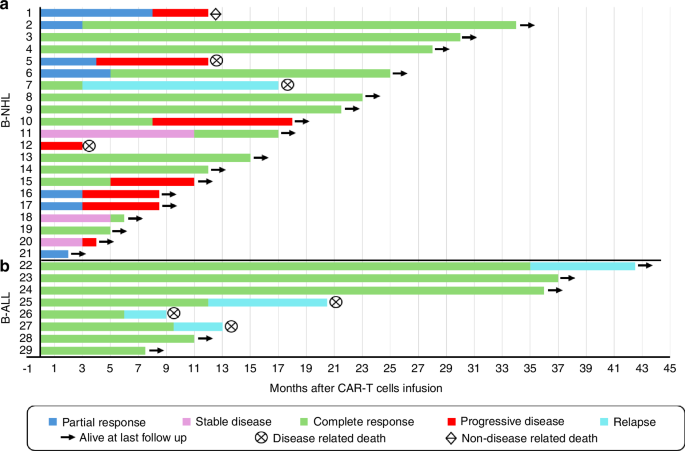
The efficacy of PP CAR-T therapy compares favorably with that of approved CAR-T products reported in pivotal registration trials. In our B-ALL cohort (n = 8), all patients achieved a complete response (CR), with 87.5% (n = 7) attaining minimal residual disease (MRD)-negative status within 1–3 months following CAR-T infusion. These outcomes are comparable to those reported in a Chinese study utilizing a 4-1BB-based CAR-T construct (CR: 90%, MRD-negative: 85%) [2], as well as with Tisa-cel, which demonstrated a CR rate of 81% with MRD negativity [1].
At median follow-up durations of 16.8 and 12 months, respectively, sustained remission was maintained in 50% of PP CAR-T-treated B-ALL patients, comparable to 59% reported with Tisa-cel [1]. All responding patients in our study developed B-cell aplasia (Table 1), consistent with findings from previous studies using Tisa-cel [1].
Three MRD-negative patients experienced disease relapse at 6, 12, and 36 months post-infusion, respectively, including one patient who relapsed with CD19-negative blasts. One patient, who achieved morphological CR but had persistent BCR-ABL positivity, underwent allogeneic HSCT but relapsed 12 months after CAR-T infusion and 8 months post-transplant. The role of allogeneic HSCT following CAR-T-induced remission in B-ALL remains a subject of ongoing debate. In our setting, the principal challenge is timely identification and procurement of suitable donors. Notably, one patient who achieved CR experienced a CD19-negative relapse after a prolonged delay in undergoing allo-HSCT and ultimately died from the relapse without receiving the transplant. In our cohort, most CAR-T responders lacked access to suitable donors. Similarly low rates of allogeneic HSCT following CAR-T therapy in B-ALL (18–22%) have been reported in other studies [6, 9].
In our B-NHL cohort (n = 21), a high overall response rate (ORR) of 81% (n = 17) was observed as early as 1 month post-infusion, including a CR rate of 57.1% (n = 12). Two patients who initially had stable disease (SD) subsequently converted to CR at 5 and 11 months post-infusion, respectively. The best ORR achieved was 90.5% (n = 19). At a median follow-up of 12 months, 52.4% (n = 11) of patients remained in CR. These response rates are comparable to those observed in a registration trial of Tisa-Cel, with reported ORRs of 53% and CRs of 39% [3].
At median follow-ups of 12 and 36 months, durable responses were achieved in 57.1% of B-NHL patients treated with PP CAR-T, comparable to 60.4% reported with Tisa-cel in the JULIET study [3]. Of note, at a median follow-up of 12.5 months, the median overall survival was not reached in both our B-ALL and B-NHL cohorts.
However, approximately one-third of B-NHL patients who initially responded experienced relapse (n = 1, 4.8%) or disease progression (n = 6, 28.6%), primarily within the first 3 months following infusion. Additionally, two patients who did not achieve an initial response experienced early disease progression. These findings are consistent with previously reported relapse and progression rates of 30–60% within the first year after CAR-T therapy [10].
Among the five patients who relapsed or progressed after PP CAR-T infusion, most exhibited high-risk features such as elevated baseline LDH, primary extranodal disease, and adverse molecular subtypes (e.g., double- or triple-expressor DLBCL). All of these patients eventually died, with a median overall survival of 8.5 months. Notably, previous studies have reported a median survival of less than six months following CAR-T failure [9]. These observations underscore the urgent need for improved strategies to enhance outcomes in high-risk patients undergoing CAR-T therapy.
A robust in vivo expansion of CAR-T cells is strongly correlated with achieving CR [1, 4]. In our cohort, peak CD19+CAR-T cell levels exceeding 10% were observed in 87.5% (7 of 8) of B-ALL patients (range: 13.7–69.61%) and in 28.6% (6 of 21) of B-NHL patients (range: 13.38–47.03%), all of whom attained an early CR. In B-ALL, peak CAR-T expansion occurred between days 7 and 14 post-infusion, whereas in B-NHL, peak CAR-T levels were observed between days 7 and 21. Among the four B-ALL patients who relapsed, CD19+CAR-T cells were undetectable by day 21 in three cases. Likewise, all B-NHL patients who experienced relapse or disease progression had CAR-T cell levels below 1% on days 21 and 28. These findings are consistent with previous reports linking insufficient CAR-T cell persistence or rapid clearance to early treatment failure [1, 4].
In conclusion, PP CD19 CAR-T therapy offers a potentially life-saving option for patients with relapsed or refractory B-ALL and B-NHL who have exhausted standard therapies. Beyond clinical efficacy, this approach addresses significant logistical barriers in resource-limited settings. Local manufacturing shortens production timelines—crucial for patients with aggressive disease—and eliminates the need for overseas shipping, thereby reducing costs while preserving safety and efficacy that appear comparable to commercial CAR-T products. Nevertheless, larger studies with extended follow-up are required to confirm and further characterize these preliminary yet promising outcomes with this locally developed CAR-T cell therapy.

Comments (0)