
Remember me

A 10-year-old girl presented with right-sided abdominal pain and diarrhea as her chief complaints. She had no significant past medical or family history. Three days prior to hospitalization, she developed fever, sore throat, and cough during the night. As these symptoms persisted, she visited a local clinic 2 days before admission. Although a rapid antigen test for M. pneumoniae was negative, the physician diagnosed her with acute bronchitis likely caused by M. pneumoniae based on the local outbreak situation and a history of close contact with her brother, who had been experiencing persistent high fever for a week. She was prescribed tosufloxacin at a dose of 450 mg (13 mg/kg).
On the following day, the patient developed right-sided flank pain and returned to the clinic. The pain was initially considered to be due to constipation, and magnesium oxide was prescribed. However, after administration of magnesium oxide, the patient developed diarrhea the next day, leading to the discontinuation of the laxative. Despite discontinuation, the diarrhea persisted and was accompanied by nausea and vomiting.
On the day of admission, as her symptoms persisted, the patient revisited the clinic. Suspecting that her symptoms might be drug-induced, the physician discontinued tosufloxacin. However, her symptoms failed to improve after returning home, leading her to present to the emergency department of our hospital.
On admission, the patient’s body temperature was 37.7 °C, with a heart rate of 100 beats per minute and an SpO₂ of 97% on room air. She was alert and oriented. Abdominal examination revealed a flat and soft abdomen with no evidence of increased or decreased bowel sounds. However, spontaneous pain, tenderness, and rebound tenderness were noted in the right flank and lower abdominal regions. In addition, percussion tenderness was observed over the right costovertebral angle (CVA).
Laboratory results on admission revealed a complete blood count (CBC) and coagulation tests within the reference range. Blood biochemistry showed an elevated C-reactive protein (CRP) level of 1.57 mg/dL and an elevated serum creatinine level of 1.09 mg/dL. The estimated glomerular filtration rate (eGFR), calculated using the Japanese pediatric 5-variable formula [2], was 49 mL/min/1.73 m2, indicating impaired renal function. Urinalysis revealed no evidence of pyuria, with an absence of white blood cells in the urine (Table 1). The urine pH was 5.5. The calcium-to-creatinine ratio was 0.01 g/g·Cr, and the N-acetyl-β-D-glucosaminidase (NAG)-to-creatinine ratio was 13.4 IU/g·Cr. Urinary sediment examination showed 50–99 hyaline casts, 10–19 epithelial casts, and 1–4 granular casts per whole field (WF), suggesting tubular involvement.
Table 1 Laboratory tests on admissionGiven the tenderness and rebound tenderness in the right lower abdomen, the possibility of acute appendicitis was considered, and an abdominal ultrasound was performed. However, no enlargement of the appendix was observed. Instead, Grade 1 hydronephrosis in the right kidney and punctate hyperechoic areas within the renal pelvis were identified. No structural abnormalities of the kidneys were observed, and there were no findings suggestive of urinary tract obstruction. The renal cortical echogenicity was within normal limits, and no focal areas of reduced renal perfusion were clearly identified on ultrasound. During the examination, significant tenderness was elicited when the probe was applied to the affected area.
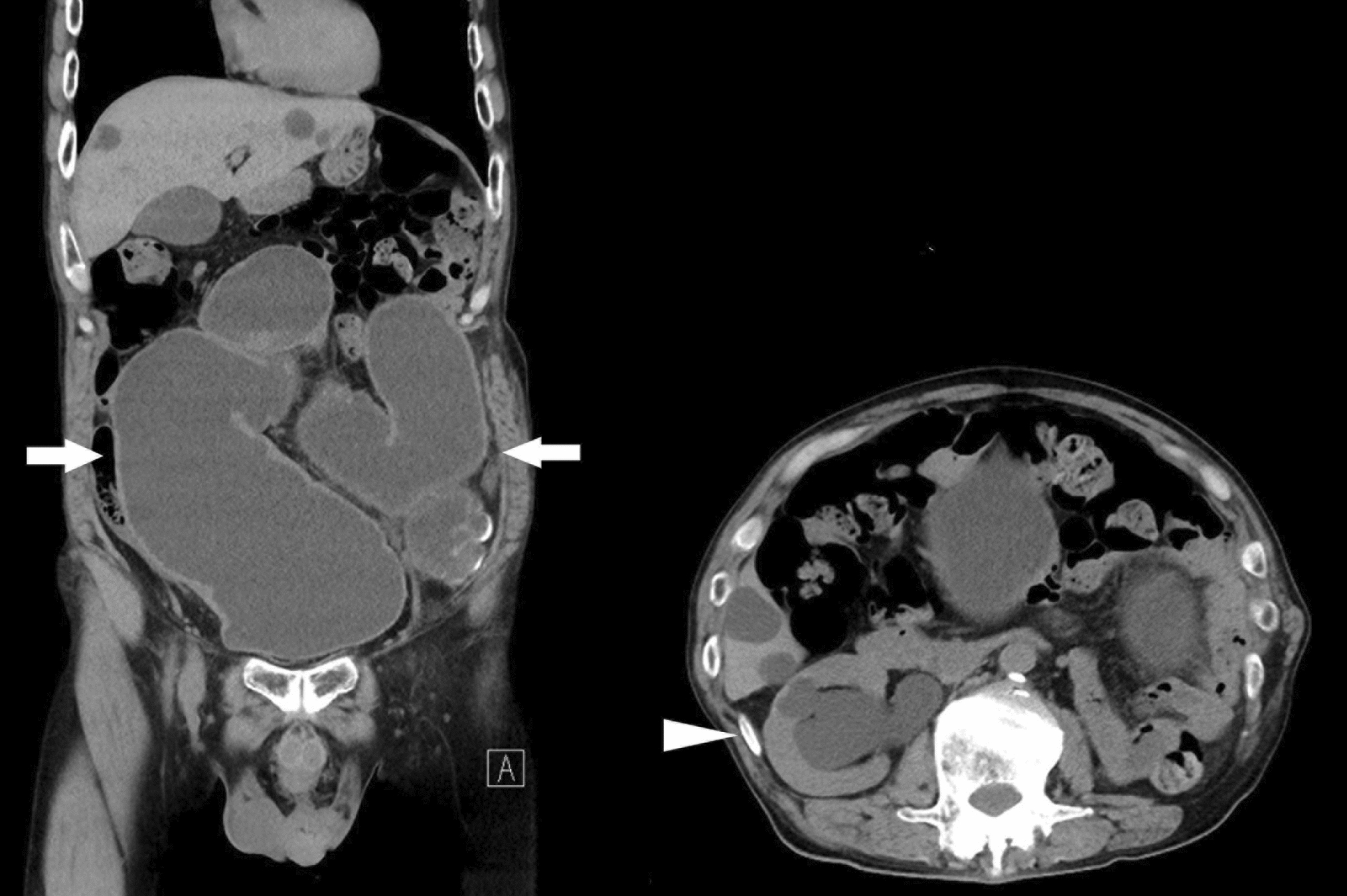
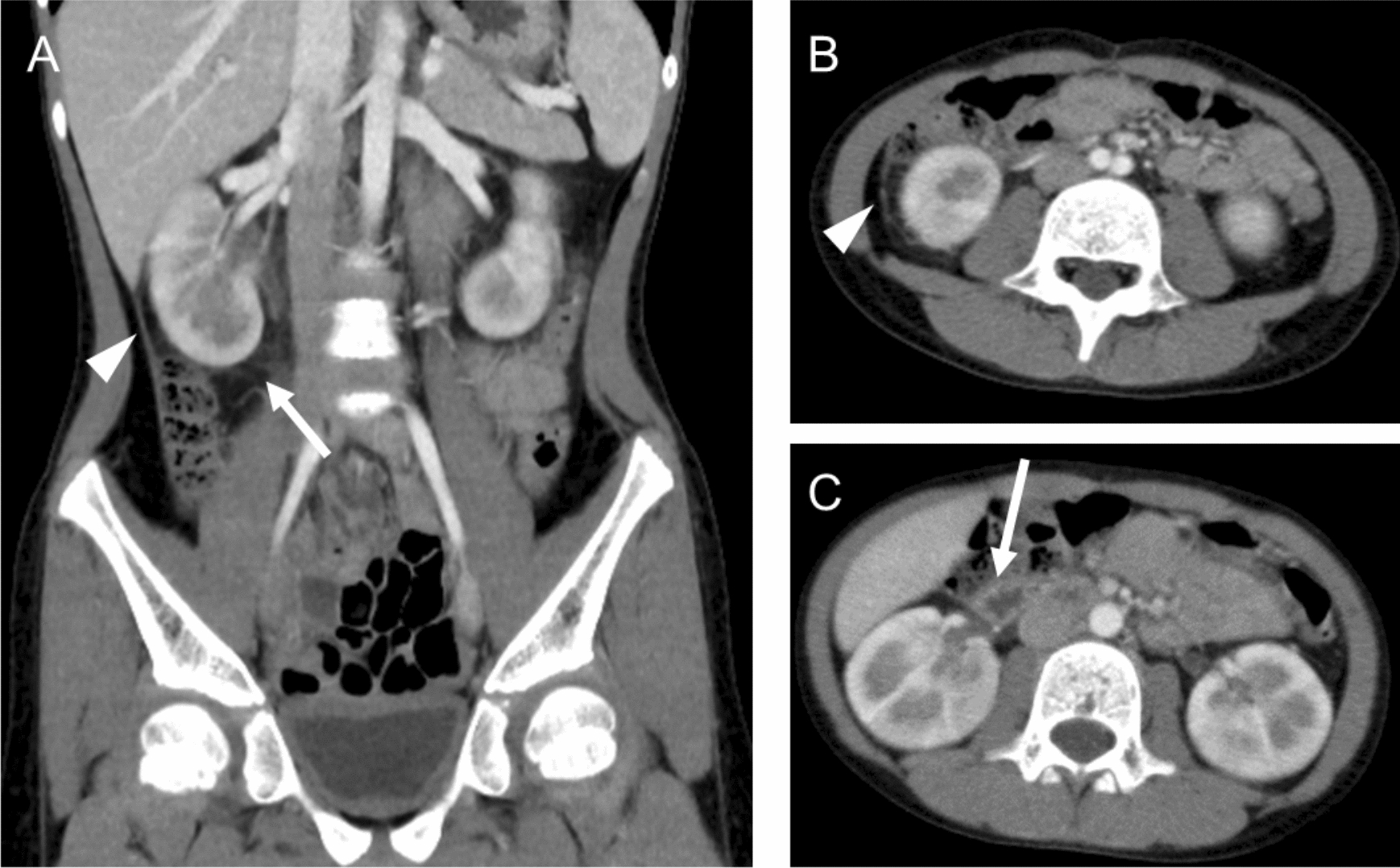
As pyuria was absent on urinalysis, an abdominal contrast-enhanced CT scan was performed to evaluate for acute focal bacterial nephritis. The CT scan did not demonstrate any hypo enhanced areas within the kidney, which are characteristic of acute focal bacterial nephritis. On the other hand, peritoneal thickening in the right paracolic gutter and fat stranding around the right kidney were observed (Fig. 1A, B). In addition, thickening of the adjacent duodenal wall was observed (Fig. 1C). These findings were suggestive of localized peritonitis, likely secondary to inflammation extending from the right kidney.
Fig. 1
Contrast-enhanced abdominal CT image of the patient. A Coronal contrast-enhanced abdominal CT scan of the patient. The arrowhead indicates peritoneal thickening in the right paracolic gutter, while the arrow denotes fat stranding around the right kidney. B Axial contrast-enhanced abdominal CT scan of the patient. The arrowhead shows peritoneal thickening in the right paracolic gutter. C Axial contrast-enhanced abdominal CT scan of the patient. The duodenal wall appears thickened (arrow)
In the absence of findings strongly indicative of a bacterial infection, the differential diagnosis included acute enteritis and adverse effects of tosufloxacin. The patient was admitted for observation without the initiation of antibiotics.
By the day after admission, her fever had resolved, and the spontaneous abdominal pain in the right abdomen showed mild improvement. By the third day of hospitalization, the abdominal pain had completely subsided, and her serum creatinine level improved to 0.55 mg/dL, with an eGFR of 86 mL/min/1.73 m2.
Urine microscopy could not be performed on the day of admission or the following day due to the weekend. However, on the third day of hospitalization, microscopy of the urine sample collected on admission revealed numerous needle-shaped and sea urchin-shaped crystals, findings consistent with drug crystals associated with tosufloxacin (Fig. 2). Under low magnification (× 100), approximately 10–20 crystals per field of view were observed in the sample collected on admission. A small amount of crystals (approximately 1 crystal per several fields of view under low magnification) was observed in the urine sample collected on the second day of hospitalization, while no crystals were detected in the sample collected on the third day. Based on these findings, the abdominal symptoms and renal impairment were diagnosed as adverse effects of tosufloxacin.
Fig. 2
Drug crystals in the patient’s urine observed under microscopy (× 400 magnification) Needle-shaped and sea urchin-shaped crystals were observed in the patient’s urine. These crystals are characteristic of tosufloxacin. The scale bar represents 20 μm
By the fourth day of hospitalization, the CVA tenderness had resolved, and the patient was discharged. At follow-up visits after discharge, she remained asymptomatic, with no signs of renal impairment or abdominal symptoms.
Comments (0)