Drug-induced kidney injury (DKI) is a major cause of acute interstitial nephritis (AIN), with drug-induced AIN (DI-AIN) accounting for approximately 70% of AIN cases [5]. This case highlights, for the first time, that Saikokaryukotsuboreito can induce AIN through an immune-mediated mechanism, similar to other well-characterized drug-induced hypersensitivity reactions. Importantly, although glucocorticoid treatment was not initiated immediately, our patient showed substantial improvement, demonstrating that DI-AIN due to herbal medicines can be effectively diagnosed and treated using established approaches for conventional drug-induced nephropathy.
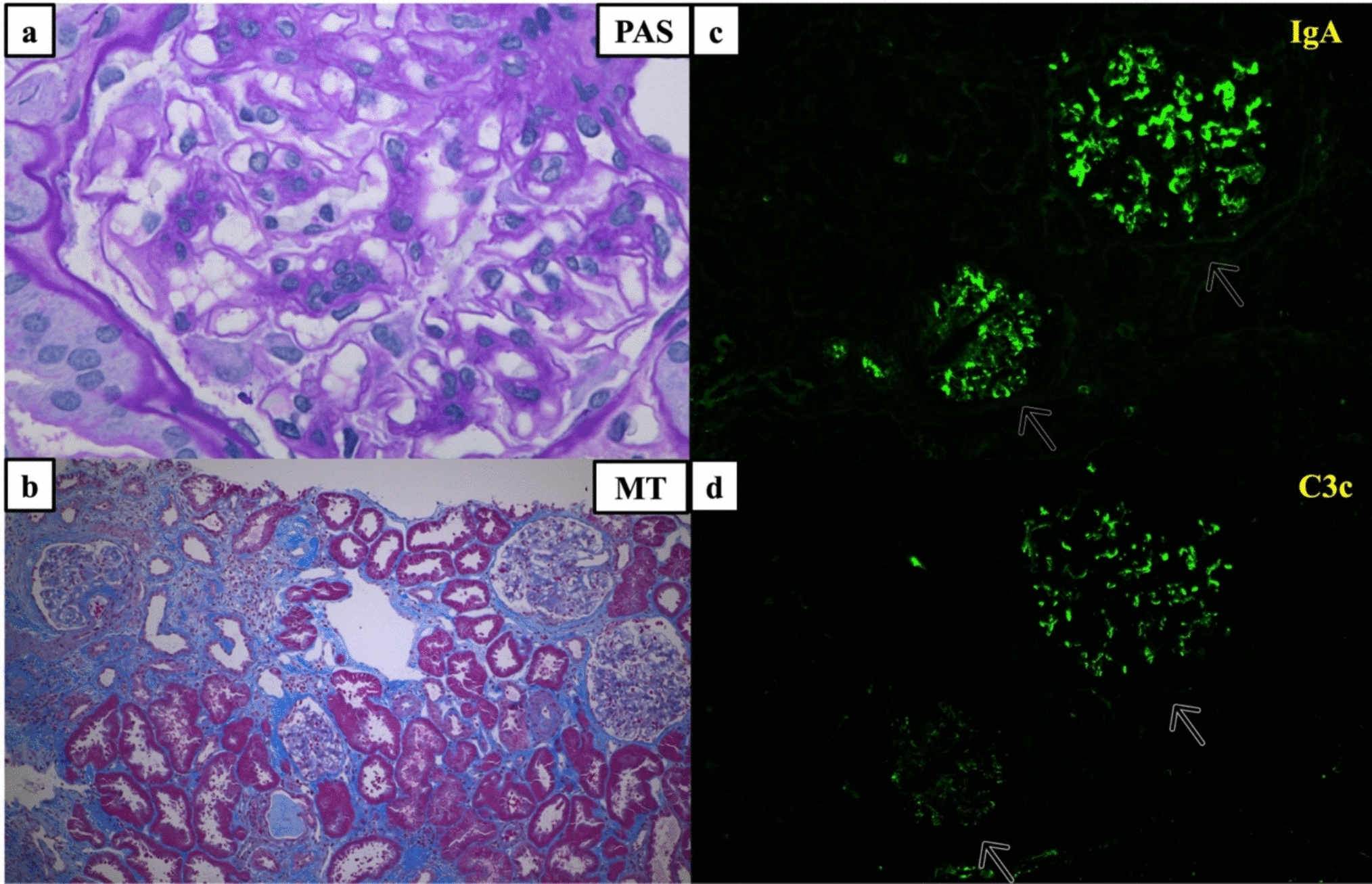
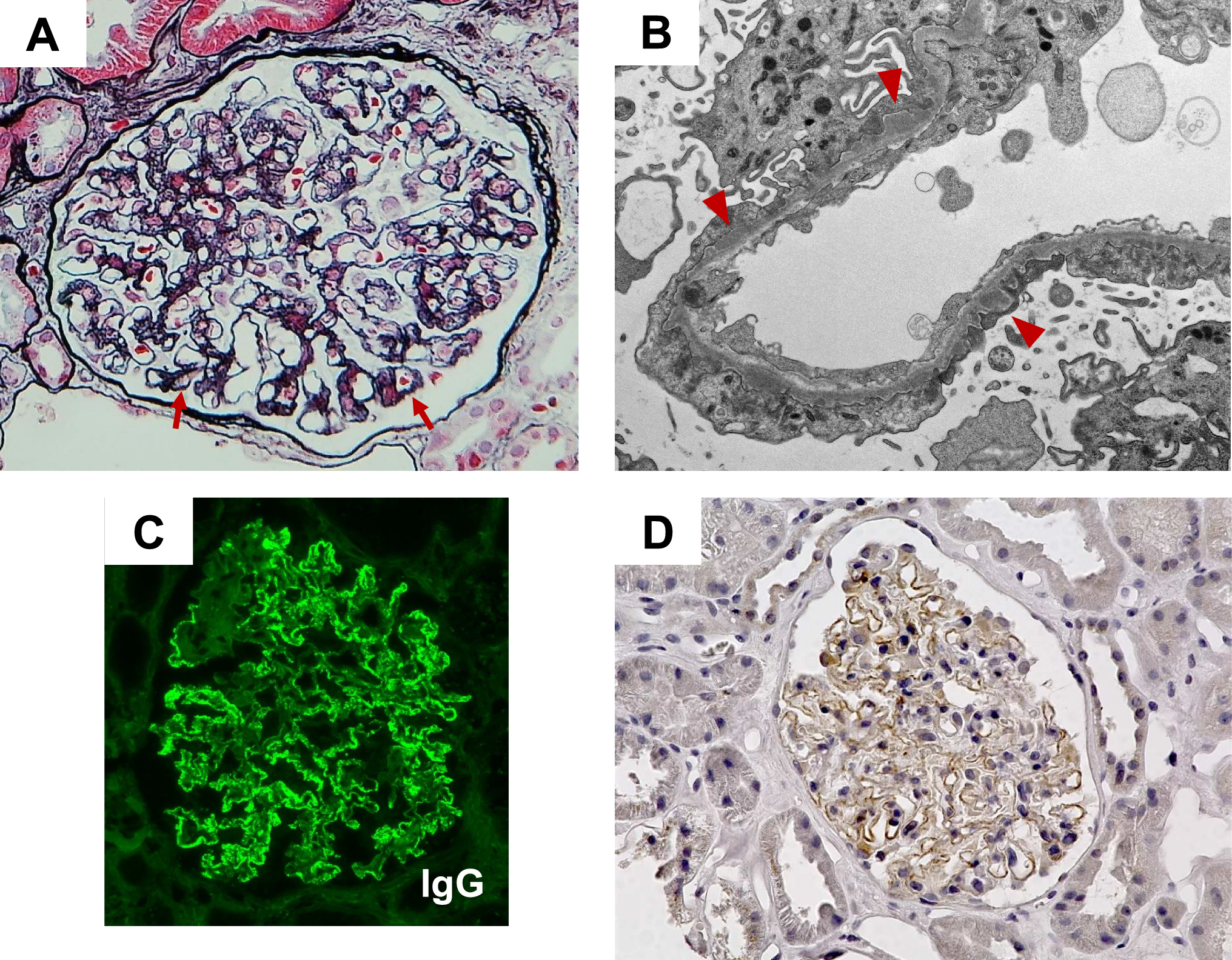
The diagnosis of Saikokaryukotsuboreito-induced AIN was supported by a comprehensive evaluation. Our patient presented with severe acute kidney injury with minimal urinary abnormalities. Renal biopsy revealed key diagnostic features of drug hypersensitivity: diffuse interstitial inflammation with predominant T lymphocytes and macrophages infiltration, marked tubulitis, and preserved glomerular architecture. This cellular composition is consistent with a cell-mediated immune response characteristic of drug hypersensitivity reactions [6]. The absence of granulomas, giant cells, or immune complex deposits helped exclude other type of AIN [7]. The immunological basis of this reaction was confirmed by positive drug-induced lymphocyte stimulation test (DLST) results for Saikokaryukotsuboreito and all four of its major components (Bupleurum root, Pinellia tuber, Scutellaria root, and Ginseng), despite their diverse chemical structures. This distinctive pattern suggests a complex immune response that may involve metabolic transformation of multiple herbal constituents rather than simple structural cross-reactivity [8].
This case must be differentiated from other forms of herbal medicine-associated nephropathy. Unlike aristolochic acid nephropathy (AAN), which causes progressive interstitial fibrosis, tubular atrophy, and cortical shrinkage through direct DNA damage [9, 10], our patient’s condition was characterized by acute inflammation without evidence of direct toxicity. We confirmed with the manufacturer that Saikokaryukotsuboreito does not contain aristolochic acid. Similarly, our case differs from the recently described Beni-koji (red yeast rice) nephropathy [11,12,13], which presents as Fanconi syndrome and acute kidney injury due to puberulic acid contamination and shows incomplete recovery despite treatment discontinuation. Kidney biopsies in these cases primarily show tubulointerstitial changes, with a recent nationwide survey reporting tubulointerstitial nephritis in 50% and tubular necrosis in 32% of cases [14]. In contrast, our patient’s biopsy lacked tubular necrosis typically seen in Beni-koji nephropathy, and the significant response to glucocorticoid therapy suggested an immune-mediated rather than toxic etiology.
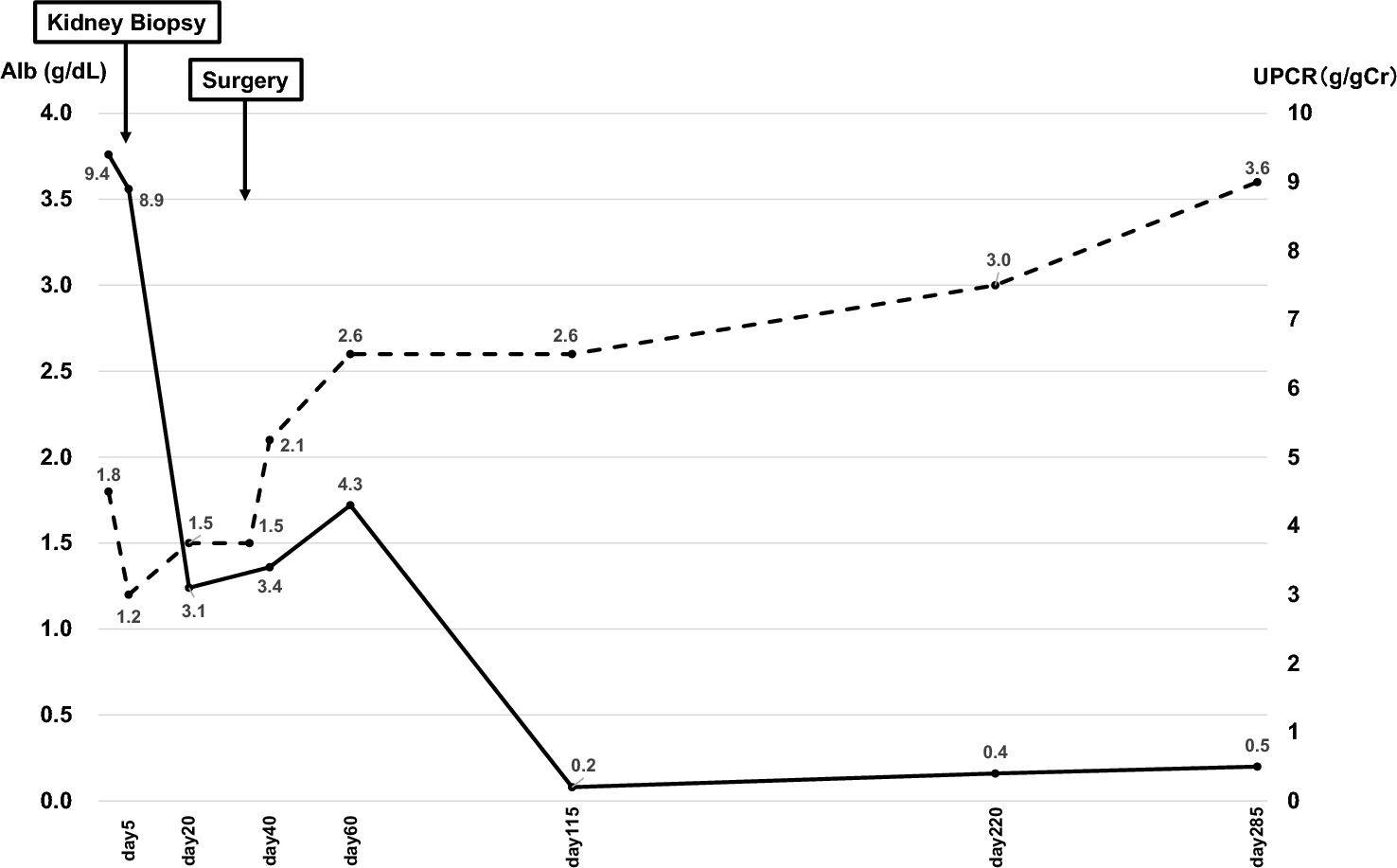
Regarding treatment, while prompt discontinuation of the causative agent is fundamental, glucocorticoid therapy remains beneficial in cases with severe or persistent renal dysfunction. Multiple retrospective studies suggest that early glucocorticoid therapy initiation is associated with improved renal outcomes and reduced progression to chronic kidney disease [15, 16]. In our case, despite initiating prednisolone approximately 50 days after Saikokaryukotsuboreito discontinuation, we observed a favorable response with normalized renal function, except for minor residual tubular acidosis. This outcome suggests that the predominantly inflammatory nature of the lesion, rather than established fibrosis, allowed for effective glucocorticoid responsiveness even with delayed initiation. This finding further indicates that AIN induced by Saikokaryukotsuboreito does not require special consideration and can be approached with the same therapeutic strategies used for conventional drug-induced AIN.
Several limitations should be acknowledged. The sensitivity and specificity of DLST are suboptimal [17], and certain herbs, including Bupleuri Radix (a component of Saikokaryukotsuboreito), may cause false-positive results due to inherent mitogenic activity [18]. In addition, we were unable to test all components of the herbal formulation. Furthermore, serum IgG4 and IgE levels were not measured during the patient’s hospitalization, which might have provided additional insights into the immunological mechanisms involved. Nevertheless, the temporal relationship between drug administration and symptom onset, combined with the consistent positive results across all four tested components, along with the improvement after drug discontinuation and glucocorticoid therapy, strongly supports causality. The fact that CD68-positive cellular infiltration was prominent in the interstitium suggested that although there were no typical giant cells, a foreign body reaction to the suspect drug may have occurred, which may have activated T cells and caused interstitial nephritis.
In conclusion, this case demonstrates that Saikokaryukotsuboreito can cause immune-mediated AIN that responds favorably to glucocorticoid therapy. It highlights that herbal medicines, despite their perceived safety, can induce significant kidney injury through mechanisms similar to conventional pharmaceuticals. Clinicians should include herbal medicines in the differential diagnosis of unexplained AIN and apply standard diagnostic and therapeutic approaches. This case underscores the importance of comprehensive medication history, including traditional remedies, and the value of both renal biopsy and immunological testing in establishing accurate diagnosis and guiding appropriate treatment.


Comments (0)