The comparative effectiveness of research evaluating the impact of “real world” pulmonary rehabilitation on surgical outcomes is not extensively documented. Randomized controlled trials (RCTs) have strict patient inclusion and exclusion criteria that might restrict the generalisability of the study results. Overall, in this case, matched analysis, the participants in the PR group were matched to the NR group in their demographic characteristics, BMI classification, smoking status, lung function, surgery incision, surgery side, lobe, lung resection technique, comorbidities, and other measures as presented in Table 1. The PPC and LOS showed a trend of being higher in the PR group compared to the NG group, which could be attributed to the PR group having a trend toward a higher prevalence of COPD and greater pack-year histories. Furthermore, this study revealed that the PR group had a reduction of 0.2 days of LOS compared to the usual care group (EE = − 0.20) and that reduction can potentially go up to 1.8 days (95% CI = − 1.8–1.6). Also, in the PPC, the PR group had a reduction of 60% (EE = − 0.60). In the PR group, the QoL domains, including physical functioning, dyspnoea score, and global health score, all improved 6 weeks following surgery, with a maximum improvement of more than 10 units in physical functioning and global health scores 6 weeks and 6 months following surgery, which is considered a clinically significant improvement. Patient participation in the PR program was higher before surgery than after, demonstrating that the intervention is both feasible and acceptable to patients. This increased preoperative engagement highlights the program’s ability to complement patients’ needs effectively during the pre-surgical period.
A preoperative exercise rehabilitation program, pulmonary rehabilitation, has been shown to reduce LOS and PPC and is associated with better QoL. Pulmonary rehabilitation focuses on improving respiratory function and overall health in patients with chronic lung conditions through exercise, education, and support (Spruit et al. 2013). Similarly, prehabilitation, a preparatory intervention aimed at enhancing a patient’s physical and mental fitness before surgery, has demonstrated the potential to improve outcomes and recovery (Drudi et al. 2019; Gravier et al. 2021; Ferreira et al. 2021). Furthermore, pulmonary rehabilitation reduces LOS by enhancing recovery as patients become fitter, and it reduces PPC by improving mobility, enabling more effective coughing, decreasing the likelihood of atelectasis, and enhancing overall breathing (Spruit et al. 2013; Drudi et al. 2019; Gravier et al. 2021). However, due to study heterogeneity, no firm recommendations can be made regarding the optimal exercise modality, delivery method, frequency, or preoperative duration of these interventions. Nonetheless, a preoperative exercise rehabilitation program should be considered, particularly for patients with borderline lung function or limited exercise capacity, to optimize surgical readiness and recovery.
The latter findings correlate with findings from a systemic review that showed prehabilitation was associated with decreased LOS, postoperative complications, improved objective physical functioning, and improved QoL measures in patients undergoing cardiac and vascular procedures (Drudi et al. 2019). Similarly, evidence from another systemic review has shown that prehabilitation improves PPC, exercise capacity, and QoL compared to usual care in patients undergoing non-small lung cancer resection (Gravier et al. 2021). The findings of this study and of those studies presented in the literature suggest that prehabilitation could improve surgical outcomes, including LOS, PPC, and QoL, in patients undergoing cardiac, vascular, and lung cancer procedures (Drudi et al. 2019; Gravier et al. 2021).
Interestingly, this study’s findings contradict findings from an RCT, which showed that prehabilitation had no effect on PPC and LOS in patients scheduled for non-small cell lung cancer resection (Ferreira et al. 2021). However, the same study concurred with this study’s findings in showing the impact of prehabilitation and its association with better QoL, including physical functioning following lung cancer surgery (Ferreira et al. 2021). Nonetheless, it should be noted that this RCT had a short follow-up period, a weakness that may have limited the ability to demonstrate the long-term impact of prehabilitation on QoL (Ferreira et al. 2021).
In addition, this study’s findings oppose those of a recent systemic review that examined prehabilitation for cancer patients and concluded that while some prehabilitation programs showed benefits, many did not significantly improve postoperative outcomes, including postoperative complications, LOS, and QoL compared to usual care (Meneses-Echavez et al. 2023). However, it should be mentioned that the results of this systemic review could be limited by the heterogeneous tools for outcome measurement for the study included in the review (Meneses-Echavez et al. 2023).
Our analyses faced certain limitations typical of observational studies; the results may not be applicable to other major surgeries, different populations, or various settings. Additionally, the uneven availability of PR across sites could introduce site-related bias, as the outcomes observed in patients receiving PR might not be generalisable to those from non-PR sites or to the broader patient population. This limited accessibility could also affect the representativeness of the study sample. Furthermore, the widespread implementation of PR faces multiple barriers, including resource constraints such as funding, infrastructure, and trained personnel, particularly in rural areas, as well as patient adherence challenges such as logistical difficulties, low motivation, and competing medical priorities (Spruit et al. 2013). Inadequate referral pathways, sociocultural factors, and the absence of long-term follow-up further limit accessibility and effectiveness, highlighting the need for targeted interventions to improve enrolment and adherence (Spruit et al. 2013).
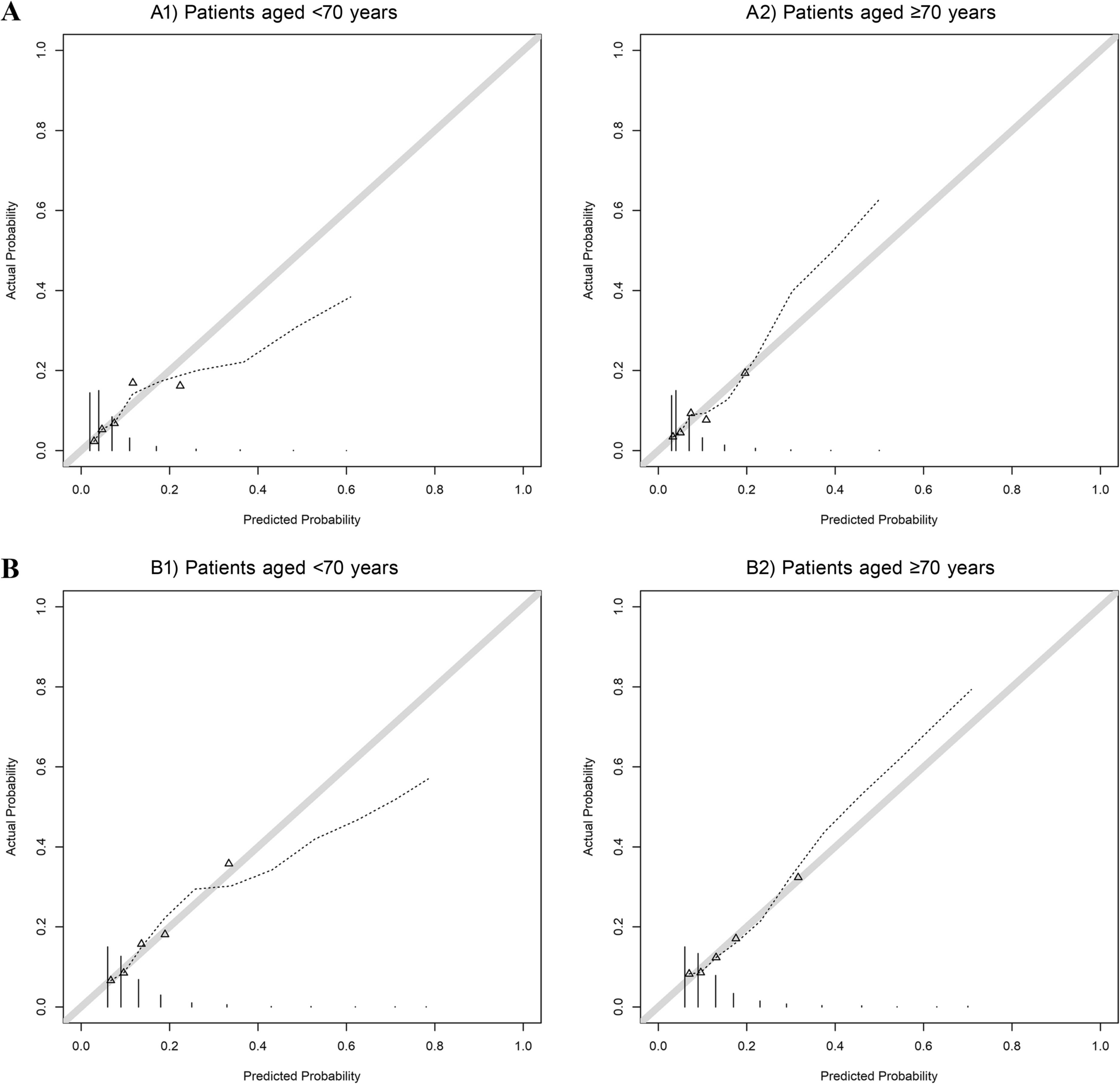
While propensity score analysis (PSA) was employed to minimize confounding and improve the comparability of groups, the potential for unmeasured confounding remains a limitation. Certain variables, such as patient motivation, informal caregiver support, or individual clinician practices, may not have been fully accounted for, which could influence both engagement in PR and postoperative outcomes. Despite the use of robust analytical methods, residual confounding cannot be entirely ruled out, and future studies with additional adjustments for such factors may provide further insights into the true impact of PR.



Comments (0)