
Remember me



Studies have shown that oral glucose intake elicits a more robust insulin secretion response compared to intravenous glucose delivery, despite identical glucose concentrations [3]. This phenomenon, referred to as the “incretin effect,” was subsequently attributed to gastrointestinal and endocrine factors. The first factor identified was gastric inhibitory polypeptide (GIP), which was thought to increase glucose-stimulated insulin secretion. However, it was found that the incretin effect remained preserved even after the removal of GIP in experiments. Glucagon-like peptide (GLP) type 1 was subsequently identified as another active incretin [4].
In the 1980 s, researchers identified GLP-1 in the gut and discovered its role in enhancing insulin release while simultaneously suppressing glucagon secretion [5]. In 2005, the first GLP-1 agonist, exenatide, was approved for the management of Type 2 diabetes mellitus (T2DM) [6]. In 2009, another GLP-1 agonist, liraglutide, reached the market, followed by the establishment of more GLP-1 agonists in diabetes management [7].
Gastrointestinal FactorsOver the past century, many observations have been made supporting the presence of gastrointestinal (GI) substances that might increase insulin secretion. In 1906, Moore et al. suggested that the duodenal mucosa could potentially release a hormone that acts as an excitant for internal pancreatic secretions [8].
In 1959, the innovation of radioimmunoassay by Berson and Yalow helped quantify insulin secretion in humans [9]. Experiments undertaken in 1964 showed more insulin secretion with oral versus intravenous (IV) glucose administration despite identical glucose concentrations, an effect coined the “Incretin effect” [10].
In 1973, John Brown discovered the glucose-dependent insulinotropic polypeptide (GIP) employing peptide purification and protein sequencing, it was shown to have an incretin effect, increasing Insulin release triggered by glucose intake after oral administration [11]. However, preservation of the incretin effect after GIP removal has been demonstrated in animal GIP immunoneutralization experiments [12]. Studies in humans confirmed the lack of GIP effect on insulin secretion in patients with all DM types [13].
During the early 1970 s, the introduction of recombinant DNA (rDNA) technology enabled more precise protein amino acid sequencing by analyzing the nucleotide sequences of cloned recombinant cyclic DNA (cDNA) derived from messenger RNA (mRNA) [14]. Using this new technology, Habener et al. discovered the amino acid and gene sequences of proglucagon from anglerfish, which contained a stretch of amino acids resembling glucagon [14, 15]. Shortly thereafter, Graeme Bell et al. published the complete structure of mammalian and human proglucagon, which contained two glucagon-like structures called GLP-1 and GLP-2 [16]. However, there was uncertainty regarding the identification of the bioactive isoforms of Glucagon-like peptide 1 (GLP-1) that possessed a true insulinotropic effect.
Svetlana Mojsov first predicted the presence of GLP-1 isoforms [17]. Her subsequent work with Daniel Drucker using radioimmunoassay and chromatography identified a unique pattern of proglucagon-derived peptides in the gastrointestinal tract and pancreas, including more immunoreactive GLP-1 peptides in GI extracts [18]. Subsequent experiments showed that the active forms of GLP-1 were GLP-1(7–36 amide) and GLP-1(7–37) isoforms, increasing cAMP levels, insulin mRNA transcripts, promoting insulin secretion in the pancreases of pigs and rats, respectively [19]. In 1993, Nauck et al. showed that fasting glucose levels were completely normalized by GLP-1 infusion in T2DM patients [20]. This observation led to a study where GLP-1 was given to obese patients with T2DM and showed improved glycemic control with no side effects, establishing a proof-of-concept for GLP-1 agonists, which over time led to their use in the treatment of T2DM patients [21].
GLP-1 receptor agonists have been administered as subcutaneous injections. To overcome a potential barrier among patients favoring an alternative, oral formulations were developed. In 2019, oral semaglutide received approval as the first oral GLP-1 receptor agonist [22]. To improve gastrointestinal absorption, a carrier molecule of sodium N-(8-[2-hydroxybenzoyl] amino) caprylate (SNAC) was added to its chemical structure to overcome the challenges of peptide degradation and poor membrane permeability [23].
Looking ahead, the future of GLP-1RA delivery is poised to include oral, ultralong-acting injectables, implantable pumps, smart electronic devices, and noninvasive systems like sublingual or transdermal routes. These innovations aim to enhance bioavailability, reduce dosing frequency, and improve patient compliance [24].
A Pivotal Contribution from Regulatory Agencies To Relevant Clinical ObservationsThe requirements to assess the safety of new diabetes medications, including GLP-1R agonists, set forth by The United States Food and Drug Administration (FDA) were specified in the December 2008 guidance document titled “Guidance for Industry: Diabetes Mellitus — Evaluating Cardiovascular Risk in New Antidiabetic Therapies to Treat Type 2 Diabetes.” A draft of this document had been issued in March 2008 and the final document followed recommendations from the Endocrinologic and Metabolic Drugs Advisory Committee that convened on July 1 and 2, 2008 [25]. This guidance advised that companies should show that the risk of cardiovascular events in T2DM patients didn’t increase with the use of their new antidiabetic therapies (drugs or therapeutic biologics), a proactive response to concerns about the cardiovascular safety of some diabetes medications developed previously (https://www.fda.gov/regulatory-information/search-fda-guidance-documents/type-2-diabetes-mellitus-evaluating-safety-new-drugs-improving-glycemic-control-guidance-industry; accessed August 25, 2025). Similar recommendations were made by the European Medicines Agency (EMA) that required including major adverse cardiovascular events (MACE) as a primary endpoint (https://www.ema.europa.eu/en/clinical-investigation-medicinal-products-treatment-or-prevention-diabetes-mellitus-scientific-guideline).
These regulatory requirements led to the discovery of cardiovascular benefits in GLP-1R agonists, demonstrating the importance of due diligence and proactive safety monitoring. The agencies not only ensured safety but also facilitated the expansion of therapeutic indications for GLP-1R agonists, including obesity and cardiovascular risk reduction.
The cardiac benefits of GLP-1 agonists were not anticipated before outcome studies were performed for several reasons: (1) Historical Precedent-past experiences with other diabetes medications that unexpectedly had adverse cardiovascular effects made it less likely for researchers and clinicians to anticipate potential cardiovascular benefits without concrete evidence from large-scale trials; (2) Primary Focus on Glucose Control- GLP-1R agonists were developed to improve glycemic control in T2DM patients. The primary goals were to lower blood sugar levels and reduce the risk of diabetes-related complications; (3) Lack of Early Indicators- prior to the cardiovascular outcomes trials (CVOTs), there was no strong evidence or clear biological indicators suggesting that this class of drug would have a direct effect on cardiovascular health; and (4) Complexity of Cardiovascular Disease- cardiovascular disease is multifactorial and complex. It was not clear how a drug that primarily affects glucose metabolism might directly impact the occurrence of cardiovascular events.
The FDA released an updated guidance document for industry in March 2020 that focused on the safety of drugs for chronic use to improve glycemic control in T2DM patients ((https://www.fda.gov/regulatory-information/search-fda-guidance-documents/type-2-diabetes-mellitus-evaluating-safety-new-drugs-improving-glycemic-control-guidance-industry 2020 fda.gov; accessed August 25, 2025). An emphasis was placed on post-marketing surveillance informed by pre-marketing safety signals and on comorbid conditions that are common in T2DM patients, including: cardiovascular disease, chronic kidney disease, and older age.
The guidance document recommended that clinical trials include substantial representation of these populations to better reflect real-world use. Specifically, it called for safety data from at least 500 patients with stage 3 or 4 CKD, 600 with established CVD, and 600 aged over 65. This broadened inclusion criteria allowed for a more comprehensive understanding of drug effects in high-risk groups and supported the expansion of GLP-1R agonist indications beyond glycemic control to include cardiovascular and renal benefits.
The guidance emphasized post-marketing surveillance informed by pre-marketing safety signals, moving away from a rigid “one-size-fits-all” model. This flexibility enabled regulators to tailor safety monitoring based on actual risk profiles observed during drug development, facilitating the approval of drugs like GLP-1R agonists for broader therapeutic use, including in non-diabetic populations with Cardiovascular-Kidney-Metabolic (CKM) Syndrome.
In broader terms, the guidance exemplified how regulatory science can catalyze translational research, uncover unanticipated benefits, and accelerate innovation across therapeutic domains.
Mechanisms of Action and BenefitBiological, Physiological, and Molecular ConsiderationsGlucagon-like peptide 1 (GLP-1) is primarily secreted by enteroendocrine L-cells in the intestine, pancreatic α-cells, and the central nervous system (CNS) [26]. It is an incretin peptide hormone that participates in insulin secretion, contributing to bioenergetic pathways of cell survival [27]. After food intake, GLP-1 is rapidly released, enhancing insulin secretion in response to rising glucose levels [27].
GLP-1 receptor (GLP-1R) is class B of the G protein-coupled receptor (GPCR) and is primarily found in the CNS and pancreas. While its expression is most concentrated in these areas, it is also present in the lungs, heart, kidneys, digestive system, liver, skeletal muscles, and peripheral nervous system to a lesser extent [27, 28] (Fig. 1).
Fig. 1
The multiple sites of Glucagon-like Peptide (GLP)−1 expression and their resulting biological and physiological effects (from Pharmaceuticals 2023; 16: 836)
Once synthesized in by the ribosomes in the rough endoplasmic reticulum (RER), GLP-1R gets targeted to the smooth endoplasmic reticulum (SER) by a signal peptide located at the N-terminus of the receptor [29]. Cleavage of this signal peptide is crucial for GLP-1R expression on the cell surface; if cleavage is blocked, the receptor remains in the SER. Within its N-terminal domain, GLP-1R contains six conserved cysteine residues that form specific disulfide bonds between Cys46-Cys71, Cys62-Cys104, and Cys85-Cys126 [30]. Additionally, residues Asp67, Trp72, Pro86, Arg102, Gly108, and Trp110 are highly conserved across class B GPCRs, with Trp72 and Trp110 playing a vital role in agonist binding [29].
Once bound to GLP-1R, GLP-1 initiates a cascade of events, including the activation of membrane-bound adenylyl cyclase (AC) leading to cyclic adenosine monophosphate (cAMP) synthesis. cAMP formation initiates several downstream signaling pathways by activating downstream effector proteins such as protein kinase A (PKA) and exchange protein (Epac) activated by cAMP [31, 32].
GLP-1R GeneGLP-1R gene encodes the glucagon-like peptide 1 receptor, a protein essential for regulating glucose metabolism and promoting insulin secretion. It’s a 7-transmembrane protein that functions as a receptor for the GLP-1 hormone. GLP-1R gene expression has been demonstrated in many organs and organ systems, including the heart and cardiovascular system [30].
Transcription events related to the GLP-1R gene involve its activation by GLP-1 or its analogs, initiating a series of intracellular reactions. These reactions include increasing cAMP and intracellular calcium, activation of protein kinase A, and induction of gene transcription [33]. Furthermore, GLP-1R can also become internalized in response to GLP-1 and its analogs, indicating a complex regulatory mechanism that affects gene expression and protein activity [32].
Evolutionary BiologyUpon nutrient ingestion enteroendocrine L-cells secrete GLP-1, which has a crucial role in glucose metabolism regulation via enhancing insulin secretion and inhibiting glucagon release. The evolutionary advantage of this system is to ensure efficient nutrient utilization and energy storage, which are critical for survival during periods of food scarcity [34, 35].
The cardiovascular effects of GLP-1 can be seen as an extension of its role in maintaining metabolic homeostasis. By improving cardiovascular function, GLP-1 helps to ensure that nutrients and oxygen are efficiently delivered to tissues, which is essential for overall metabolic health [36].
EmbryologyThe biological and physiological interface between the gastrointestinal (GI) tract and the cardiovascular system can be explained from an embryological perspective by examining the co-development of these systems during organogenesis.
During embryogenesis, the heart and the GI tract develop in proximity and share common signaling pathways and structural components. The heart originates from the mesoderm, while the GI tract arises from the endoderm. The interaction between these germ layers is crucial for the proper development of both systems.
Research has shown that the endoderm has a significant role in heart morphogenesis. For example, the endoderm provides essential paracrine signals that influence cardiac specification and differentiation. This is evident in the co-development of heart and digestive system tissues within human induced pluripotent stem cell (iPSC)-derived organoids, where the presence of endodermal tissue promotes the maturation of cardiac tissues [37].
In addition, the serosal mesothelium, which covers the gut, is a major source of gut vasculature smooth muscle cells. This mesothelium undergoes epithelial-mesenchymal transition (EMT) and plays a role vascular smooth muscle cells development, highlighting a conserved mechanism in blood vessel development for coelomic organs, including the heart and gut [38].
During heart tube assembly, the endoderm mechanical role is critical as it contracts, pulling the heart fields towards the midline to facilitate heart tube formation. This mechanical interaction underscores the importance of the endoderm in guiding the morphogenesis of the heart [39].
Gastrointestinal- Cardiovascular System SignalingThe gut-heart axis involves bidirectional communication where gut microbiota and their metabolites, such as short-chain fatty acids (SCFAs) and trimethylamine-N-oxide (TMAO), influence cardiovascular health. SCFAs have protective cardiovascular effects, while TMAO and lipopolysaccharides (LPS) from gut dysbiosis exacerbate cardiovascular diseases by promoting inflammation and endothelial dysfunction [40].
Vasoactive Intestinal Peptide (VIP), another gut-derived peptide, acts as a potent vasodilator and has positive inotropic effects on the heart. It increases coronary blood flow and reduces vascular resistance, contributing to improved cardiac function and protection against ischemic injury [41].
These interactions highlight the complex and integrated role of gut-derived peptides in modulating cardiovascular function, emphasizing the therapeutic potential of targeting these pathways in cardiovascular diseases as captured below under gaps and new areas of investigation.
Glucagon-Like Peptide-1 (GLP-1) and its Cardiovascular EffectsOver the past thirty years, researchers have made significant strides in understanding the gut-derived hormones impact on cardiovascular health. Among these hormones, GLP-1 has emerged as a pivotal role in cardiovascular disease and health.
GLP-1R agonists exert their cardiovascular effects through multiple pathways.
Positive Inotropic and Chronotropic EffectsGLP-1 exerts positive inotropic and chronotropic effects on the heart. By enhancing myocardial contractility, GLP-1 contributes to efficient cardiac function [42].
Preserve Left Ventricular Structure and FunctionGLP-1 maintains left ventricular integrity through both direct and indirect mechanisms. It contributes to cardiac functional and structural well-being. These effects particularly are relevant in preventing adverse remodeling and heart failure progression [43].
Pro-Survival and Energy UtilizationGLP-1 activates pro-survival kinases within cardiac cells. These kinases promote cell survival, potentially protecting against ischemic injury and oxidative stress. Furthermore, GLP-1 enhances energy utilization, optimizing cardiac metabolism [44].
Immune Modulating EffectsInduced human regulatory T cells (iTregs) express a functional GLP-1R, which increases intracellular cAMP levels upon stimulation with a GLP-1R agonist. This suggests that GLP-1R signaling in iTregs may mediate GLP-1R agonists anti-inflammatory effects [45]. A subset of CD8 T cells also express GLP-1R when exhausted. These GLP-1R-positive CD8 T cells has a role in the alloimmune response, and their signaling through GLP-1R acts as a negative costimulatory mechanism. This signaling can prolong allograft survival and mitigate alloimmune responses [46].
Proinflammatory cytokine expression in the myocardium has been shown to be reduced by GLP-1R agonists, which directly protects the heart against oxidative stress and inflammation. These combined effects on immune cells and direct myocardial protection underscore the multifaceted cardioprotective benefits of GLP-1R agonists [47].
Inflammation Attenuating EffectsEvidence suggests that inflammation in organs such as the liver, kidneys, and heart can be reduced by GLP-1R agonists [48]. In addition, by minimizing inflammation and preventing apoptosis they have a cellular protective role in the nervous and cardiovascular systems [49]. GLP-1R agonists regulate various molecular pro-inflammatory mediators, including oxidative stress, cytokine production, immune cell recruitment, glucotoxicity, and lipotoxicity ([50]). Employing preclinical, ex vivo, in vivo, and in vitro model systems investigators determined that GLP-1 agonists exert anti-inflammatory and immune modulating effects through their effects on macrophages (reduced interleukin [IL] 1β, IL-6, tumor necrosis factor [TNF]α, and C-X-C motif chemokine ligand [CXCL]), T and B lymphocytes (reduced cluster of differentiation [CD] 4 cells), monocytes (increased IL-10), mononuclear cells (decreased monocyte chemoattractant protein [MCP]−1, cell death protein [PD],, CD4 and CD8 T cells) [51,52,53,54,55].
Shiraki and colleagues determined that GLP-1 agonists anti-inflammatory effect were particularly robust on vascular endothelial cells [56]. GLP-1 agonists has protective effects against inflammation and oxidative stress on human endothelial cells, including those injured by inflammatory mediators like tumor necrosis factor (TNF)-α [57]. The inhibition of protein kinase C (PKC), NADPH oxidase, and NF-ҡB signaling exhibited anti-oxidative and anti-inflammatory effects in endothelial cells, accompanied by the upregulation of protective anti-oxidative enzymes [57]. Favorable effects were also demonstrated by Krasner and colleagues [58].
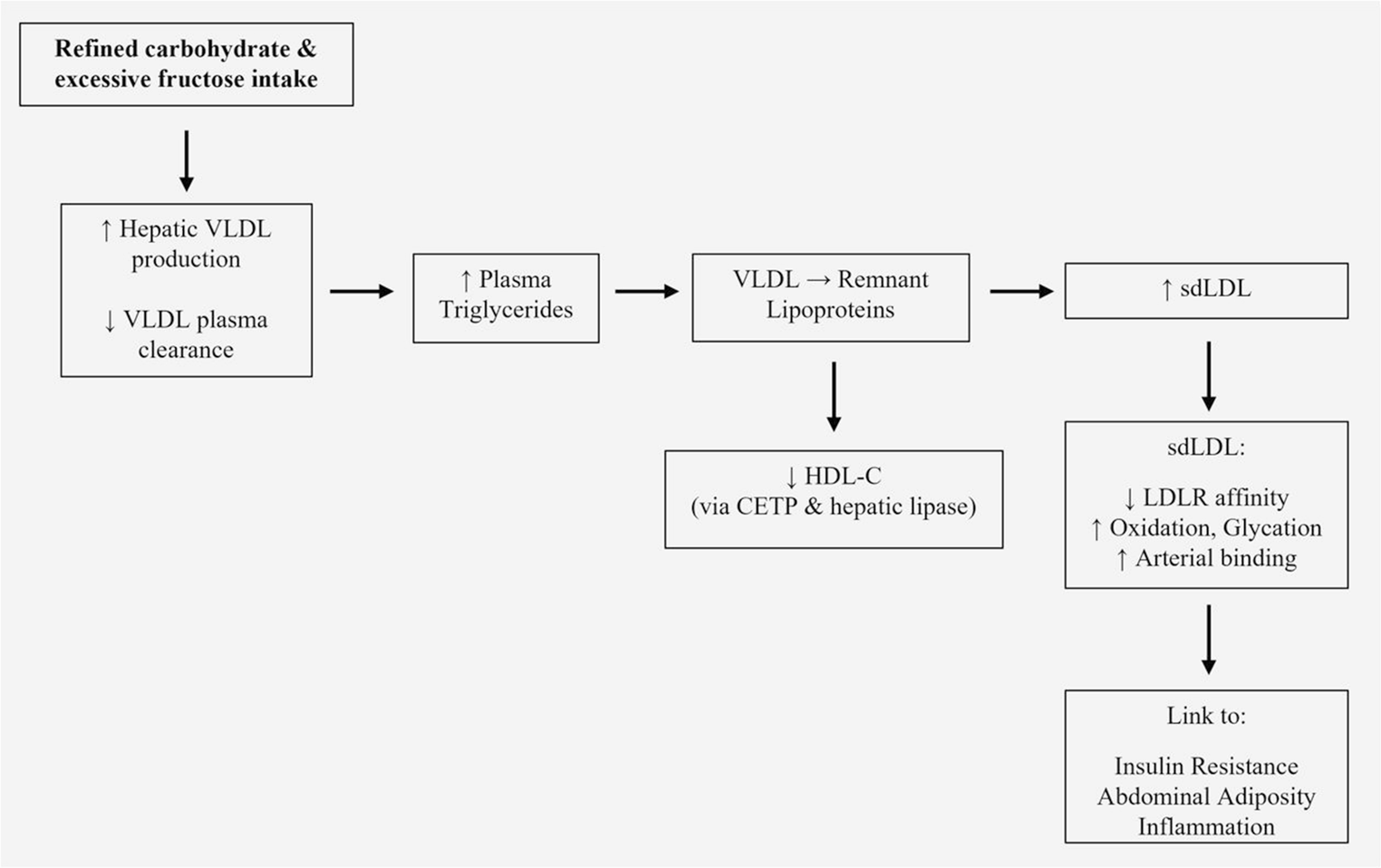
Anti-atherosclerosis EffectsAtherosclerosis, a chronic inflammatory disorder of the arterial wall, involves several key contributors to its initiation and progression that can be favorably altered or attenuated by GLP-1 agonists. Low density lipoprotein (LDL) cholesterol (C) and oxidized (ox) LDL are involved in atherogenesis, including the initial stage of endothelial cell injury and inflammation. GLP-1 agonists reduce LDL-C and ameliorate ox-LDL’s proinflammatory injurious effects on vascular endothelial cells that include monocyte binding [59]. Yue and colleagues showed that the GLP-1 agonist, liraglutide, reduced the transcriptional factor KLF2 and the rescued ox-LDL induced reduction of mitogen-activated protein kinase (MAPK) kinase extracellular signal regulated kinase 5 (ERK5) phosphorylation, and blockage of ERK5 activity on KLF2 expression [60]. Liraglutide also reduced endothelial tight junction protein barriers, ameliorated ox-LDL induced endothelial monolayer permeability, and inhibited ox-LDL induced expression of vascular adhesion molecules (E-selectin and vascular cell adhesion molecule- 1), preventing ox-LDL induced monocyte adhesion to endothelial cells [57].
GLP-1R are present in human coronary artery endothelial cells [61]. There is interest in GLP-1 agonists and their ability to either reduce atherosclerotic plaque burden or the potential for plaque disruption- recognized as a proximate cause of arterial thrombotic events. There are supportive clinical trials in T2DM patients of GLP-1 agonist mediated reduction in plaque burden, size and composition [62].
Despite a growing body of work, the precise mechanism(s) whereby GLP-1R agonists achieve anti-atherogenic effects is an area of much needed investigation.
Vasodilatory EffectsGLP-1 agonists exert vasodilatory properties in several vascular beds, ranging from the aorta to the coronary, mesenteric and renal arteries. The mechanism(s) represents a combination of direct and indirect effects on smooth muscle and endothelial cells. Selley and colleagues reported that GLP-1 associated vasodilation was mediated through the glucagon receptor [63]. Koska et al. found that increased postprandial endothelial function (EF) was independent of reductions in plasma glucose and triglycerides. The GLP-1 agonist, exenatide, increased fasting EF via endothelial nitric oxide (NO) synthase (eNOS) activation, nitric oxide (NO) production in endothelial cells, induced dose-dependent vasorelaxation, and reduced high-glucose or lipid-induced endothelial dysfunction in arterioles ex vivo [64].
GLP-1R agonists effect(s) on vascular smooth muscle cells are equally important to those on endothelial cells with several favorable responses being reported, including enhanced differentiation, attenuated response to reactive oxygen species, reduced vascular remodeling through improved mitochondrial activity and dynamics, and the prevention of aberrant migration [65].
MicrocirculationAnimal studies suggest that GLP-1R agonists enhance microvascular function and myocardial perfusion. Sukumaran and colleagues treated Zucker lean and obese rates with either vehicle or the GLP-1 agonist liraglutide (LIRA) for 8 weeks [66]. Synchrotron contrast microangiography was employed to assess coronary arterial vessel function (internal diameter: 50–350) in vivo in anesthetized rats. Myocardial gene and protein expression levels of vasoactive factors, inflammatory markers, oxidative stress and remodeling indicators were analyzed using real-time PCR and Western blotting. Compared to vehicle-treated rats, those receiving LIRA exhibited significant improvement in acetylcholine-mediated vasodilation within small arteries and arterioles (< 150 μm diameter). LIRA did not significantly alter soluble guanylyl cyclase or endothelial nitric oxide synthase (eNOS) mRNA levels, nor total myocardial eNOS protein expression. However, LIRA led to a notable downregulation of Nox-1 mRNA (p = 0.030) and a reduction in ET-1 protein expression (p = 0.044). Moreover, LIRA significantly suppressed the expression of proinflammatory and profibrotic biomarkers, including NF-κB, CD68, IL-1β, TGF-β1, osteopontin, and nitrotyrosine, in comparison to vehicle-treated rats [66]. There have been equally favorable observations in healthy volunteers with obesity and patients with either diabetes, stable coronary artery disease or unstable coronary artery disease. In each group microvascular blood flow velocity, blood volume, and myocardial perfusion were increased and improved, respectively, to variable degrees [67].
Favorable Metabolic EffectsGLP-1R agonists has shown to reduce the effects of several atherosclerotic cardiovascular disease (ASCVD) metabolic risk factors including diabetes mellitus, hyperlipidemia, overweight and obesity, and hepatic steatosis [68].
Anti-hypertensive EffectsEssential hypertension is ubiquitous worldwide and contributes substantially to cardiovascular disease-associated morbidity and mortality. GLP-1 agonists exert anti-hypertensive effects compared to placebo [69], reducing systolic blood pressure by 2–3 mmHg. There are several mechanisms that include vasodilation, natriuresis, and decreased sympathetic activity [70].
Neurohumoral EffectsIn the central nervous system, GLP-1Rs are highly expressed in regions involved in metabolic regulation, appetite, and autonomic control. Key sites include the hypothalamic nuclei (arcuate, paraventricular, dorsomedial), area postrema, nucleus of the solitary tract (NTS), dorsal motor nucleus of the vagus nerve, amygdala, lateral septum, hippocampus, and cortex. These receptors are present on both neuronal cell bodies and axonal projections and are found in GABAergic and glutamatergic neurons depending on the region [71].
In the peripheral nervous system, GLP-1Rs are expressed on vagal afferent neurons, enteric neurons, dorsal root ganglia, and nerves innervating metabolically active tissues such as adipose tissue and the gastrointestinal tract. Vagal neurons are a major site for peripheral GLP-1 action, mediating gut-brain communication for the regulation of feeding, gastric emptying, and glucose metabolism [72]. GLP-1Rs are also present on Schwann cells and sensory, motor, and enteric neurons, implicating them in peripheral neuropathy and metabolic disease modulation [73]. GLP-1Rs agonists exert neuro-humoral actions by stimulating insulin secretion and suppressing glucagon release in a glucose-dependent manner, delaying gastric emptying, and reducing appetite via central nervous system pathways. These agents act on GLP-1Rs distributed in pancreatic, gastrointestinal, cardiovascular, hepatic, and neural tissues, mediating both peripheral and central effects.
Neuro-humoral actions include modulation of hypothalamic appetite centers, leading to increased satiety and reduced caloric intake, as well as slowing of gastric emptying, which further contributes to appetite suppression and glycemic control [74]. GLP-1R agonists also demonstrate neuroprotective effects, including reduction of neuroinflammation, oxidative stress, and neuronal apoptosis, with emerging evidence for benefit in neurodegenerative diseases such as Parkinson’s and Alzheimer’s disease [75, 76].
Vascular Aging EffectsVascular aging, marked by structural and functional changes in the vascular wall, is a hallmark of the aging and is strongly linked to cardiovascular mortality and age-related vascular disorders development [
Comments (0)