
Remember me
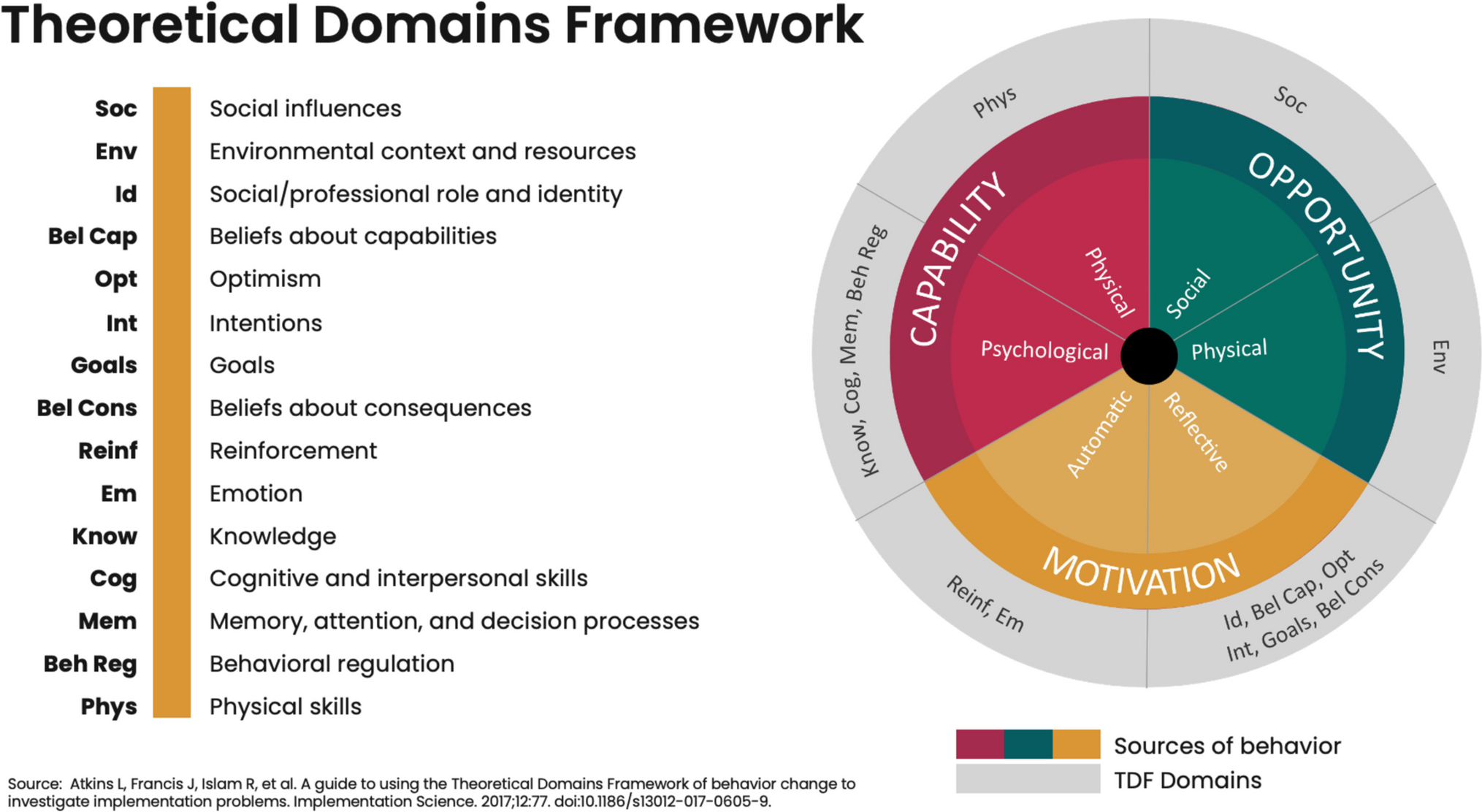


Existing literature offers insights into confirmed and hypothetical factors likely to affect women’s use of CAB PrEP once it is widely available in African markets. These insights are organized along the COM-B model and TDF in Fig. 3.
Fig. 3 1.) Capability [knowledge, memory, attention, decision processes].Confirmed Factors
1.) Capability [knowledge, memory, attention, decision processes].Confirmed FactorsConfirmed capability factors include an individual’s prior familiarity with injectable contraceptives: an ability to use injectables for pregnancy prevention is considered an enabling factor for women to use CAB PrEP [16, 17]. Furthermore, end users believe that CAB PrEP simplifies the PrEP regimen (CAB is injected every two months compared to taking a daily pill). Unlike oral PrEP, which has to be carried with the user if they are mobile or traveling, CAB PrEP offers greater perceived ease in adherence, which is another confirmed factor [18,19,20,21].
Hypothetical FactorsA lack of knowledge and awareness of CAB PrEP as a long-acting HIV prevention method may act as a barrier to initial uptake and use. Information, education, and communication (IEC) materials may facilitate awareness and knowledge-building, which could ease this barrier and promote uptake of CAB PrEP [22]. High-quality materials may also help facilitate community sensitization and greater acceptance among key influencer groups of women end users, as well as correct myths and misinformation, which can be barriers [22,23,24,25]. Based on lessons from oral PrEP rollout, client- and provider-facing behavior change communication materials should emphasize the high efficacy and convenience of CAB PrEP, provide information on various PrEP options in non-technical language, and answer frequently asked questions [4]. Appointment reminders may also help facilitate continued use [4, 23].
2.) Opportunity [social influences, environmental context, and resources].Confirmed FactorsCAB PrEP offers users discretion. Unlike oral PrEP, it does not need to be carried around, stored covertly in households, or used in settings where partners or family members may observe use.
[16, 19, 20, 26,27,28]. CAB PrEP’s discreet nature helps prevent potential negative social consequences of unintentional PrEP disclosure. Concerns about and belief in myths about the harms of CAB PrEP, including that it causes infertility, changes in DNA, and/or cancer, are examples of negative perceptions in the minds of young women’s parents, guardians, and fellow community members that are barriers to use [29]. The presence of choice has been shown to increase uptake of all available PrEP methods, including CAB PrEP [30].
Hypothetical FactorsThe effect of task sharing among healthcare personnel has yet to be formally explored, but studies posit that having injections administered by a range of healthcare cadres (including community, lay, and peer providers) and not exclusively by clinical physicians may result in less stigmatized services and reduce pressure on the health system [18, 23, 31, 32]. Similarly, offering CAB PrEP in a range of settings, including those outside traditional health facilities (e.g., pharmacies, food banks, schools, and mobile health units), could increase client reach, lower the burden of travel associated with traditional health settings, and destigmatize services [23, 31,32,33,34,35]. The integration of CAB PrEP services with other sexual and reproductive health (SRH)-related services could also act as a facilitator by reducing the number of clinic visits and travel costs for clients while easing the burden on the health system [4, 23, 25, 36, 37]. Finally, offering CAB PrEP at no charge to users and investing in healthcare provider training that focuses on correct administration of injections and nonjudgmental informed choice counseling could further facilitate uptake and continued use of this method [4, 18, 23, 24, 31, 38, 39]. On the other hand, barriers related to opportunity include potential supply chain issues, like CAB PrEP stockouts, cold chain requirements, or lack of sufficient needles [6, 18, 23, 33, 37, 40]. Where there is not a designated space in which to administer injections, women may find this lack of privacy to be a barrier [18, 23, 33, 36].
3.) Motivation [social/professional role and identity, beliefs about consequences, emotion].Confirmed FactorsThe perceived high efficacy of CAB PrEP to prevent HIV in most cases is extremely meaningful for women [16, 19,20,21, 27, 28, 34]. For some, this perception is due to beliefs that injections are more effective than other forms of medication; for others, it is because CAB PrEP becomes effective quickly after administration [17, 20, 40,41,42,43]. CAB PrEP users also appreciate that the method is not potentially disruptive to sex, unlike other HIV prevention methods.
One study conducted in several countries in SSA found that women who chose CAB PrEP over oral PrEP appeared to be at higher risk of HIV because they were less likely to live with a partner and more likely to have experienced recent physical intimate partner violence and/or to have been paid for sex [21, 27, 28, 41]. In these instances, a non-disruptive method was preferred. Overall, CAB PrEP was found to be tolerable, with no discontinuation of product use due to adverse events and a general acceptability of the needle size (1 1/2 inch) and site of administration (gluteal muscle) [16].
However, a dislike or fear of needles as well as concern about possible side effects, including injection site pain, injection site reaction, nausea, headaches, and dizziness, should be noted as factors that act as barriers to CAB PrEP use [17, 19,20,21, 26, 27, 37, 39]. For some women, the CAB PrEP injection is seen as irreversible due to its systemic nature, which is a barrier [19, 26, 27]. In addition, desire for pregnancy arose in research as one reason some may not opt for CAB PrEP. Some concern exists about its safety and efficacy profile for pregnant and/or breastfeeding women because it is not yet approved for use by this population in all countries [39].
Hypothetical FactorsThe belief that CAB PrEP prevents HIV from all types of sexual exposures may facilitate use [22, 44]. Requiring CAB PrEP to be administered by a provider and not by the user may cause end users to perceive CAB PrEP as safe because administration by a professional would ideally reduce chances of mistakes, thereby facilitating use [35, 42]. However, required administration by a provider could also create a sense of loss of independence and/or control in relation to HIV prevention medication use, which may act as a barrier [23, 25, 35]. Evidence from clinical trials found acceptability among women with the site of CAB PrEP administration; but hypothetical findings suggest that some may experience discomfort with the injection site, resulting in the perception that CAB PrEP injections are invasive [18].
The risk of developing drug-resistant HIV after stopping CAB PrEP or perceived difficulty of CAB PrEP discontinuation may be barriers to use, but this has yet to be confirmed. (In some settings, guidelines dictate that oral PrEP be taken for a period of time after CAB PrEP use stops and may be used between missed doses of CAB PrEP; this is known as “oral bridging” and may be difficult for those who already have continuation challenges with oral PrEP) [31,32,33, 35, 42, 45, 46].
4.) Key Remaining GapsFurther consideration and formative work are needed to address gaps in our understanding of women’s capability, opportunity, and motivation to use CAB PrEP. Our understanding of end-users’ motivation is particularly limited, and we do not yet fully understand some aspects of their capability. Figure 4 illustrates key gaps in the literature along the COM-B model and TDF.
Fig. 4
COM-B + TDF coverage and gaps
Future efforts should endeavor to address research questions that speak to the capability, opportunity, and motivation of women in SSA to use CAB PrEP. Knowledge gaps must be identified and addressed; in particular, greater communication efforts are needed to mitigate the spread of misinformation about CAB PrEP on issues such as its effectiveness, the consequences of stopping CAB PrEP, and potential drug resistance. Equipped with the right information disseminated through channels with reach and influence, women in SSA may be more prepared to take up and use PrEP to stop the spread of HIV.
More work is needed to understand which factors affect women’s decision-making process when deciding whether or not to use PrEP generally and CAB PrEP specifically. Women are not a homogenous group, so the role of influencers must be explored to determine their impact on women’s decision to use CAB PrEP or not. For example, an understanding of the utility of peer-to-peer motivation is required to gauge what kind of user and influencer testimonials are most compelling. Exploratory work should be focused on the type of messages, specific communication strategies, and tactics implemented across a variety of channels that will be most successful in motivating women to seek out and adhere to CAB PrEP and HIV prevention services. Finally, researchers should explore whether CAB PrEP can be positioned in a manner that affirms control for the user—what are the unexplored emotional drivers behind women’s choice to use CAB PrEP?
To date, CAB PrEP has not yet been widely available in SSA and has been exclusively available in clinical and implementation study settings, with wider rollout expected in the future. Therefore, most of the available findings concerning drivers of CAB PrEP uptake and use are hypothetical, derived from formative research conducted through studies and projects that do not include product use outside of clinical and implementation study settings. Much of this work also took place prior to any national or large-scale rollouts of CAB PrEP in the general market. An opportunity exists to answer vital research questions as CAB PrEP becomes available to women in real-life rollout settings.
Comments (0)