
Remember me
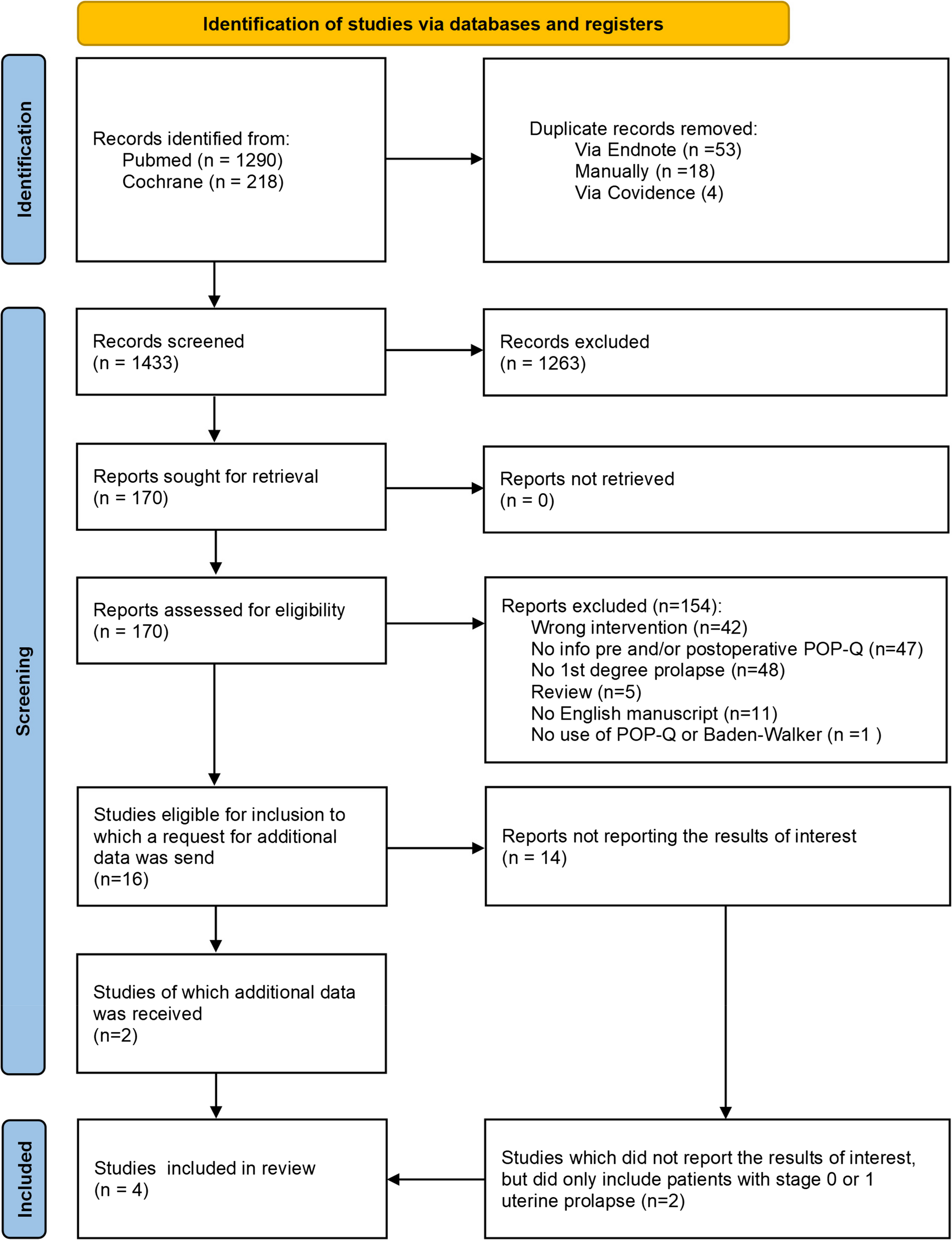
From 400 BC to 2025 AD, a total of 308 publications were sourced, of which 50 were pre-1900. Obstetric indications accounted for 116 publications (37.7%), nearly all on incarceration of a retroverted gravid uterus. Gynaecological indications, including conservative and surgical interventions, accounted from 107 publications (34.7%). Factors relevant to pelvic floor dysfunction, including imaging, diagnosis and prevalence, were in the remaining 85 publications (27.6%).
DefinitionThe definition and simple classification of the retroverted uterus has been non-controversial over the last 240 years [3,4,5,6,7]. A uterus is described as retroverted when the cervix is pointing downwards and forwards and the axis of the body of the uterus is directed backwards, towards the hollow of the sacrum, and away from its “normal” (anteverted) position overlying the bladder. The longitudinal axis of the anteverted uterus is approximately at right angles to the vagina, whereas the axis of the retroverted uterus tends to be similar (closer to parallel) to that of the vaginal axis. The anteriorly placed cervix is close to the bladder and urethra, as opposed to the position of the cervix of an anteverted uterus lying in the posterior fornix and directed infero-posteriorly.
If angulation of the body (corpus) of the uterus on the cervix, at the level of the isthmus, is more pronounced, the retroverted uterus should additionally be termed “retroflexed” (see Fig. 1).
Fig. 1
Left: anteverted uterus. Right: retroverted uterus. Centre: retroverted, retroflexed uterus.(Copyright: Bernard Haylen and Levent Efe, leventefe.com.au)
HistoryThe retroverted uterus has a long and interesting history, with large gaps in reporting. The majority of the case reports are obstetric cases, in particular the incarceration of a gravid retroverted uterus in the second trimester (generally) causing urinary retention and, at times, maternal and foetal compromise.
A: Early History (400 BC to 1890 AD)—Relationship to (Clinical) Voiding and Defecatory Dysfunction; Early Prevalence Figures 47 out of 308 Publications (15.3%)The retroverted uterus is mentioned in the writings of Hippocrates (around 400 BC) according to Smith in his 1869 paper [8], specifically the books “De Morbis Mulierum” and “De Naturâ Muliebri”. Edwards [9], in 1849 cites references to the retroverted uterus by Philomenas, amongst other “ancients” such as Rod à Castro, Mauricean and La Motte. The description given by Aëtius Tetrabiblos (Medice Artis Principes, fol. 1567) and recorded in the original Latin by Smith [8], points to an author (Aëtius) clearly acquainted with different forms of malpositioning of the uterus. The recommended treatment of acute severe cases (urinary retention, obstructed defecation) by urinary catheter, enema and pressure on the uterine fundus per rectum, the latter measures (as recorded by Smith), “delegated to his midwife”, is not so different from equivalent current emergency treatments.
Following Aëtius Tetrabiblos, Edwards [9] suggested that the subject of the retroverted uterus had been “almost lost sight of” until Desgranges (1715), Gregoire (1746) and Hunter (1754) drew attention to it and “placed the matter in a clear and intelligent light”.
The celebrated anatomist, William Hunter (1718–1783) is generally credited with being the first to have named “retroversion of the uterus” and described several case histories [10]. Some of the cases in this and an earlier paper were communicated to Hunter by William Bird (1750) and Maxwell Garthshore (1732–1812). Cockell [7] also refers to Hunter’s 1954 lecture on the subject. Edwards [9] also cites the clinical entity of the retroverted uterus as being described by John Maubray (died 1732) in his popular text, the “Female Physician” (London, 1724).
Voiding DysfunctionIncluding urinary retention in pregnancy, most of the reported cases are due to a uterus impacted (“incarcerated”) in the pouch of Douglas, with corresponding marked cervical pressure anteriorly and superiorly placed on the bladder base. Oliver [11], in 1890, reported a case of death from rupture of the bladder and subsequent peritonitis in a fixed retroverted gravid uterus. In another case described by Corkhill [12] in 1887, the cervical os was palpable above the pelvic brim. Edwards [9], in 1849, reported three cases of voiding dysfunction associated with non-gravid uterine retroversion, with two of the uteri being “hypertrophied” (perhaps with fibroid involvement).
Defecatory DysfunctionHerman [13, 14], in 1882, highlighted the impact of a severely retroverted and retroflexed uterus on the rectum, citing a case from the Edinburgh Medical and Surgical Journal of 1854 (p. 336) in which the fundus protruded at the anus when the patient defecated. Edwards [9], in 1854, noted that the pressure of the fundus against the rectum can produce “severe constipation” or even “difficulty in going to stool at all”. Cyclical (premenstrual—when the uterus is more congested and thus heavier) exacerbation of defecatory dysfunctions, due to retroversion, recognized as far back as 1854 [9], most likely represents a degree of extrinsic impingement on the rectum. Herman [13, 14], in 1882, discussed the relative merits of a Hodge and ring pessary in relieving symptoms, with support from Smith [8] and subsequent support from McCann [15] and Luker [4]. There were some more unusual designs, such as the one used by Murray [16] in 1868 (Fig. 2), which might be directed at supporting the lateral fornices of the vaginal vault [1] to elevate the uterus.
Fig. 2
An early pessary. From W. Murray (1868) [16]. A spring pessary for the relief of retroversion and retroflexion of the uterus by active extra-uterine support. Permission granted to reproduce by Elsevier
Early Prevalence FiguresHerman [13, 14] quotes the extensive clinical (clearly no ultrasound imaging available) studies of Vedeler (Archiv fur Gynäkologie, vol xix, p. 294), a physician who practiced in Christiania (more likely the old name for Oslo, Norway, though possibly a district in Copenhagen, Denmark). The overall prevalence of retroversion in 1504 healthy women was 16.5%: 14% in healthy virgins (414 examined); 12% in healthy nullipara (506 examined); 22% in parous women (584 examined). Of 1158 women with uterine symptoms, 259 (22.4%) had a retroverted uterus.
Period B: (1891–1955)—More Emphasis on Clinical Diagnosis, Conservative and Surgical Management; 37 out of 308 Publications (12.0%)Luker [4] emphasizes in 1934 that most retroverted uteri are asymptomatic, with women generally unaware of their presence; no investigation or treatment is required. Surgical correction (ventrosuspension) was becoming popular in this period, generally by a modified Gilliam ventrosuspension (a.k.a. ventrofixation). A permanent suture (silk at the time) was used to attach a loop of round ligament on each side to the rectus sheath. Luker [4], however, emphasized that “it is preferable to give a good trial to medical treatment (including pessaries) before resorting to a surgical operation” for symptomatic retroversion. Indications for surgical relief of uterine retroversion in 1934 [4] included:
1.Infertility (sterility and miscarriage—now a rare reason
2.Fixed retroversion associated with pelvic pain (of whatever cause)
3.Dyspareunia
4.Pelvic floor discomfort
5.Voiding and defecatory dysfunction
Rendle-Short [17], in 1941, quotes “only” a 50% perfect symptomatic and anatomical result from a series of 120 patients who had undergone ventrosuspension, with other functional or orthopaedic causes possibly present.
Attempts at further clinical classifications during this time [4, 13,14,15] did not last. As previously noted, the simplest and most relevant clinical classification is anatomical, depending on the presence or absence of retroversion and whether retroflexion is additionally present.
Fothergill [18] perhaps too closely links retroversion with the development of prolapse in his 1912 comments: “every case of classical prolapse is characterized by both cystocoele and retroversion”. The Fothergill (Manchester) repair involves anterior colporrhaphy, plication of the merged uterosacral and cardinal ligaments, and amputation of the cervix.
Period C: (1956–1985) 41 out of 308 Publications (13.3%)There was a slowing down in the performance of ventrosuspensions; this was a relatively quiet period in the history of the retroverted uterus, although there was some discussion on aetiology [5].
The retroverted uterus is thought normally to be a developmental occurrence [6] although acquired retroversion can occur owing to the effects of endometriosis, pelvic inflammatory disease and pelvic tumours. There is no clear evidence to support a “traditional theory” [18] that the anteverted uterus becomes retroverted as it prolapses. Symmonds [5] proposes a strong argument, on the basis of the axes of the retroverted uterus and the vagina being in line: “intra-abdominal pressure can exert a piston-like action on the retroverted uterus driving it down the vagina”. In contrast, the anteverted uterus would be forced infero-posteriorly, receiving support from the rectum.
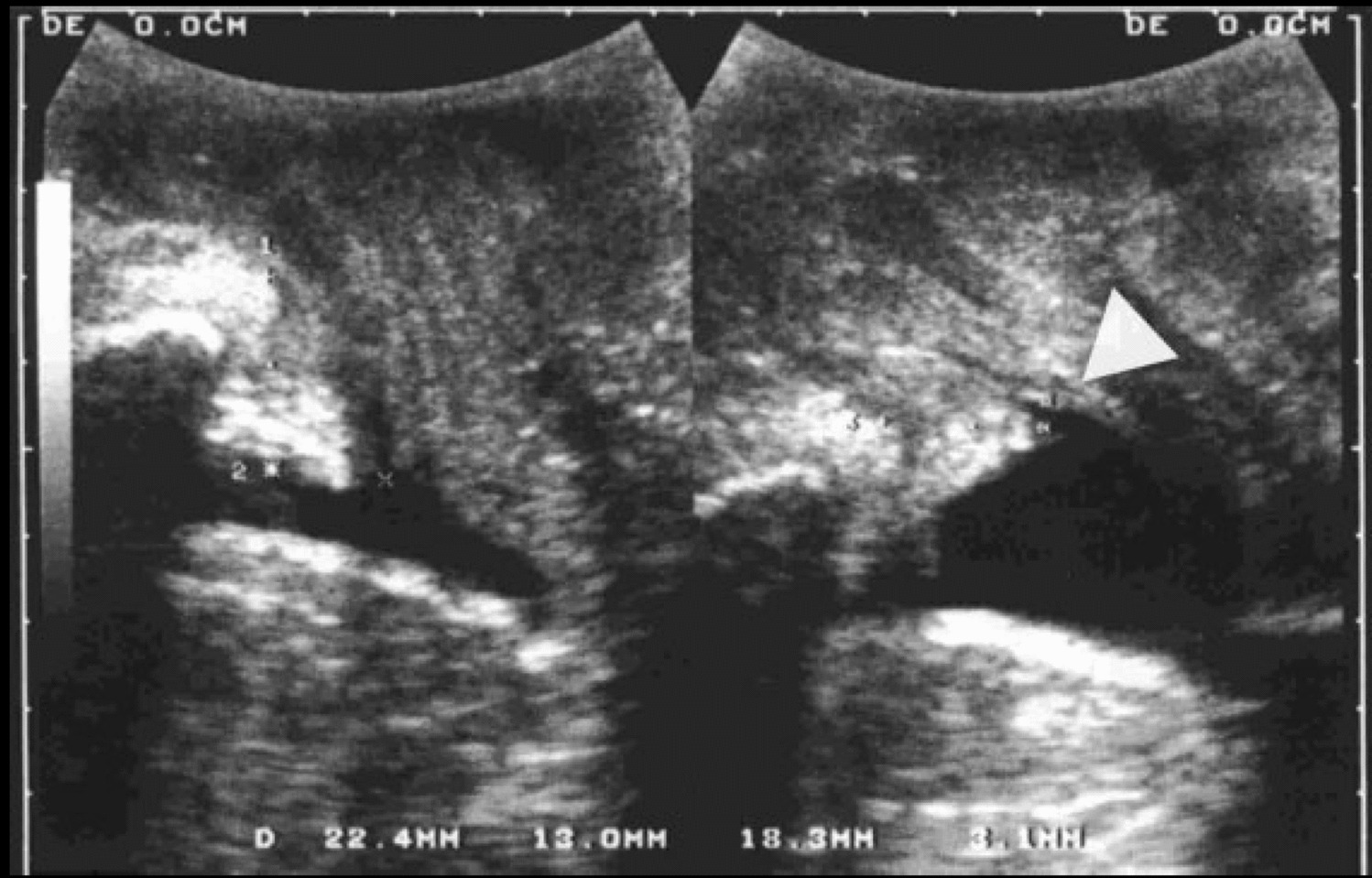
Period D: (1986–2007)—Transvaginal Ultrasound Clarifies the Diagnosis and Prevalence of the Retroverted Uterus and Relationship to Pelvic Organ Prolapse; 93 out of 308 Publications (30.2%)The advent of transvaginal ultrasound in urogynecology in 1987 allowed a far more accurate appreciation of the retroverted uterus than had previously been possible. Apart from measuring bladder volumes [19] including postvoid residuals, some of its other routine uses were identifying intercurrent pelvic/lower urinary tract pathology and the presence/absence of uterine retroversion (empty bladder important) [19, 20].
Freimanis and Jones [20] determined that an accurate ultrasound of the retroverted uterus required
1.The use of transvaginal ultrasound because of the superior resolution of that modality and the proximity of the probe to the area of interest
2.An empty bladder
In confirming these criteria, Haylen et al. [21] noted a significant reduction in the prevalence of the retroverted uterus in 480 general gynaecology patients receiving subspecialist ultrasound assessment from 18% (empty bladder, transvaginal ultrasound used) to 13% (full bladder, transabdominal ultrasound used).
In a study of a urogynaecological patient population [7] of 592 women using a clinical and transvaginal ultrasound (empty bladder) diagnosis, a 34% prevalence of the retroverted uterus, 79% greater than for the general gynaecological population, was found, with uterine (and co-existent vaginal) prolapse issues the likely reason for this 1:3 prevalence. Fauconnier et al. [22] noted a 24% prevalence of the retroverted uterus by clinical examination alone (ultrasound was not routinely used) in an unselected population of women attending for routine gynaecological assessment. In the same study, women with retroversion were noted to have a significantly higher prevalence of dyspareunia and severe dysmenorrhoea (67% vs 42%; both symptoms, p = 0.03), with no association with noncyclic, ovulation or premenstrual pain.
In a further analysis of the earlier urogynaecological patient population [7, 23] of 592 patients, using routine clinical and transvaginal ultrasound (empty bladder) diagnosis, there was a 4.5-fold increase in presentations with stage II–IV uterine prolapse in women with a retroverted uterus than in those with an anteverted uterus. There was a higher prevalence of stage II–III cystocoele (×1.9) and at least stage I vaginal vault descent (×4.7) in association with a retroverted uterus than was the case with an anteverted uterus. The earlier comments of Symmonds [5] provide a very plausible explanation.
Period E: (2008–2025)—Relationship of the Retroverted Uterus to Other “Most Common” Urodynamic Diagnoses; Repopularization of Ventrosuspension by Laparoscopy; 90 out of 308 Publications (29.2%)The advent of the International Urogynecological Association/International Continence Society Female Pelvic Floor Terminology Report for pelvic floor dysfunction [2] allowed the analysis of any relationships between the retroverted uterus and the five “most common” urodynamically based diagnoses (apart from pelvic organ prolapse): urodynamic stress incontinence (USI); detrusor overactivity (DO); bladder oversensitivity (BO); recurrent urinary tract infections (UTIs); voiding dysfunction.
Urodynamic Stress Incontinence and the Retroverted UterusIn the previously cited studies [7, 23], there were no significant differences in the prevalence of USI between women with
1.An anteverted uterus
2.A retroverted uterus
3.An absent uterus
Detrusor Overactivity, Bladder Oversensitivity and the Retroverted UterusNo significant relationship was found between the presence or absence of a retroverted uterus and DO or BO diagnoses [23, 24].
Recurrent Urinary Tract Infection and the Retroverted UterusTheoretically, the chances of recurrent UTI (three or more medically diagnosed episodes in 12 months) might be more likely in women with uterine retroversion owing to more likely impingement on the anteriorly placed cervix and, in turn, greater frictional pressure of the cervix on the bladder base. In a large study, using the modified criteria of two or more medically diagnosed UTIs in 12 months, no significant relationship was found between recurrent UTI and uterine retroversion (p = 0.366). In this and the above studies, we have found no other studies to contradict the stated findings [23, 25].
Retroverted Uterus and Voiding DysfunctionVoiding dysfunction has been defined as abnormally slow and/or incomplete micturition as determined by an abnormally slow urine flow rate and/or an abnormally high postvoid residual [2]. Despite case reports of acute and chronic retention of urine associated with a retroverted uterus, there is no significant relationship between the retroverted uterus and an increasing postvoid residual (p = 0.163). In a urogynaecological patient population [23], no significant differences were found between women with an anteverted uterus, those with a retroverted uterus and those with an absent uterus in relation to the diagnosis of voiding dysfunction (previously termed voiding difficulty). In a further study [26], the absence of a significant relationship between voiding dysfunction and the retroverted uterus was confirmed (p = 0.250).
Re-popularization of Ventrosuspension by LaparoscopyOf the 183 papers in this and the previous time period, 31 (16.9%) focused on laparoscopic ventrosuspension. Newer and less morbid techniques for laparoscopic ventrosuspension, combined with a renewed awareness of the possible adverse effects of uterine retroversion for pelvic floor/general gynaecological indications, has seen a re-invigorated interest in surgical management. The non-fertility indications alluded to in 1934 [4], namely fixed retroversion associated with pelvic pain (of whatever cause), dyspareunia, pelvic floor discomfort, and voiding and defecatory difficulties, are still present. In a more general or endoscopic gynaecological practice, pelvic pain (including dysmenorrhoea and dyspareunia) may be the more predominant symptoms. Evidence for the beneficial effect of laparoscopic ventrosuspension has been recently cited [27], although the absence of randomized clinical trials precludes acceptance of uterine suspension as an established therapy for pelvic pain [27]. Multiple other scenarios for laparoscopic ventrosuspension have been quoted [28,29,30,31].
Comments (0)