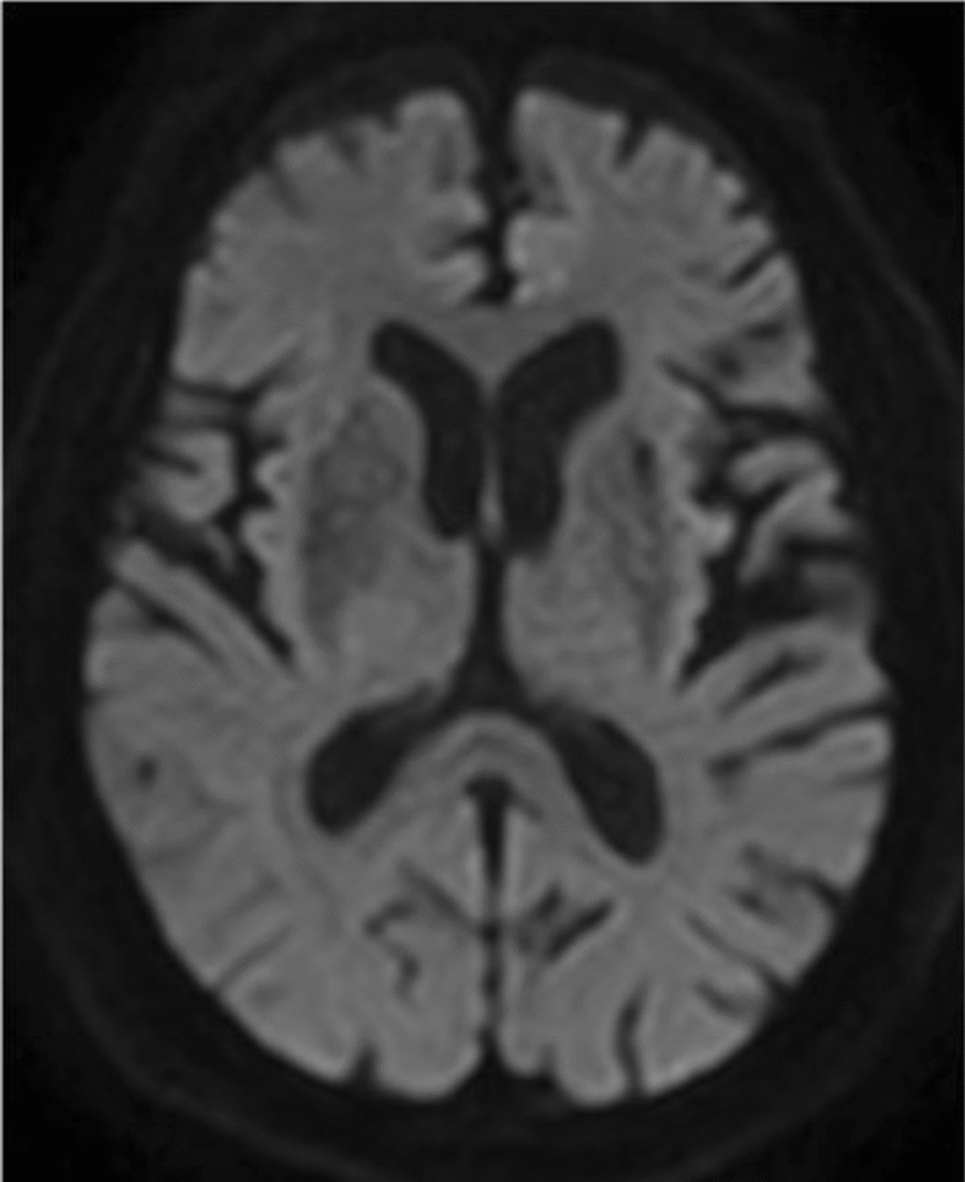
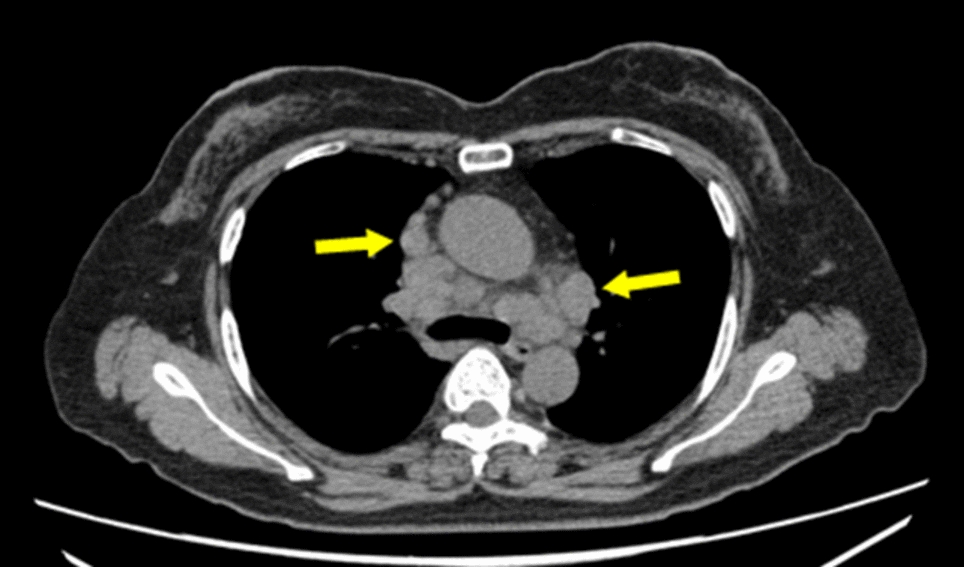
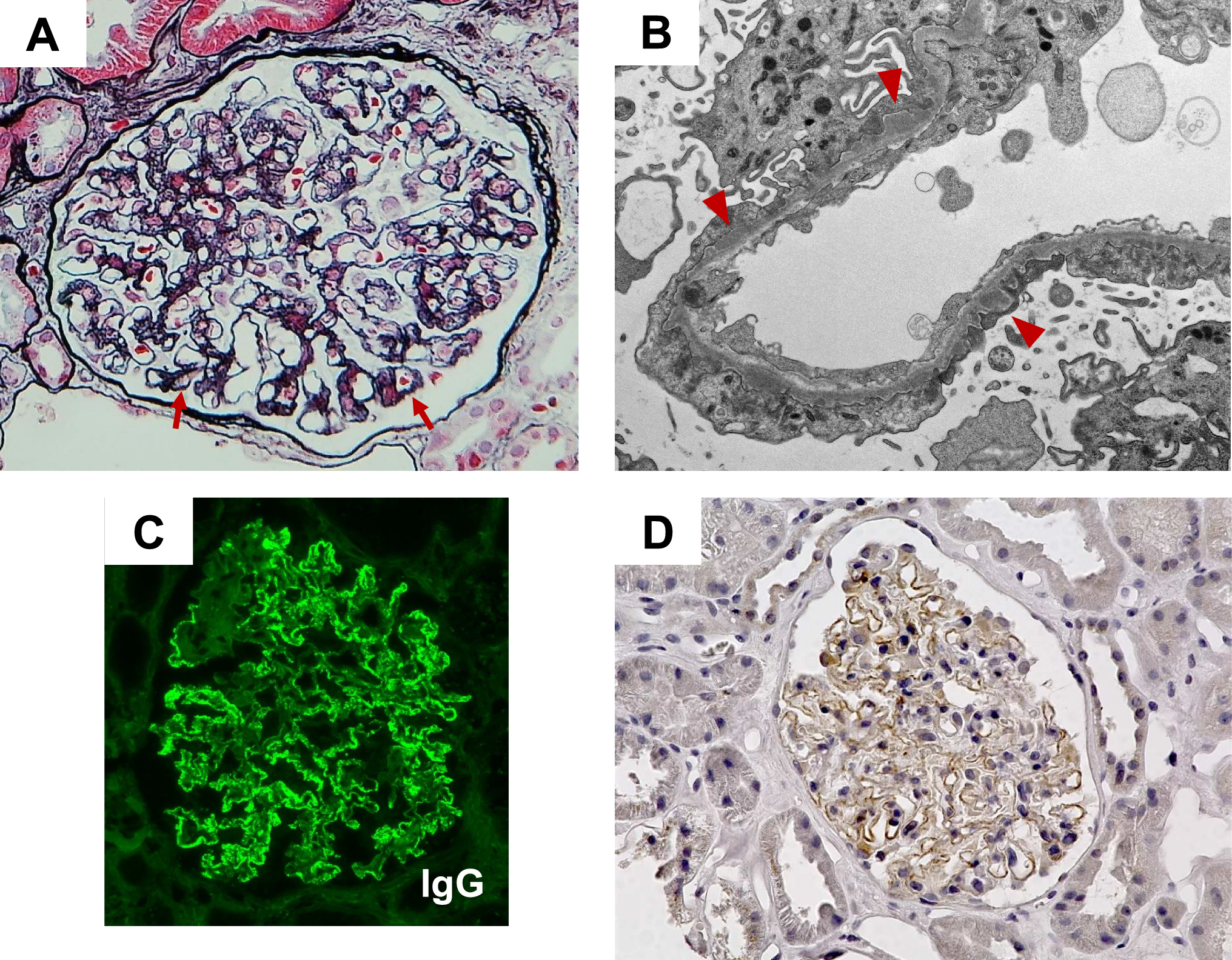
In our patient with NSCLC adenocarcinoma, brain metastases and a nephrotic syndrome due to a secondary membranous nephropathy treated with pembrolizumab, no renal excretion of pembrolizumab could be detected. After three doses, the pembrolizumab peak plasma concentration reached 79.9 ug/mL, with a trough of 13.1 ug/mL. This aligns with model-based pharmacokinetics predictions by Ahamadi et al., who forecasted a trough concentration of 16 ug/mL after three doses of 2 mg/kg every 3 weeks [9]. Of note, target saturation of PD-1 inhibition by pembrolizumab is already achieved at trough concentrations of 1 ug/mL and above [10, 11]. Thus, based on these findings, we assume target saturation in our patient. In addition, undetectable pembrolizumab concentrations in urine suggest that the paraneoplastic nephrotic syndrome did not negatively affect drug exposure. With treatment, clinical indicators of nephrotic syndrome improved since serum albumin increased from 19.8 to 29.1 g/L and urine protein declined from 1.76 to 1.17 g/L over the initial three cycles. However, the UPCR remained unchanged in this period.
Jansen et al. reported on a similar case receiving pembrolizumab for a NSCLC who also had a paraneoplastic nephrotic syndrome [12]. In their patient, also a therapeutic pembrolizumab trough concentration (73.1 ug/mL, after three doses) was observed. However, in contrast to our findings, pembrolizumab was observed in their patient’s urine in a concentration of 2.4 ug/mL. The authors concluded that despite renal loss of pembrolizumab because of the paraneoplastic nephrotic syndrome, treatment resulted in therapeutic drug exposure and both a radiological and clinical response [12]. In nephrotic syndrome, alteration of the glomerular filtration barrier leads to increased urinary excretion of proteins. The severity of this membrane dysfunction correlates with the clinical severity of nephrotic syndrome, as reflected in laboratory findings such as increased proteinuria and decreased serum albumin concentrations [13, 14]. Compared with the case presented in the article by Janssen et al., our patient had a less severe form of paraneoplastic nephrotic syndrome (hypoalbuminemia 19.8 g/L versus 7.0 g/L) and proteinuria (UPCR 3.2 versus 11.5 g/gCr). This is a possible explanation for the difference in urinary pembrolizumab concentrations. However, to our knowledge, there is only scarce evidence regarding studies investigating the renal excretion of pembrolizumab in patients with proteinuria. Looking into the evidence for Immunoglobulin G (IgG), which is also a high-molecular-weight (HMW) protein, there is abundant evidence indicating that increased urine IgG concentrations in nephrotic patients could reflect activity and severity of the glomerulonephritis [13]. Recent clinical studies showed that in patients with glomerular diseases, the urinary excretion of some HMW proteins (immunoglobulins G and M) and of some low-molecular-weight proteins correlates with the severity of the histologic lesions [14]. Based on these findings, we suggest that the degree of glomerular size-barrier dysfunction reflects urinary excretion of HMW proteins, like monoclonal antibodies.
Although paraneoplastic nephrotic syndrome might result in urinary loss of the monoclonal antibody, therapeutic drug exposure was observed in this study and by others previously [12]. Different etiologies of proteinuria could be associated with differences in monoclonal antibody pharmacokinetics. In general, there are four basic etiologies of proteinuria; glomerular, tubular, overflow and post-renal proteinuria. These forms and the effect on immunoglobulin exposure will be discussed below consecutively.
Glomerular proteinuria mostly results from (chronic) hypertension and/or prolonged poor glycemic control. It is characterized by increased filtration of macromolecules across the glomerular capillary wall caused by damage to the glomerular basement membrane and podocytes [15, 16]. In these cases, the glomerular damage is often irreversible. In a patient with atypical hemolytic uremic syndrome (aHUS), variability of eculizumab pharmacokinetics was seen [17]. This was probably due to an increase in urinary drug loss as a result of progression of proteinuria. UPCR reflects urinary leakage of both intermediate MW proteins (e.g., albumin) and HMW proteins. In parallel to the increase in UPCR and drug clearance, a decline in IgG serum concentration was measured. As the chronic kidney disease progressed, proteinuria progressed [17]. The same authors investigated the effect of proteinuria on the pharmacokinetics of eculizumab in patients with aHUS. They predict that the non–target-mediated clearance in case of severe proteinuria (defined as a UPCR of > 3.1 g/gCr) will increase with 42%. UPCR was a relevant covariate for eculizumab clearance. They conclude that patients with severe proteinuria are more at risk for inadequate therapy compared with patients without proteinuria. However, this study only measured eculizumab concentrations in serum, not in urine [18]. Wehling et al. measured eculizumab concentrations in urine before and after eculizumab dosing. A significant correlation between urine eculizumab concentrations and degree of proteinuria was observed [19]. These findings indicate that severe proteinuria affects the pharmacokinetics of monoclonal antibodies, leading to urinary loss and underexposure.
Glomerular proteinuria as a result of a nephrotic syndrome is less common. Most cases of nephrotic syndrome appear to be caused by primary kidney diseases, whereas secondary causes include auto-immune diseases, malignancies or infection [3, 20]. In these examples, proteinuria may be reversed when the underlying illness is treated. Primary membranous nephropathy (pMN) and focal segmental glomerular sclerosis (FSGS) are examples of glomerular auto-immune diseases resulting in glomerular proteinuria. Studies on the pharmacokinetics of the immunosuppressive monoclonal antibodies adalimumab and rituximab, which are used in these patients, reported a lower systemic exposure in case of glomerular proteinuria. Roberts et al. observed enhanced renal clearance of adalimumab in patients with primary FSGS and nephrotic range proteinuria with up to 13% of the dose being excreted in the urine. A non-linear relationship between proteinuria and renal clearance was observed, with increase of renal clearance at UPCR of 12 g/gCr [4]. In addition, the FONT study group observed that the adalimumab exposure in these patients was about halved due to increased clearance. There was an association between the adalimumab serum half-life and the urinary protein–creatinine ratios and serum albumin concentrations. Serum half-life was shorter in FSGS patients who exhibited higher UPCRs and lower serum albumin levels, reflecting enhanced renal clearance [5]. Rituximab exposure in pMN patients was also observed to be lower, with even one study reporting that 56% of their patients had undetectable rituximab plasma concentrations at 3 months potentially due to renal loss. This negatively impacted achieving a clinical remission at 6 months. Enhanced clearance, shorter half-life, and lower exposures were demonstrated in patients with MN. Linear regression analyses demonstrated significant negative relationships between rituximab half-life and urinary protein excretion. This demonstrated that rituximab has an altered pharmacokinetic profile in patients with MN as compared to patient populations without kidney diseases [6, 21, 22].
In summary, evidence from pharmacokinetic studies of eculizumab, rituximab, and adalimumab in patients with glomerular proteinuria indicate that higher UPCRs correlate with shorter serum half-life, enhanced clearance, and lower exposure of monoclonal antibodies. All patients in the aforementioned studies had severe proteinuria (UPCR > 3.1 g/g or > 3.5 g/day). Since only a few studies have measured mAb concentrations in urine, it is challenging to estimate the variability in renal clearance or detection rates in urine based on different types of monoclonal antibodies. Inter-mAb variability in the efficiency of FcRn-mediated reabsorption has been observed, likely due to differences in the physicochemical properties of the variable regions [23]. In addition, the urine matrix may affect the detection efficiency of monoclonal antibodies, as matrix effects on assays have been reported for urinary albumin, and urea is known to exert a denaturing influence on mouse monoclonal antibodies [24, 25]
Tubular proteinuria is characterized by a diminished proximal tubular reabsorption of low-molecular-weight proteins (< 25 kDa). Under normal circumstances, small proteins can be filtered across the glomerulus and are almost completely reabsorbed in the proximal tubule. Tubulointerstitial diseases can lead to increased excretion of these smaller proteins [26,27,28]. Monoclonal IgG-based antibodies have a size of about 150 kDa. One study observed a very slight increased IgG proteinuric rate in patients with tubular proteinuria [29], to probably no clinically relevant extent. In tubular proteinuria, there is no need to anticipate loss of protein through the urine. Investigating the tubular reabsorption mechanism of intermediate (albumin) and high-molecular-weight proteins (IgA, IgG, mAbs) reveals that this process is mediated by the FcRn, along with other receptors, in the proximal tubules. In cases of an increased filtered load of these proteins across the glomerular membrane, along with defects or saturation of the FcRn, there may be an increase in their urinary elimination. The extent to which this affects the clearance of mAbs remains unclear [15].
Overflow proteinuria is also characterized by increased excretion of low-molecular-weight proteins but due to a marked overproduction of a particular protein exceeding the normal proximal reabsorption capacity. These proteins are often immunoglobulin light chains (i.e., Bence Jones proteins), in multiple myeloma but also lysozyme, myoglobin or free hemoglobin can be seen [30]. Also in this type of proteinuria, there is no need to anticipate loss of protein through the urine to a clinically relevant extent.
Finally, post-renal proteinuria is caused by inflammation of the urinary tract. Only small amounts of IgA and IgG are excreted (< 1 g/day), clinically not relevant [16, 31]. In post-renal proteinuria, there is no need to anticipate loss of protein through the urine.
To conclude, an effect on the pharmacokinetics of monoclonal antibodies is observed only in glomerular proteinuria, particularly in cases of nephrotic range proteinuria.
Importantly, aside from enhanced renal clearance, various other factors affect the pharmacokinetics of mAbs, with binding to available target (i.e., target-mediated drug disposition) being the most predominant factor [32]. Also, hypoalbuminemia is thought to be a marker for elevated protein turnover secondary to a cancer-associated chronic state of systemic inflammation. A higher endogenous catabolic rate for albumin correlates strongly with the catabolic turnover of IgG molecules such as mAbs [33]. Besides hypoalbuminemia being the result of a nephrotic syndrome, it can also be caused by a higher endogenous catabolic rate.
In conclusion, our patient, diagnosed with NSCLC and presenting a paraneoplastic nephrotic syndrome with mild nephrotic range proteinuria, did not exhibit renal loss of pembrolizumab. This was likely due to the mild nephrotic range proteinuria (UPCR 3.2 g/gCr). Measuring serum and urine drug concentrations provided valuable insights, indicating sufficient drug exposure. In patients with a paraneoplastic nephrotic syndrome, addressing the underlying cancer leads to improvements in nephrotic syndrome symptoms, as corroborated by the findings of Jansen et al. and our own findings. If possible, Therapeutic Drug Monitoring of the monoclonal antibody could be used to assure adequate drug exposure in these patients. Existing literature shows that increased renal clearance of monoclonal antibodies in patients with glomerular proteinuria is possible, but it probably depends on the amount of glomerular proteinuria. We suggest that in cases of severe glomerular proteinuria, like nephrotic range proteinuria, the likelihood of renal loss of monoclonal antibodies is higher than in other cases.


Comments (0)