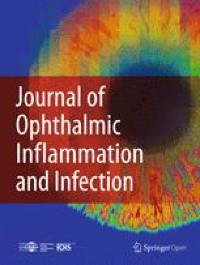
Microscopic evaluation of the corneal scrapings is one of the most rewarding and rapid methods for the etiological diagnosis of microbial keratitis aiding in early initiation of specific treatment. A large body of literature supports the application of this methodology in cornea clinics engaged in treatment of microbial keratitis patients [15, 16]. However, the limitations of the method include low sensitivity and requirement for high expertise [12]. Experience of the observer is one of the key players that determines accuracy of the results. The ocular microbiologists involved in the microscopic observation of the corneal scrapings in these cases even with their experience were uncertain about the fluorescent structures in KOH + CFW mount that resembled yeast or microsporidial spores. Some of the cells had a hyper fluorescent spot at one of the poles. An earlier study reported that, Golgi complex cluster towards one end of cell prior to cell division that might be visible as brighter fluorescent spot in KOH + CFW mount [10]. The budding seen in some of the cells were broad based and not typical of budding yeast. Usually budding yeast cells have clear budding shape similar to figure “8”, with a large mother cell and small daughter cell. Daughter cell can vary in its size based on origin, i.e., daughter cell derived from an old mother cell is comparatively larger, than the one derived from a young mother cell [17].
Normally, the KOH + CFW mount of corneal scraping is examined under 40X objective lens. Calcofluor white is a fluorescent brightener that has a high affinity to bind cellulose present in the cell wall of fungi, yeast and microsporidia. Use of CFW along with KOH increases the diagnostic positive rate, sensitivity and specificity of smear examination and simultaneously reduces the diagnostic time. A small fragment of any fungal hyphae or few yeast / Microsporidia cells can be noticed in KOH + CFW mount, that may be missed with only KOH mount. Hence, KOH + CFW has a potential value for clinical applications. In our recent experience, we saw a much clearer view of these atypical structures at higher magnification (100X objective lens in KOH + CFW mount). Therefore, we suggest the use of 100x objective lens for better visualisation of such atypical structures.
Absence of these atypical structures in corresponding Gram stain may be attributed to relatively lesser sensitivity of Gram stain compared to KOH + CFW for the detection of fungal spores and other pathogens such as Microsporidia or Acanthamoeba in clinical samples [18, 19]. It is also possible that unlike Gram stain, use of KOH causes clearing of the background tissue making these structures stand out prominently. Inability to grow in culture could be due to either low numbers of the organisms or non-viable organisms.
In recent times, molecular methods (conventional PCR, real time PCR, DNA sequencing, next generation sequencing etc.) have found their way into clinical diagnostic laboratories for detection and identification of microorganisms in clinical samples [20, 21]. They are extremely versatile and apart from accurate and specific identification, they help to recognise previously unknown organisms [22]. Strong clinical suspicion of yeast prompted us to proceed further with PCR followed by sequencing to confirm the identity of these structures as Candida spp. and Citeromyces matriensis.
Our results emphasise that KOH + CFW stain can demonstrate atypical spore like structures (with or without budding) in corneal scrapings that can be suggestive of Candida species. In absence of growth in culture they can be further confirmed by ITS targeted pan fungal PCR. The clinical importance of this understanding was shown by the fact that, out of 6 cases given antifungal therapy all cases responded to targeted treatment except one which had already extended to limbus requiring TPK.
Absence of detectable Candida DNA in all 12 corneal scraping samples, from smear and culture negative cases, suggests that Candida is unlikely to be a normal flora in the cornea and could not have been a contaminant in the samples of the eight cases reported in this series. This is in contrast to a recent report that has shown Candida DNA in normal conjunctiva by next generation sequencing (NGS) [23]. However, the difference in the sensitivity of the PCR technology in the two studies would explain the discrepancy. Using NGS for diagnosis in a clinical scenario remains far-fetched at this point in time.
Clinically, Candida keratitis may resemble bacterial keratitis [24]. Regina et al. in their study on characteristics of Candida keratitis reported that, out of 29 patients, keratomycosis was suspected in 2 patients and rest were considered bacterial keratitis [25]. Therefore, to avoid erring in favour of bacterial keratitis, we recommend increased awareness among microbiologists to report this entity for the early initiation of antifungal treatment.
In this series topical amphotericin B 0.15% was used in all except two patients for treatment. In general, its use is limited because of unavailability of ready to use topical preparation and because it needs compounding pharmacy for formulation from injectable form. It is also associated with surface toxicity leading to punctate corneal erosions, stromal edema and iritis. Therefore, topical natamycin and voriconazole are other alternatives for treating Candida keratitis [25].
The limitation of the study was its retrospective design, small sample size and involvement of several treating clinicians that may account for the final visual and functional outcomes in patients according to their clinical decisions.
We conclude that the awareness of considering round to oval shaped atypical structures, without any budding or pseudo-hyphae with a hyperfluorescent point at one of the poles in KOH + CFW mount of corneal scraping of a suspected microbial keratitis patient as budding yeast, will be helpful in clinical practice. Further confirmation can be made by fungal PCR.



Comments (0)