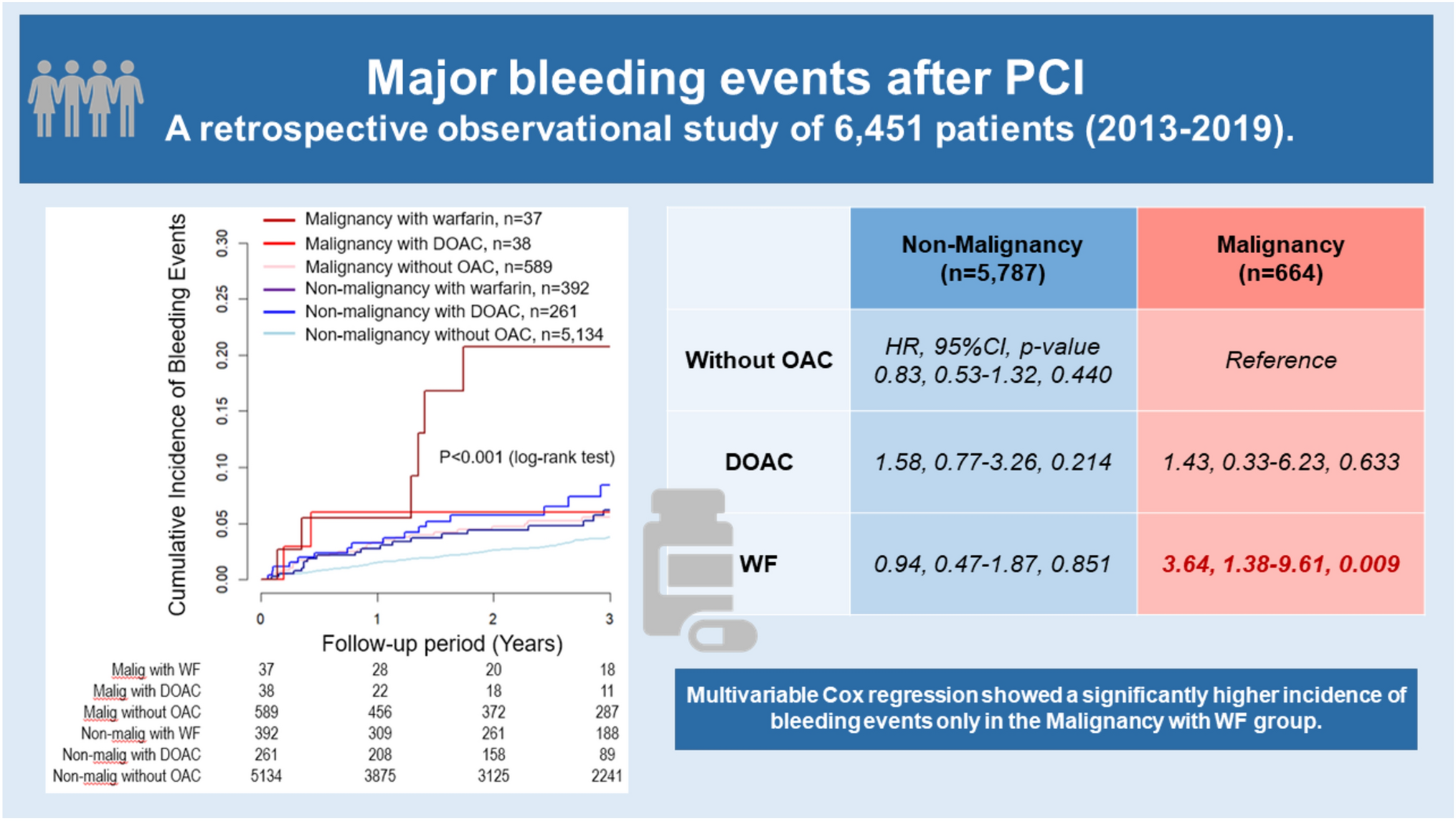
This large-scale, multicenter, observational cohort study of 6451 patients who underwent PCI during a 3-year follow-up period investigated the association between malignancy and bleeding events. Given the limited reports directly comparing DOAC and WF for anticoagulant therapy in patients with malignancy after PCI, the findings of this study provide valuable insights. Regarding the primary outcome, the present study showed that a higher incidence of bleeding events in the Malignancy group compared to the No Malignancy group, supporting the inclusion of malignancy as a HBR factor in both the ARC-HBR and Japan-HBR criteria. Moreover, patients with malignancy receiving warfarin after PCI experienced a higher incidence of bleeding events, highlighting the elevated bleeding risk associated with warfarin in this population (Graphical abstract).
The overall incidence of bleeding events was 3.3% in our cohort, consistent with the 1.6% to 7.3% range reported in previous studies [20,21,22]. In addition, the prevalence of malignancy in patients undergoing PCI was 10.3%, aligning with previously reported rates of 3.8% to 13.3% [5], [23,24,25]. Furthermore, gastrointestinal bleeding was more frequent than intracranial bleeding, a finding consistent with previous studies on post-PCI complications [26].
Further investigation is required to explore the reasons why cancer patients undergoing PCI, particularly those treated with warfarin, are more prone to bleeding events. The increased bleeding risk in cancer patients treated with warfarin may be attributed to multiple. factors. Tumor-related bleeding, hepatic dysfunction, medications, radiation therapy, malnutrition, thrombocytopenia, and disseminated intravascular coagulation (DIC) are potential contributors. Patients with malignancy had a higher incidence of bleeding events when treated with OAC compared to those without malignancy, with similar findings observed in studies specifically focused on warfarin [27, 28]. Furthermore, this population has a significantly higher rate of transfusions during the perioperative period of PCI and experience more frequent readmissions for bleeding compared to those without malignancy following PCI for AMI [29, 30]. These study findings clearly demonstrate that a malignant condition leads to an increased susceptibility to bleeding.
Warfarin metabolism relies on hepatic cytochromes P450 (CYP) enzymes, and its clearance may be impaired by hepatic dysfunction, which can be exacerbated by cancer or congestive hepatopathy following PCI [31]. This impaired clearance can lead to enhanced anticoagulant effects. Additionally, conditions such as hypoalbuminemia, common in cancer patients due to malnutrition or nephrotic syndrome, increase the proportion of unbound warfarin, further enhancing its anticoagulant effect and elevating risk of bleeding [32, 33].
Regarding anticancer agents, 5-fluorouracil, molecular targeted therapies such as gefitinib and imatinib, and anticancer drugs like tamoxifen used in the treatment of breast cancer have been reported to enhance the effects of warfarin by several reason such as inhibiting CYP enzymes [27], [34]. Optimal INR control in warfarin therapy for cancer patients is challenging in the context of cancer treatments, leading to an increased risk of bleeding and other significant cardiovascular adverse events [35]. In light of these risks, warfarin administration in patients with malignancy is associated with an increased incidence of bleeding events following PCI. The selection of anticoagulant therapy was left to the discretion of the attending physicians at each institution. In general, DOAC were favored in patients with non-valvular atrial fibrillation, preserved renal function, and no contraindications such as high-risk gastrointestinal lesions or potential drug interactions with anticancer agents. Warfarin was more often chosen for patients with advanced renal dysfunction, mechanical heart valves, or unstable coagulation profiles requiring close INR monitoring. These real-world prescribing patterns may have introduced indication confounding, as baseline characteristics and clinical complexity likely differed between the DOAC and warfarin groups. Although we adjusted for potential confounders and applied multiple imputation for missing data, unmeasured confounding cannot be entirely excluded.
In terms of the secondary outcomes, multivariable Cox regression analysis demonstrated a significantly higher incidence of MACE in the Malignancy with DOAC group compared to the Malignancy without OAC group, while no significant difference was observed in the Malignancy with WF group. Several potential explanations may account for this finding. First, some malignancies are generally associated with a hypercoagulable state through mechanisms such as tissue factor expression, platelet activation, and the release of inflammatory cytokines [36]. These biological processes can increase thrombotic risk regardless of the anticoagulant used. In this study, however, detailed information, including cancer type, stage, activity, and treatment status, was not available. Moreover, the choice of anticoagulant type was at the discretion of attending physicians, introducing the possibility of indication confounding. In clinical practice, it is also plausible that DOAC were preferentially prescribed to patients with more active malignancy or higher thrombotic risk, as supported by prior trials investigating DOAC use in cancer patients at elevated risk for thromboembolic events [37, 38]. In this context, it is conceivable that some patients in the DOAC group had a history of cancer-associated thrombosis, such as venous thromboembolism, and were prescribed DOAC accordingly. This may have contributed to the higher incidence of thrombotic events observed in the malignancy with DOAC group. In addition, variations in the duration and modification of post-discharge antiplatelet therapy may have influenced the observed differences in MACE incidence. Second, the discrepancy may be attributed to the small sample sizes in the malignancy groups treated with DOAC and WF (n = 38 and n = 37, respectively), which may have introduced that statistical variability and led to unstable estimates. Therefore, further prospective studies with larger cohorts and more detailed oncologic and pharmacologic data are needed to clarify the cardiovascular safety profile of DOAC in cancer patients undergoing PCI. Although current guidelines recommend DOAC over WF for AF, the benefits of DOAC in cancer patients, particularly in relation to thromboembolic events such as ischemic stroke, have produced inconsistent results across studies [39, 40]. Given the limited number of studies comparing OAC therapies in cancer patients following PCI, as in this study, further research with larger sample sizes is warranted to better assess MACE and NACE outcomes in this population.
This study has several limitations. First, because this was a retrospective study, selection bias and unmeasured confounding factors, such as the type, progression, treatment history of the malignancy, the duration and modification of antiplatelet therapy, and transfusion history, may have influenced the results. In particular, the CLIDAS database did not consistently capture detailed information on the continuation or discontinuation of dual antiplatelet therapy (DAPT) after hospital discharge. As previous trials (e.g., WOEST, PIONEER AF-PCI, and RE-DUAL PCI) have demonstrated that prolonged triple therapy increases bleeding risk, the lack of granular antiplatelet data is a significant limitation and may have affected the observed clinical outcomes [41,42,43]. To reduce selection bias, this study included all patients from the seven hospitals during the study period. Second, owing to the nature of the database, the definition of malignancy was based on a history of prior malignancy, which differs from the active malignancy definition used in the ARC-HBR and Japan-HBR criteria. Despite this broader definition, it is unlikely that the bleeding risks in our malignancy group were overestimated. Third, the CLIDAS database includes data from the Japanese Diagnosis Procedure Combination System, which limits the traceability following hospital transfers. As a result, some bleeding events may have been underestimated due to incomplete follow-up for patients treated at other hospitals post-PCI.



Comments (0)