
Remember me







In 1886, Harald Hirschsprung described what he thought was a new and rare condition at the Berlin Congress for Children’s Diseases. He presented two cases of a 7-month-old and an 11- month-old boy, each with progressive abdominal distention and severe difficulty passing stools, starting at birth were described. At necropsy, the hugely dilated thick walled colon with intraluminal fecalomas, mucosal ulceration and a normal calibered rectum were. In 1888, unaware of previous reports, summarized his findings in an article entitled “Constipation in Newborns as a Consequence of Dilatation and Hypertrophy of the Colon” [1,2,3,4].
Whereas before the first description of this disease by Harald Hirschsprung in 1886 (first published in 1888), approximately 20 similar cases had been recorded between 1825 and 1888 years in the literature [1,2,3,4, 6,7,8,9,10,11,12]. First, a case had been described in 1691 as a phenomenon of an over-enlarged colon by Ruysch [1,2,3,4, 8]. The earliest ones were thought to be those of Parry in 1825 and Billard in 1829.” F. Jayle in 1909″ called attention to a report by Frederich Ruysch dated 1691, and now generally accepted as the first recorded instance of this disorder. This was the case of a child who died at the age of 5 years and who was autopsied by Frederick Ruysch. The observation was reported in his work. Observationurn Anatomici-Chirurgicarum Centuria, which was published in Amsterdam in 1691 [8]. A severe case of constipation, which he followed for nearly 10 years, was published as a book in 1800 after Domenico Battini’s death [9]. This book not only provided a very careful account of the patient’s clinical development but also provided a detailed postmortem examination of the abdominal viscera, with reference to changes occurring in the intestines [9]. The unique case reported by Lewitt in 1867 is the first to appear in the American literature [10]. Lewitt’s article, in which he wrote about the postmortem findings of a patient who had had similar attacks repeatedly until the age of 12 and who had not been discharged for 3 weeks, was an important study on colon enlargement. Even, in a 2011 article, the knowledge of ancient Hindu surgeons about Hirschsprung’s disease was demonstrated with evidence from the Sushruta Samhita, dating from around 1200–600 BC [11]. Sushruta Samhita is an ancient tome of Ayurvedic surgery compiled by Sushruta (circa 1200–600 bc). A condition called Baddha Gudodaram in this book, described in the Samhita, closely resembles Hirschsprung disease. There were indications that ancient Indians even deciphered the etiology as defective nerves. Although the ailment was considered incurable, a palliative operation has been discussed as descriptive details of the operation matched with sigmoid colostomy. Evidence from Sushruta Samhita was indicated that Hindu surgeons of prehistoric India probably had considerable knowledge about Hirschsprung disease [11]. While Harald Hirschsprung summarized his findings in a publication in 1888, unaware of previous reports, it can be seen in the literature that this disease was successfully treated years ago [12,13,14].
In 1893, Walker Griffiths reported that in the autopsy of a child who died with colon dilatation, the longitudinal and circular muscle layer of the hypertrophied colon was hypertrophied and that there was chronic inflammation of the mucous membrane [12]. The rectum was somewhat large for a lad of 11 years, and its muscular walls are thinner than natural. They suggested that this unique condition was initially caused by inflammation of the mucous membrane called colon-colitis and became chronic due to various reasons, that a great intestinal distension occurred due to the changing chemical chains in the stool and that a lot of gas was produced. He also suggested that this expansion of the intestines would naturally make peristalsis more difficult, that the difficulty in pushing the stool forward was compensated by the increase in the size of the muscle fibers and by the formation of new fibers, e.g., a true muscle hypertrophy developed [12].
In an article published in 1898, Treves suggested that cases of “idiopathic colonic dilatation” in children were less “idiopathic” than in the elderly [13]. In this article, in which he presented a young child who clearly showed the features of “idiopathic colonic dilatation”, as indicated by excessive abdominal distension, persistent constipation, hypertrophy of the lower part of the colon, and the practical failure of all purgative measures, he showed that there was evidence that the great majority of these children were due to congenital narrowing of at least the lower extremity of the large intestine.
In 1901, Karl Tittel had shown for the first time that there were no ganglion cells in the distal rectum [5]. The case of a 15-month-old infant with abdominal distension was that started 8 days after birth and who suffered from the lack of a bowel movement for 11 days. The child was developing fairly well while on breast feeding. After the child was switched to cow’s milk, his/her health status deteriorated and the child died of bowel obstruction. Once again, an autopsy revealed megacolon, and as Tittel noted, it was very interesting that the ganglia of myenteric plexus could hardly be found. Normal findings were found in ileum. Tittel thought it could be impaired bowel fixation, but he almost immediately doubted this thesis when a well-defined sympathetic ganglion was found outside the rectum wall. More compelling was his notion that a probable cause of impaired peristalsis was not macroscopically detected changes of the bowel but a disorder of intramural innervation [5].
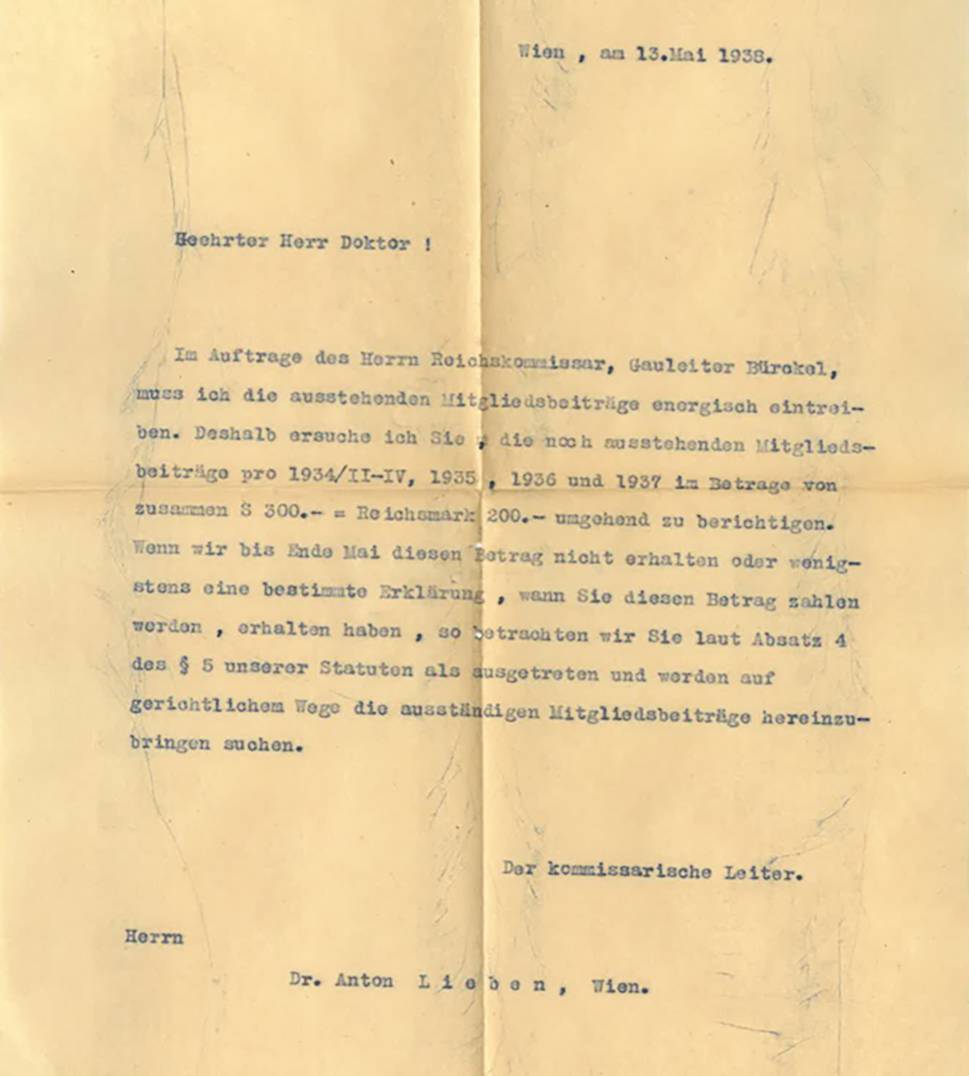
There are important articles about this disease in the literatures between 1880 and 1950, especially two systematic reviews by Finney (1908) and Whitehause & Kernohan (1948) among these articles were particularly interesting and informative, as well as the work of Tittel’s study [14, 15] (Fig. 2).
Fig. 2
Photocopies of first pages from articles of Tittel’s, Finney’s and Whitehause and Kenohans’ are seen as respectively
The first of is titled “Congenital Idiopathic Dilatation of the Colon (Surg Gynec&Obst, 1908;6:624–643)” in which 246 references were reviewed and written systematically by JMT Finney [13] (Fig. 2). Finney presented a 9-year-old boy who had constipation and abdominal distension since birth [14]. Findings of Hirschsprung disease were very typical in his history. In the abdominal exploration, it was observed that the diameter of the sigmoid colon, which was severely dilated hypertrophied, reached 14 cm, its mesentery was thickened up to 3 cm, and the other intestines were normal; and the patient underwent a right transverse colostomy. Finney’s study on congenital megacolon is one of the most comprehensive studies on this subject and examined all studies on congenital megacolon as well as the presentation of his own case. In this article, he made a comprehensive review of 246 articles on congenital megacolon (clinical presentation, medical history and naming of the disease, etiological causes, diagnosis, treatment and histopathological evaluations) [14].
One of the highlights of Finney’s article was naming of the disease [14]. It has been reported that the disease had been called as Hirschsprung disease by European authors since 1900, but it has been named as congenital colonic dilatation in non-European countries [1, 2, 4, 6,7,8,9,10,11,12,13,14]. In Finney’s article, he also mentioned Hirschsprung disease from page from especially where the authors he cited discussed their topics [14]. Although it has been determined that “German and Dutch authors used it as Hirschsprung’s Disease, while American, English and French used it as “congenital idiopathic dilatation of the colon”, but Finney it used as “Hirschsprung Disease” from on page 628 of his study [14].
On page 640 of Finney’s article, “Indeed, there has been repeated suggestion of congenital absence of the normal nervous plexus in the colon wall.” is written, but which author’s work is not mentioned [14]. Tittel (1901), and Brentano (1904), who reported the absence or scarcity of ganglion cells in the rectum in two studies until 1908, appear to be included in the references section of Finney’s article. But, both authors’ names were miswritten with a letter error in the form of Tattel and Bretano by Finney (Fig. 3).
Fig. 3
In the references list of Finney’s article, it is seen that both Tittel and Brentano were miswritten with a letter error as TATTEL and BRETANO
The second important study in the Literature is titled “Myenteric Plexus in Congenital Megacolon: Study of Eleven Cases” by Whitehouse FR, and Kernohan JW [15] (Fig. 4). In that study, the presentation of their 11 cases with congenital megacolon and literature review about congenital megacolon histopathology were made. Other ten authors data were collected from the literature, 14 of these 18 cases showed that myenteric plexus ganglia were not found in the distal part of the colon or in an unspecified part of the colon. Those studies were listed in chronological order in a table in that study by Whitehouse FR and Kernohan JW. In this histopathological review, study made in 1948, and Tittel (in 1901) was shown in the first place and Brentano (in 1904) was shown in the second place in a table (Fig. 4). Both authors reported scarcity or absence of ganglion cells in their study [15].
Fig. 4
In this table of Whitehause and Kerhonan’s article [18] is seen that in 14 of 18 cases collected from the literature, there was absence of the ganglions of the myenteric plexus in the distal part of the colon or in a part of the colon not specified. The ganglions of the myenteric plexus in the distal part of the colon or in a part of the colon not specified were absent
The literature on congenital aganglionic megacolon discussed in this study is listed separately in chronological order in Table 1 (Table 1).
Table 1 Chronological order of leading articles. The table is marked with an (*) by authors who indicated that there were no ganglion cells in the rectum and colon
Comments (0)