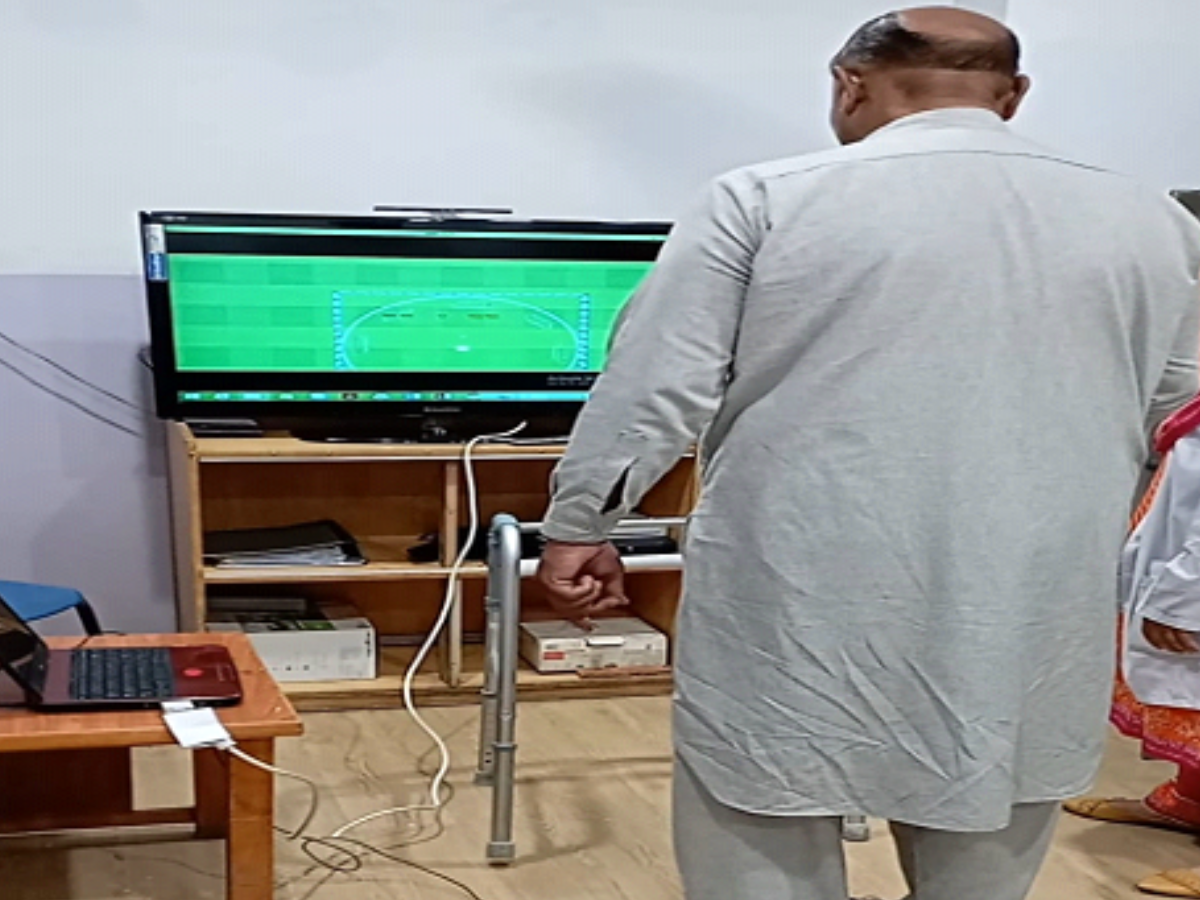
Exergame-Based Mat Training ProgramThe mat-based exercise system (Stampede, SHENNONA Co., Ltd) facilitates exercise training by using electronic light and sound effects to guide participants through various exercises, with intensity progressively increasing from moderate to high levels. This system facilitates customized movement programming tailored to specific training objectives, and its architectural diagram is presented in A. The training program is divided into 2 phases: the first phase focuses on fundamental movements, whereas the second phase introduces more advanced exercises. With progress, additional exercise equipment is incorporated, along with increased sets, duration, movement variations, and training intensity. Training sessions can be conducted in a simple progressive manner or a game-competitive format (B). Throughout the training, participants wore a heart rate monitor (ALATHEC Obeat1) that recorded their exercise intensity and heart rate fluctuations (B). Exercise intensity was indicated by lighting colors, corresponding to specific percentages of the maximum heart rate (HRmax) as follows: blue (0%-50% HRmax), cyan (50%-60% HRmax), green (60%-70% HRmax), yellow (70%-80% HRmax), orange (80%-90% HRmax), and red (>90% HRmax). However, the exercise intensity and frequency were adjusted based on participants’ adaptation. This study encompassed 5 different lighting modes, namely all light on, circle on, 4 corners, 2 lines, and diamond (). Each mode was paired with different training protocols and movement patterns, supplemented by training equipment, such as medicine balls, resistance bands, kettlebells, and balance pads. This combination enhanced engagement while simultaneously promoting functional fitness, including muscular strength, muscular endurance, aerobic capacity, flexibility, agility, balance, and core strength. Detailed training protocols are provided in . All participants achieved a 100% attendance rate, and adverse events were observed by qualified specialists. All training sessions were supervised and instructed by certified fitness instructors.
 Figure 1. Stampede exercise mat system. (A) A central router facilitates data transmission among a cloud server, user interface devices (such as smartphones), and an analysis unit. The system highlights seamless data flow, emphasizing connectivity, data processing, and user interaction. (B) Stampede exercise mats use lighting and sound effects to guide participants through exergame implementation in the National Taipei University of Nursing and Health Sciences I203 laboratory. In addition, the system can be integrated with other exercise equipment to enhance fitness benefits while incorporating elements of enjoyment and gamification.
Figure 1. Stampede exercise mat system. (A) A central router facilitates data transmission among a cloud server, user interface devices (such as smartphones), and an analysis unit. The system highlights seamless data flow, emphasizing connectivity, data processing, and user interaction. (B) Stampede exercise mats use lighting and sound effects to guide participants through exergame implementation in the National Taipei University of Nursing and Health Sciences I203 laboratory. In addition, the system can be integrated with other exercise equipment to enhance fitness benefits while incorporating elements of enjoyment and gamification.  Figure 2. Exergame-based mat training modes and intensity monitoring. (A) This study used 5 lighting modes (all lights on, circle on, 4 corners, 2 lines, and diamond) for designated training protocols or in combination with other exercise equipment. (B) Heart rate was continuously monitored throughout the program. Body Composition
Figure 2. Exergame-based mat training modes and intensity monitoring. (A) This study used 5 lighting modes (all lights on, circle on, 4 corners, 2 lines, and diamond) for designated training protocols or in combination with other exercise equipment. (B) Heart rate was continuously monitored throughout the program. Body CompositionInBody 270 (Biospace) was used as the body composition analyzer. It is a noninvasive bioelectrical impedance analysis device, which estimates body composition by transmitting a low-level electrical current through the body and measuring resistance. It provides accurate assessments of BMI, body fat percentage, obesity analysis, skeletal muscle mass, and visceral fat levels, serving as a comprehensive tool for evaluating body composition. The detailed procedures have been described previously [].
Senior Fitness TestIn older adults, various components of functional fitness were evaluated using standardized tests. Aerobic endurance was assessed through the 2-minute step test, whereas upper and lower limb muscular endurance were measured using the arm curl test and chair stand test, respectively. Lower limb flexibility was evaluated with the sit-and-reach test, and shoulder flexibility was assessed using the back-scratch test. In addition, static balance was measured using the one-leg standing test, and dynamic balance was evaluated using the 8-foot up-and-go test. Detailed procedures, devices, and manipulation have been described previously []. These senior functional tests are cost-effective and convenient for assessing functional fitness in older adults. They are suitable for independently living individuals aged 60-90 years and above, encompassing numerous fitness levels, ranging from frailty to high fitness []. All certified assessors, independent from the research team, conducted the Senior Fitness Assessments and AFAscan fitness assessment in a single-blind manner.
AFAscan Fitness AssessmentThe AFAscan leader facility was used to assess various components of physical fitness, including lower body explosiveness, core strength, flexibility, agility, balance, and endurance. It used gyroscopes (positioned on the chest and both thighs) and a force platform to precisely and objectively measure all physical performance parameters.
Lower Body ExplosivenessLower body explosiveness was evaluated using a countermovement jump with an arm swing. Participants jumped to the highest extent while attempting to land in the same position on the force mat from which they took off. During the airborne phase, they maintained full extension of their hip, knee, and ankle joints to prevent any additional flight time caused by leg bending. Flight time was recorded as the primary measurement reference.
Core StrengthCore strength was measured using the bent-knee sit-up exercise. Participants lay on their backs with their knees flexed and feet positioned 12 inches from their buttocks. To ensure stability, a partner could assist by holding their feet in place. Participants conducted curl-ups, raising their upper bodies to at least 35°, and completed the fullest possible repetitions within 60 seconds.
FlexibilityFlexibility was assessed using the standing toe touch exercise. Participants stood with their feet together, toes pointing forward on the force mat. They bent forward at the hips, attempting to touch their fingertips to that of their toes without bending their knees. They held the position for 3 seconds to allow for angle measurement, which served as the flexibility assessment outcome.
AgilityAgility was assessed using the quick feet test. Participants alternately raised their feet in rapid succession, taking the shortest possible steps. They tried completing the maximum number of repetitions within 15 seconds.
BalanceBalance was assessed using the single-leg stand test. Participants raised their preferred foot and placed it against the inner thigh of the standing leg. They maintained a steady center of gravity within the center of a designated circle. A higher score was achieved by remaining stable within the center for a longer duration, with a maximum assessment time of 30 seconds.
EnduranceEndurance was assessed using the high-knee test. Participants drove their right knee toward their chest and quickly returned it to the ground, continuously alternating with the opposite knee. Arm swinging was permitted to aid movement. Participants raised their knees to an indicated angle >50° and completed the maximum number of repetitions within 30 seconds.
QuestionnairesPhysical activity levels were measured using the IPAQ, which evaluates walking, moderate-intensity, and vigorous-intensity activities over the past 7 days. The IPAQ has shown good test-retest reliability (Spearman ρ=0.76-0.94) and acceptable internal consistency (Cronbach α=0.80), with evidence of concurrent validity when compared against accelerometer data [,]. The Taiwanese version of the IPAQ was used, specifically the long-form Taiwan Physical Activity Survey Questionnaire, which consists of 26 items encompassing four domains: work, household activities, transportation, and leisure activities [].
In addition, the Taiwanese version of the WHOQOL-BREF—a short version of the World Health Organization Quality of Life Assessment questionnaire—was used. This version consists of 28 items, encompassing 4 domains: physical health, psychological well-being, social relationships, and environmental factors. The WHOQOL-BREF has demonstrated acceptable internal consistency, with Cronbach α ranging from 0.66 to 0.84 across domains, and satisfactory construct validity when tested in different populations [,]. This shortened and adapted version serves as a valid alternative to the long-form WHOQOL questionnaire used in Taiwan [].
Eligibility CriteriaThe inclusion criteria were as follows: (1) older adults (aged 60‐80 years) with no musculoskeletal injuries in the past month and capable of participating in training activities, (2) completion of the Physical Activity Readiness Questionnaire (PAR-Q) and eligibility for moderate-intensity exercise intervention, and (3) ability to adhere to the exercise frequency required by the study and independently commute to the training site. The exclusion criteria were as follows: (1) individuals with musculoskeletal disorders, joint diseases, unstable cardiovascular conditions, or cognitive impairments, as well as those with psychiatric disorders based on questionnaire evaluation, and (2) individuals whose PAR-Q responses indicate potential risks or concerns.
Statistical AnalysesDescriptive statistics and chi-square tests were used to analyze the anthropometric and sociodemographic characteristics of all participants. The normality of all dependent variables was evaluated using Kolmogorov-Smirnov tests to ensure the appropriate selection of parametric and nonparametric analyses. To examine significant between- and within-group differences, nonparametric methods (Wilcoxon signed-rank test and Mann-Whitney U test) and parametric methods (mixed 2-way analysis of variance, unpaired 2-tailed t tests, and paired t tests) were applied. Two participants withdrew before completing posttest assessments and thus provided only baseline data. Because no postintervention outcome data were available for these individuals, no imputation was applied, and analyses were performed using complete cases. Consequently, a total of 15 participants in the experimental group and 15 participants in the control group were included in the final statistical analysis. All statistical analyses were performed using SPSS software (version 22; IBM Corp), with statistical significance set at P<.05. Effect sizes (d) were calculated as Cohen d and interpreted according to conventional benchmarks: small (0.2), medium (0.5), and large (0.8) []. The 95% CIs were reported alongside all effect size estimates to enhance interpretability.
Ethical ConsiderationsThis study was reviewed and approved by the Fu Jen Catholic University Institutional Review Board (IRB # C112161) per ethical guidelines for human research. Before participation, all participants were informed about the study procedures and precautions, and written informed consent was obtained. All acquired data will be analyzed and disseminated in deidentified format to ensure participant confidentiality. Study participants will receive individualized physical fitness assessment reports and monetary compensation consisting of US $32.77 (exchange rate: US $1=30.5 TWD) for transportation expenses. To ensure participant safety, all training sessions were supervised by qualified specialists, who continuously monitored for potential and unexpected adverse events. Any adverse event would have been documented immediately, managed with appropriate first aid, and referred for medical evaluation if necessary.
The experimental procedure is illustrated in . This study recruited 32 participants, with 16 allocated to each of the experimental and control groups. However, one participant from each group withdrew from the study because of personal reasons. Finally, 15 participants in both groups were analyzed for primary outcomes. The participants in the experimental group were paired and engaged in the training activities through alternating and cooperative interactions. Heart rate monitoring during the training indicated fluctuations characteristic of high-intensity interval training (). In addition, no significant differences were observed in sex, age, height, weight, systolic, diastolic pressure, and resting heart rate (t28=0.065‐1.121; all P>.05) before the intervention ().
 Figure 3. Study flow diagram. PAR-Q: Physical Activity Readiness Questionnaire. Table 2. Basal anthropometric characteristics.CharacteristicsControl (n=15)Experiment (n=15)Mean difference (95% CI)Effect size (Cohen d)Sex (male/female), n2/132/13——Age (years), mean (SD)67.7 (4.4)67.8 (3.9)0.13 (–2.96 to 3.22)0.03Height (cm), mean (SD)157.7 (3.5)157.8 (5.7)0.11 (–3.43 to 3.65)0.02Weight (kg), mean (SD)50.2 (9.4)55.4 (13.8)5.26 (–3.63 to 14.2)0.44Systolic pressure (mm Hg), mean (SD)121.6 (17)127.8 (15)6.13 (–6.17 to 18.4)0.37Diastolic pressure (mm Hg), mean (SD)75.4 (10)77.0 (9.2)1.60 (–5.47 to 8.67)0.17Resting heart rate (bpm), mean (SD)81.6 (11)85.4 (12)3.87 (–4.83 to 12.6)0.33
Figure 3. Study flow diagram. PAR-Q: Physical Activity Readiness Questionnaire. Table 2. Basal anthropometric characteristics.CharacteristicsControl (n=15)Experiment (n=15)Mean difference (95% CI)Effect size (Cohen d)Sex (male/female), n2/132/13——Age (years), mean (SD)67.7 (4.4)67.8 (3.9)0.13 (–2.96 to 3.22)0.03Height (cm), mean (SD)157.7 (3.5)157.8 (5.7)0.11 (–3.43 to 3.65)0.02Weight (kg), mean (SD)50.2 (9.4)55.4 (13.8)5.26 (–3.63 to 14.2)0.44Systolic pressure (mm Hg), mean (SD)121.6 (17)127.8 (15)6.13 (–6.17 to 18.4)0.37Diastolic pressure (mm Hg), mean (SD)75.4 (10)77.0 (9.2)1.60 (–5.47 to 8.67)0.17Resting heart rate (bpm), mean (SD)81.6 (11)85.4 (12)3.87 (–4.83 to 12.6)0.33aNot applicable.
Effects of the Exergame-Based Mat Program on Physical ActivityPre- and postintervention results of the Physical Activity Scale indicated a significant main effect of time on total physical activity levels (). After the intervention, activity levels significantly increased in the experimental group, with significant within-group differences. Therefore, the mat exercise program effectively enhanced overall physical activity in older adults. For vigorous physical activity, the main effect of time (F1,28=13.9; P=.001) and interaction effect (F1,28=11.9; P=.002) were observed. The experimental group demonstrated a significant within-group increase in total metabolic equivalents (MET) (t14=2.88; P=.01; mean difference [MD] 1266, 95% CI 325-2206; d=0.74) and vigorous activity (t14=7.37; P<.001; MD 950, 95% CI 674-1227; d=1.90), indicating that the intervention effectively promoted physical activity. In addition, after the intervention, the experimental group demonstrated significantly higher vigorous activity levels than the control group (t28=1.97; P=.04; MD 439, 95% CI 28-914; d=0.72), supporting the effectiveness of the exergame-based mat program. However, no significant main effects or interaction effects were observed for moderate-intensity activity, walking, or sedentary behavior (F1,28=0.583‐1.889; P>.05). Thus, the intervention exerted a relatively lower impact on moderate- and low-intensity physical activities.
Table 3. Effects of the exergame-based mat training program on physical activity levels in older adults: effect sizes and 95% CIs.Physical activity intensityControl (MET-min/week), mean (SD)Experiment (MET-min/week), mean (SD)Mean difference (95% CI)Effect size, Cohen dPrePostPrePostTotal MET2866 (1540)3328 (2045)2052 (1650)3318 (1440)–9.67 (–1332 to 1313)0.01Vigorous intensity789 (692)828 (762)317 (417)1267 (406),439 (28 to 914)0.72Moderate intensity752 (945)1252 (1029)560 (782)757 (620)–495 (–1131 to 141)0.58Walking1153 (862)1076 (715)1112 (817)1164 (732)85.8 (–456 to 627)0.12Sitting (work)297 (139)211 (119)206 (158)230 (182)19.3 (–96 to 134)0.13Sitting (holiday)277 (134)239 (111)278 (157)282 (144)43.3 (−52 to 140)0.34aMET: metabolic equivalents.
bMET·min·wk⁻¹
cIndicates significant within-group differences.
dIndicates significant between-group differences.
Effects of Exergame-Based Mat Program on Quality of LifeThe WHOQOL-BREF assessment evaluated overall health and health satisfaction, along with four domains: physical health, psychological health, social relationships, and environment (). Concerning physical health, the experimental group demonstrated significant differences both within (P=.02) and between (P=.01; Hodges-Lehmann median difference=1.2; 95% CI 0.6-2.3; r=0.53) groups. Specifically, significant within-group improvements were observed in pain and discomfort (P=.02), dependence on medical aids (P=.002), mobility (P=.008), and daily activities (P=.002). In addition, daily activities (P=.002) and work capacity (P=.006) showed a significant between-group difference in the experimental group, compared with the control group. Concerning psychological health, the experimental group exhibited a significantly higher overall score than the control group (P=.02; Hodges-Lehmann median difference=2.7, 95% CI 1.3-4; r=0.52). Significant between-group differences were observed in self-esteem (P=.02) and negative feelings (P=.001), with negative feelings showing significant differences within (P=.02).
Table 4. Effects of the exergame-based mat training program on quality of life in older adults with effect sizes and 95% CIs.DimensionsControl, mean (SD)Experiment, mean (SD)Hodges-Lehmann, median difference (95% CI)Effect size (r)PrePostPrePostOverall health3.4 (0.6)3.3 (0.5)3.6 (0.5)4 (0.5)1 (0 to 2)0.64Health satisfaction3.3 (0.7)3.0 (0.6)3.4 (0.6)3.7 (0.5)1 (0 to 2)0.65DomainsPhysical health13.3 (1.3)14.3 (1.8)13.5 (0.9)16.1 (1.6),1.2 (0.6 to 2.3)0.53Pain and discomfort3.3 (0.5)3.5 (0.9)3.0 (0.5)4.1 (0.8)1 (0 to 2)0.35Dependence on medical substance and medical aids3.3 (0.9)3.3 (0.8)3.3 (0.5)4.1 (0.6)0 (–1 to 1)0.17Energy and fatigue3.5 (0.5)3.3 (0.6)3.4 (0.5)3.6 (0.5)0 (1 to 1)0.29Mobility3.5 (0.6)3.9 (0.5)3.5 (0.5)4.2 (0.7)0 (–1 to 1)0.28Sleep and rest3.2 (1.1)3.1 (0.9)3.5 (0.7)3.3 (0.8)0 (–1 to 1)0.07Activities and daily living3.3 (0.6)3.5 (0.6)3.3 (0.5)4.3 (0.5),1 (0 to 2)0.56Work capacity3.9 (0.5)3.5 (0.5)4.1 (0.7)4.1 (0.5)1 (0 to 2)0.50Psychological health13.8 (1.9)13.4 (2.0)14.3 (1.7)15.3 (1.6)2.7 (1.3 to 4)0.52Positive feeling3.5(0.6)3.3 (0.6)3.5 (0.6)3.7 (0.7)1 (0 to 2)0.34Spirituality, religion, and personal beliefs3.7 (0.7)3.7 (0.6)3.7 (0.9)3.8 (0.7)0 (–1 to 1)0.14Thinking, learning, memory, and concentration3.5 (0.7)3.1 (0.7)3.8 (0.7)3.5 (0.5)0 (–1 to 1)0.30Bodily image and appearance3.7 (0.6)3.5 (0.6)3.9 (0.7)4 (0.8)1 (0 to 2)0.31Self-esteem3.9 (0.6)3.5 (0.6)3.7 (0.6)4.1 (0.5)1 (0 to 2)0.42Negative feelings3.3 (0.6)3.1 (0.7)3.4 (0.9)3.9 (0.5),1 (0 to 2)0.64Social relationship13.4 (2.1)12.8 (1.9)14.4 (2.6)14.5 (1.5)2 (1 to 3)0.50Personal relationship3.9 (0.6)3.2 (0.6)3.9 (0.9)3.7 (0.6)1 (0 to 2)0.38Sexual activity3.2 (1.1)3.1 (0.8)3.4 (0.7)3.2 (1.1)0 (–1 to 1)0.23Social support3.7 (0.6)3.3 (0.6)3.6 (0.7)3.9 (0.5)1 (0 to 2)0.56Being respected3.7 (0.6)3.3 (0.5)3.8 (1.1)3.7 (0.7)1 (0 to 2)0.31Environment15.1 (1.7)14.6 (1.8)15.7 (1.7)15.8 (1.4)1.8 (0.9 to 2.7)0.39Freedom, physical safety, and security3.7 (0.8)3.6 (0.6)4.1 (0.6)4 (0.5)0 (–1 to 1)0.30Physical environment3.6 (0.8)3.4 (0.5)3.6 (1.0)3.4 (0.6)0 (–1 to 1)0.06Financial resource3.8 (0.7)3.6 (0.7)4.2 (0.7)3.8 (0.9)1 (0 to 2)0.19Opportunities for acquiring new information and skills3.9 (0.6)3.9 (0.6)4.0 (0.5)4.2 (0.6)1 (0 to 2)0.26Participation and opportunities for recreation/leisure activities3.8 (0.7)3.7 (0.5)4.2 (0.8)3.8 (0.7)1 (0 to 2)0.15Home environment3.7 (1.1)3.8 (0.6)3.9 (0.7)3.9 (0.5)1 (0 to 2)0.44Health and social care: accessibility and quality4.3 (0.7)4.3 (0.5)4.3 (0.5)4.2 (0.5)1 (0 to 2)0.40Transport4.3 (0.6)4.3 (0.5)4.3 (0.5)4.3 (0.6)1 (0 to 2)0.40Eating4.1 (0.6)3.8 (0.7)3.9 (0.6)4.0 (0.8)1 (0 to 2)0.15aIndicates significant between-group differences.
bRaw domain scores for the World Health Organization Quality of Life Brief Version are transformed to a 4 to 20 score according to guidelines (Total score of the participant in a specific domain×4) divided by (Total number of items in the domain).
cIndicates significant within-group differences.
Concerning social relationships, the experimental group demonstrated significantly higher overall scores than the control group (P=.02; Hodges-Lehmann median difference 2, 95% CI 1-3; r=0.50). Furthermore, the experimental group exhibited significantly higher scores in social support than the control group (P=.003). In contrast, regarding the environment, no significant within- or between-group differences were observed in overall scores or individual items, indicating that the intervention did not substantially affect this aspect of quality of life.
Effects of Exergame-Based Mat Program on Senior Fitnesssummarizes the results for systolic blood pressure, diastolic blood pressure, and heart rate. No significant interaction effects were observed between group and time (F1,28=0.583‐1.889; all P>.05). In addition, no significant main effect of group was observed (F1,28=1.505‐2.181; all P>.05), except for a significant main effect of time on diastolic blood pressure (F1,28=4.350; P=.04). In the control group, systolic blood pressure and heart rate did not change, whereas diastolic blood pressure significantly reduced after the intervention. In the experimental group, systolic blood pressure, diastolic blood pressure, and heart rate showed no significant between- or within-group differences.
Table 5. Effects of the exergame-based mat training program on Senior Fitness Test outcomes in older adults with effect sizes and 95% CIs.VariablesControl, mean (SD)Experiment, mean (SD)Mean difference (95% CI)Effect size (Cohen d)PrePostGain scorePrePostGain scoreSystolic pressure (mm Hg)121.6 (17)116.6 (17)–5.1 (15)127.8 (15)126.2 (16)–1.6 (8.1)9.60 (–2.83 to 22)0.58Diastolic pressure (mm Hg)75.4 (10)70.6 (8.4)–4.9 (6.7)77 (9.2)76.1 (7.6)–1 (8.5)5.47 (–0.54 to 11.5)0.68Resting heart rate (bpm)81.6 (11)78.1 (6.3)–3.5 (11)85.4 (12)85.1 (13.5)–0.4 (7.6)7 (–0.89 to 14.9)0.66Arm curl test (times)17.7 (5)17.4 (5.3)–0.3 (2.9)17.7 (2.9)22.7 (4.6),5.1 (3.9)5.33 (1.59 to 9.07)1.06Chair stand test (times)23.7 (5.7)22 (4.7)–1.6 (4.1)23.6 (4.5)26.8 (4.8),3.2 (3.8)4.73 (1.15 to 8.32)0.98Chair sit-and-reach (cm)7.8 (4.4)5.8 (6.8)–2 (4.1)7.9 (6)12.3 (5.5),4.4 (3.6)6.47 (1.82 to 11.1)1.04Back-scratch test (cm)6.6 (4.2)6.6 (5.1)–0.1 (2.6)5.8 (3.1)6.4 (4.2)0.5 (3.5)–0.18 (–3.67 to 3.31)0.04One-leg standing test (s)27.8 (5.5)26.7 (7.2)–1.1 (3.7)26 (7.3)28.7 (5.2)2.7 (5.2)2 (–2.67 to 6.67)0.328-foot up-and-go test (s)4.3 (0.6)4.4 (0.6)0.2 (0.3)4.3 (0.5)3.7 (1.1)–0.6 (1.1)–0.72 (–1.36 to –0.07)0.842-minute step test (times)109 (11)109 (12)– 0.3 (7.7)107 (8.8)119 (13),12 (10)9.73 (0.37 to 19.1)0.78aIndicates significant within-group differences.
bIndicates significant between-group differences.
For muscular endurance of both upper and lower limbs, a significant interaction effect was observed between time and group (F1,28=18.1, P<.001; F1,28=10.91, P=.003, respectively). Specifically, upper limb muscular endurance in the experimental group was significantly higher in the posttest compared with the pretest (t14=4.92; P<.001; MD 5.07, 95% CI 2.80-7.27; d=1.27), and significantly higher compared with the control group (t28=2.92; P=.007; MD 5.33, 95% CI 1.59-9.07; d=1.06). Moreover, the gain score for upper limb endurance was significantly higher in the experimental group than in the control group (t28=4.26; P<.001; MD 5.4, 95% CI 2.80-7.99; d=1.55). Similarly, lower limb muscular endurance was significantly higher in the experimental group after the intervention compared with before the intervention (t14=3.24; P=.006; MD 3.2, 95% CI 1.08-5.31; d=1.55) and the control group (postintervention values; t28=2.70; P=.01; MD 4.73, 95% CI 1.15-8.32; d=0.98). The gain score for lower limb endurance was significantly higher in the experimental group than in the control group (t28=3.31; P=.003; MD 4.80, 95% CI 1.83-7.77; d=1.21).
No significant interaction effect was observed between time and group for upper limb flexibility (F1,28=0.284; P=.59). No significant between- or within-group differences were observed for upper limb flexibility after the intervention. However, a significant interaction effect was observed for lower limb flexibility (F1,28=20.71; P<.001). However, lower limb flexibility in the experimental group was significantly higher after the intervention than before the intervention (t14=4.74; P<.001; MD 4.41, 95% CI 2.41-6.40; d=1.04). Postintervention values were significantly higher than those in the control group (t28=2.85, P=.008, MD 6.47, 95% CI 1.82-11.1; d=1.04). In addition, the gain score for lower limb flexibility was significantly higher in the experimental group than in the control group (t28=4.55; P<.001; MD 6.45, 95% CI 3.54-9.36; d=1.66).
Regarding balance performance, no significant interaction effect was observed for static balance between time and group (F1,28=1.308; P=.29), with no significant between- or within-group differences. Nonetheless, a significant interaction effect was observed for dynamic balance (F1,28=6.646; P=.02). Despite no significant within-group difference in the experimental group before and after the intervention, the postintervention time was significantly lower than that in the control group (t28=−2.29; P=.03; MD -0.72, 95% CI −1.36 to −.07; d=0.84). Furthermore, the gain score for dynamic balance was significantly lower in the experimental group than in the control group (t28=−2.58; P=.02; MD −0.77, 95% CI −1.38 to −0.16; d=0.94).
For aerobic endurance, a significant interaction effect was observed between time and group (F1,28=14.027; P=.001). In the experimental group, postintervention aerobic endurance was significantly higher than preintervention endurance (t14=4.58; P<.001; MD 12, 95% CI 6.38-17.6; d=1.18). Moreover, postintervention values were significantly higher than those in the control group (t28=2.13; P=.04; MD 9.73, 95% CI 0.37-19.1; d=0.78). In addition, the gain score for aerobic endurance was significantly higher in the experimental group than in the control group (t28=3.75; P=.001; MD 12.3, 95% CI 5.59-19.1; d=1.66).
Effects of Exergame-Based Mat Program on AFAscan Fitness AssessmentNo significant interaction effect was observed for explosiveness, along with no significant between- or within-group differences (F1,28=0.169; P=.68) (). For core strength, a significant interaction effect was observed between time and group (F1,28=14.027; P=.001). In the experimental group, postintervention core strength was significantly higher than preintervention core strength (t14=3.77; P=.002; MD 8.14, 95% CI 3.47-12.8; d=1). Moreover, postintervention values were significantly higher than those in the control group (t28=5.18; P<.001; MD 13.1, 95% CI 7.90-18.2; d=1.89). In addition, the gain score for core strength was significantly higher in the experimental group than in the control group (t28=2.49; P=.02; MD 6.69, 95% CI 1.15-12.2; d=1.04).
Comments (0)