
Remember me




The first study had a number of pre-registeredFootnote 1 research questions and hypotheses:
RQ1: How does general self-concept differ between a population with and without DCD and is this influenced by diagnosis status? (Here, when we talk about self-concept, we are referring to the valence and importance of identities in the form of ‘I am’ statements). Given the limited findings from previous studies, which focus on children and use different methods (Cocks et al., 2009; Yu et al., 2016), it is difficult to make a clear directed prediction; however, we would expect the overall valence of statements to be more negative within the DCD population.
RQ2: Within a DCD population are identities relating to their DCD seen as positive or negative and what importance do individuals place on these? Does this differ regarding diagnosis status and does it link to age of diagnosis? Although previous studies have examined general self-concept in DCD (Harris et al., 2021), this is the first study to ask for identities relating to DCD so it is difficult to know whether these will be positive or negative.
RQ3: How do anxiety, depression, life satisfaction, and wellbeing differ between a population with and without DCD and is this influenced by diagnosis status? In line with previous research, we would expect to see a higher level of anxiety and depression and a lower level of life satisfaction and wellbeing in our group with DCD compared to the group without. However, how this is influenced by diagnosis or age of diagnosis remains to be seen.
RQ4: Is there a relationship between elements of self-concept (e.g., importance and valence), anxiety, depression, life satisfaction, and wellbeing? How does this relationship differ, for the DCD group, when considering identities in relation to their DCD? How does it relate to diagnosis status? We would expect to see positive relationships between self-concept valence and life satisfaction and wellbeing (more positive identities related to higher well-being) and negative relationships between identity valence and depression and anxiety (more positive identities related with lower depression and anxiety). The relationship between identity importance and wellbeing will also be explored. As this is the first study to specifically ask for identities relating to DCD, it is difficult to know how this will change the relationship.
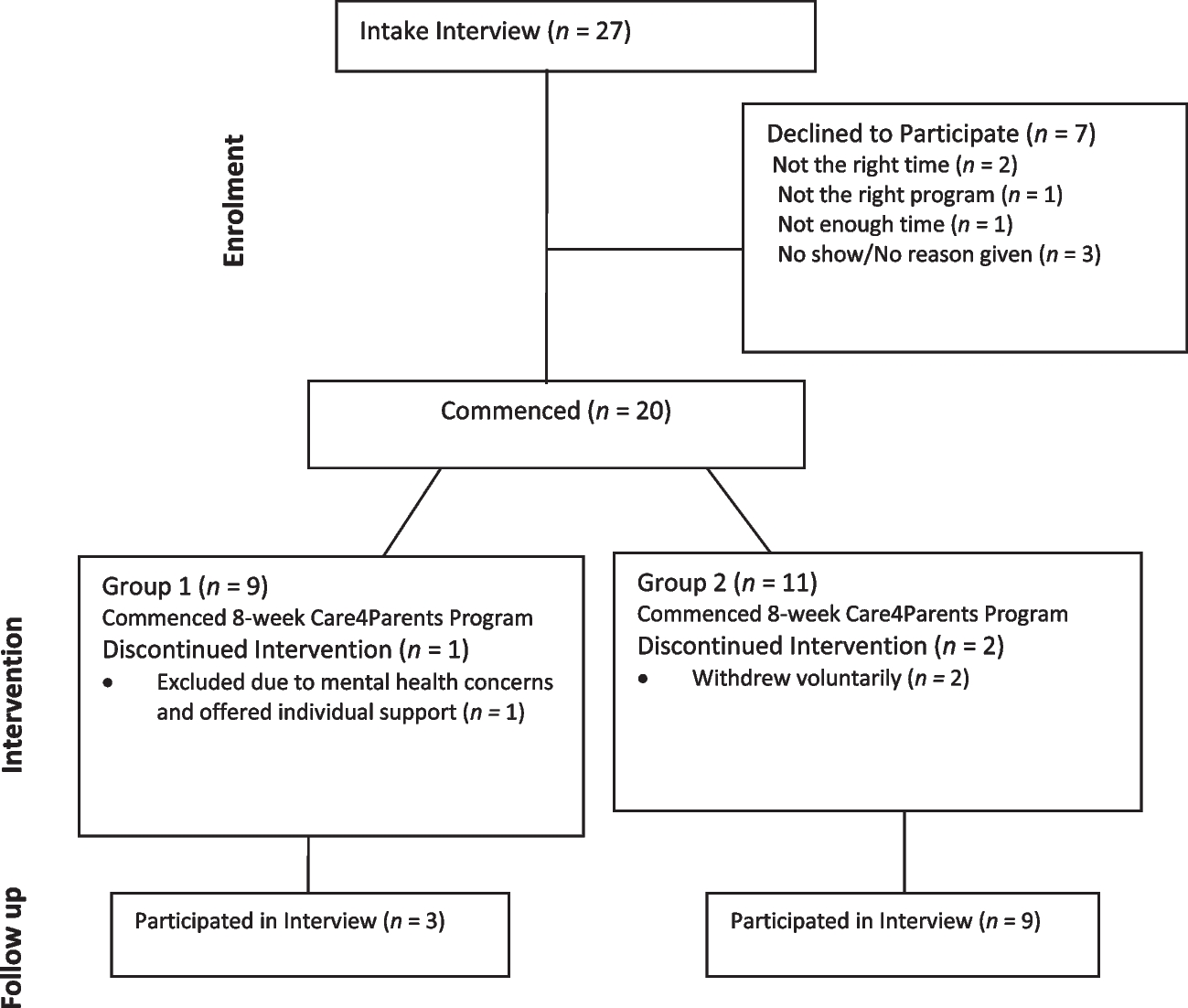
MethodParticipants105 adults diagnosed with DCD (dDCD), 52 adults with self-identified DCD (sDCD) and 53 adults without DCD (non-DCD) submitted their data. However, exclusions were made under the following criteria: 1. providing nonsense identity statements (dDCD = 1); 2. not providing full details for general identity statements (dDCD = 3, sDCD = 1); and 3. not providing chronological age (dDCD = 4, sDCD = 3, non-DCD = 4). Details of the remaining participants can be found in Table 1 which also contains details of participants for study 2. A further five participants (3 dDCD, 2 sDCD) did not provide full details for the DCD-specific identity statements. These participants were retained in the overall cohort but excluded for analyses using those variables. This was an online study and participants were recruited in a number of ways namely, through the author’s database of participants willing to take part in research, through social media (i.e., Twitter, now re-named X), via the Dyspraxia Foundation and via other personal contacts of the authors. Ethical approval for this study was granted by Oxford Brookes University Research Ethics Committee (Ref No: 191352).
Table 1 Group characteristics for study one and study twoProceduresParticipants were presented with the sections of the questionnaire as they are described above. In addition, participants indicated whether they were diagnosed with DCD, had self-identified DCD, or did not either have diagnosed or self-identified DCD, allocation to groups was done on the basis of their answer to this question.
MeasuresThe online questionnaire consisted of five distinct sections as described below, a full copy of the questionnaire can be found under the OSF project page as cited above.
Self-ConceptParticipants were asked to provide up to 10 ‘I am’ statements and then also rate each one in terms of its importance (from 1, not at all important to 10 very important), its valence (− 5, very negative to + 5, very positive) and also the age at which it emerged (i.e., the age the participant was when that self-concept became a defining part of their identity). These statements were freely-generated (not selected from a list) and thus enabled participants to describe their identity in their own words. They included reference to a range of identities including social (e.g., ‘I am a sister’), physical (e.g., ‘I am tatooed’), and psychological (e.g., ‘I am caring’) self-concepts. Participants who had indicated they were either diagnosed with DCD or self-identified they had DCD were also asked to generate up to three DCD related ‘I am…’ statements also providing importance, valence and age of emergence for each. Mean values of importance and valence were taken for both types of identity statement (general and DCD-related). These are not standardised scales but are based on the widely used Twenty-Statements Test (Kuhn & McPartland, 1954) and IAM Task (Rathbone et al., 2008).
Wellbeing Scales: Generalised Anxiety and DepressionThese were measured using the Hospital Anxiety and Depression Scale (HADS; Zigmond & Snaith, 1983). This consists of 14 questions, each rated on a 4-point scale (from 0 to 3), which ask participants to choose the statement which most closely relates to how they have been feeling over the past few weeks. An overall anxiety and an overall depression subscale score were determined by summing relevant questions. For both subscales, a score of ⩾8 is used to indicate possible cases and ⩾11 to indicate valid cases (Zigmond & Snaith, 1983).
Life SatisfactionThis was measured with the standardised Satisfaction with Life Scale (SWLS; Diener et al., 1985) which requires participants to respond to 5 questions using a 7-point scale (7 strongly agree to 1 strongly disagree). Responses were summed to provide an overall score. The scale has high internal consistency and high temporal reliability (Diener et al., 1985), with higher scores indicating a higher satisfaction with life.
General WellbeingGeneral wellbeing was measured using the standardised 18-item Psychological Well-being (PWB) scale (Ryff & Keyes, 1995). This scale asks participants to rate 18 items on a 7-point scale (1, strongly agree to 7 strongly disagree). Appropriate questions were reverse coded and then the responses summed. Higher scores indicate higher psychological wellbeing.
DemographicsParticipants were asked to provide their age in years, their gender, any formal or self-identified diagnoses of DCD/Dyspraxia (where appropriate we asked for age at diagnosis) along with any other developmental difficulties they have experienced (and age at diagnosis/self-identified diagnosis).
Statistical AnalysisOne- and two-way ANOVAs were used to investigate differences between groups and identity types while Spearman correlations were used to look for relationships. Where multiple correlations were conducted, a Bonferroni adjustment for the number of comparisons was made. A regression analysis was used to investigate factors predicting wellbeing. Bayes factor is reported throughout and was investigated via the JASP package using default priors. A model average was given for F tests (ANCOVAs and regression) and is represented as bayes inclusion (BFinc), for correlations a BF10 value is provided. Values above 3 were taken as evidence of a significant effect with cut-off point for different degrees of strength (in line with the standard classifications > 100 is taken as “extreme evidence,” 30–100 is taken as “very strong evidence,” 10–30 is taken as “strong evidence,” and 3–10 is taken as “moderate evidence”). Values between 0.33 and 3 are taken as no evidence of either a significant or a non-significant effect. Values below 0.33 is taken as evidence for a non-significant effect (0.10–0.33 is moderate evidence, 0.033–0.33 is strong evidence, 0.01–0.033 is very strong evidence, and values below 0.01 extreme evidence). These values are in line with those suggested by previous research studies (Lee & Wagenmakers, 2013). Q-Q plots were checked prior to all statistical analyses (where appropriate).
ResultsRQ1: How Does General Self-Concept (Valence and Importance) Differ Between a Population with and Without DCD and is this Influenced by Diagnosis Status?Data concerning the valence and importance of the general ‘I am’ statements can be found in Fig. 1. One-way ANOVA found a significant group effect of valence (F(2,191) = 4.58, p = 0.009, partial η2 = 0.05, BFinc = 3.56). Post-hoc tests with Tukey correction found that this was due to lower valence (more negative) from the individuals with diagnosed (p = 0.012, BFu = 0.130) and self-identified DCD (p = 0.025, BFU = 0.175) compared to the non-DCD individuals, no difference was found between the two DCD groups (p = 0.98, BFu = 5.238). No effect was found for importance (group: p = 0.092, BFinc = 0.456).
Fig. 1
Violin plots for the general valence and importance data shown across group. The mean value is represented by a black square
RQ2: Within a DCD Population are Identities Identified by the Participant as Relating to DCD Seen as Positive or Negative and how Important are these? Does this Differ Regarding Diagnosis Status and Does it Link to Age of Diagnosis?Footnote 2The relationship between importance and valence of DCD statements was initially explored in each group by running correlations between these variables (and between age of diagnosis for the dDCD group only). For the dDCD group, a significant positive correlation was found between the valence of the DCD specific statements and the importance of those statements, the more positive an identity the more importance it carried (N = 97, ρ = 0.345, p < 0.001, BFinc = 196.738). The same correlation was not significant for the sDCD group (p > 0.05, BFinc = 0.309). In addition, no significant correlations were seen between age of diagnosis and DCD specific valence (p > 0.05, BFinc = 0.130) or DCD specific importance (p > 0.05, BFinc = 0.172) in the dDCD group.
As the participants with DCD completed two different types of self-concept statement, a comparison of these as well as group was considered for both valence and importance using two-way ANOVA comparing group (dDCD vs. sDCD) and type of I am statement (DCD-specific vs general statements). Data can be found in Fig. 2. For valence, extremely strong evidence was found for a significant difference across statement type (F(1,142) = 169.87, p < 0.001, partial η2 = 0.545, BFinc = ∞) which was due to more negative DCD-related statements compared to the general statements. A significant interaction between group and statement type was also found (F(1,142) = 4.89, p = 0.029, partial η2 = 0.03, BFinc = 2.43). The interaction is explained by the non-significant difference for the dDCD compared to the sDCD group for general statements (see above) but that the sDCD group attributed a significantly more negative valence to DCD-specific ‘I am’ statements compared to the dDCD group (F(1,142) = 5.10, p = 0.025, partial η2 = 0.04, BFinc = 1.88). However, do note that Bayesian analysis suggests insufficient evidence to conclude either a significant or a non-significant effect.
Fig. 2
Graphs depicting the interaction between the type of statement given (general or DCD specific) and group (dDCD or sDCD). Self-concept valence data are provided on the left and importance on the right. The error bars represent standard error
For importance, a main effect of importance type was significant (F(1,142) = 47.52, p < 0.001, partial η2 = 0.25, BFinc = 3.10 × 106), with general statements rated as more important than DCD-specific ones. The main effect of group was not significant for either valence or importance (valence, group p = 0.106, BFinc = 1.08, importance, group p = 0.149, BFinc = 2.50). There was also strong evidence of a significant interaction between group and statement type (F(1,142) = 8.33, p = 0.005, partial η2 = 0.06, BFinc = 8.70). The interaction is explained by lack of a significant difference for the dDCD compared to the sDCD group for general statements (see above) but that the sDCD group attributed less importance to DCD-specific statements compared to the dDCD group (F(1,142) = 5.63, p = 0.019, partial η2 = 0.04, BFinc = 2.38). These data are depicted in Fig. 2.
RQ3: How do Anxiety, Depression, Life Satisfaction, and Wellbeing Differ Between a Population with and Without DCD and is this Influenced by Diagnosis Status?Data from the well-being measures can be seen in Table 2. One-way ANOVAs (group) were used to investigate the presence or absence of group effects. A significant group effect was found for HADS anxiety (F(2,191) = 5.26, p = 0.006, partial η2 = 0.052, BFinc = 4.91) and PWB total (F(2,191) = 6.40, p = 0.002, partial η2 = 0.063, BFinc = 13.5). Indicating strong evidence for group differences for these factors. For HADS anxiety, the difference lay between the DCD groups and the non-DCD group (dDCD > non-DCD, BFu = 6.21, sDCD > non-DCD, BFu = 10.446, sDCD = dDCD, BFu = 0.224). The same pattern of results was found for the PWB total (dDCD < non-DCD, BFu = 33.665, sDCD < non-DCD, BFu = 3.597, sDCD = dDCD, BFu = 0.191). No group effects were seen for HADS depression (p = 0.058, BFinc = 0.701) or SWLS (p = 0.077, BFinc = 0.517), although in both cases Bayesian analysis suggests insufficient evidence to conclude either a significant or a non-significant effect.
Table 2 Scores from the SWLS, HADS anxiety, HADS depression, and PWB questionnaires, given for each group. Standard deviation is given in bracketsRQ4: Is there a Relationship Between Elements of Self-Concept (e.g., Importance and Valence), Anxiety, Depression, Life Satisfaction, and Wellbeing? How does this Relationship Differ, for the DCD Group, when Considering Identities in Relation to Their DCD and Diagnosis Status?Footnote 3Relationships between self-concept (valence and importance for both general and DCD specific statements) and measures of wellbeing (these were only done for the HADS anxiety and PWB scores as it was these which demonstrated a group difference) were explored using Spearman correlations for each group separately (for the dDCD group age of diagnosis was included). The outcome of these correlations is in Table 3.
Table 3 Spearman correlation coefficients, p values, and BF10 values for relationships between the identity measures (valence and importance) and the measures of wellbeing (PWB and HADS anxiety)Finally, in order to consider the predictors of wellbeing in DCD, we conducted regression analysis on the DCD groups only. To do this, we used the PWB measure as it yielded stronger relationships between it and the valence of identities compared to anxiety. Variables which were added to the regression included valence and importance measures (both general and DCD-specific), group, and chronological age. Prior to analysis assumptions, checks were conducted. Durbin-Watson test was non-significant (p = 0.274) indicating auto-correlation of errors, tolerance values were all above 0.813, thus not approaching zero, the Q-Q plot indicated close clustering of residuals to the line, demonstrating normal distribution of residuals and the residual plots suggested random distribution. All of these checks suggest assumptions were met and so the outcome of the regression analysis is reliable (Tabachnick & Fidell, 2007).
A significant regression model was found F (6,137) = 7.02, p < 0.001, Adjusted R2 = 0.202. Both measures of valence (for general and DCD-specific self-concepts) were significant predictors. Group (dDCD or sDCD), age, and the two measures of importance were not significant predictors. Coefficients can be found in Table 4.
Table 4 Regression coefficients when considering factors which predict wellbeing in the DCD groups onlyDiscussion from Study OneThis first study had four specific research questions which focused on the nature of general self-concepts in those with DCD compared to those without, the nature of DCD specific self-concepts in those with DCD, differences in wellbeing measures across those with and without DCD, and finally, the relationships between self-concepts and wellbeing. In terms of general self-concepts, these were shown to be more negative in those with diagnosed DCD compared to their peers without DCD. There was evidence, albeit weak, that the general self-concepts of those who self-identify as DCD were also more negative compared to their peers. This finding is in line with previous work which has shown that children with DCD report a greater degree of negative self-concept compared to their peers (Cocks et al., 2009; Yu et al., 2016). This is the first study which has considered the emotional valence of identity in adults with DCD. The finding that those self-concepts were no less important in the DCD population, despite their increased negativity, may explain the poor outcomes in terms of wellbeing which characterise this population. However, despite the non-significant p value Bayesian analysis suggests a lack of evidence to support a conclusion that there were no differences between the importance of those general identities (Lee & Wagenmakers, 2013).
When we compare within the DCD groups across the general and the DCD specific identities, we see strong evidence that the DCD-specific identities are seen more negatively and as less important compared to the general identities. There was also evidence that the DCD-specific statements were more negative, but carried less importance in the sDCD group compared to the dDCD group. This finding fits with both the self-enhancement literature (i.e., if something is bad then it is not that central to who I am, e.g., Alicke & Sedikides, 2009) and also previous work on children with DCD which has demonstrated that negative self-concepts tend to carry less importance (Hands et al., 2020). However, it is important to note that when asked for what we have referred to as ‘general’ statements the participants were not explicitly told not to think about or refer to their DCD and some of the participants did refer to their DCD in these ‘general identities’ suggesting that these ‘general’ identities may be diluted by those related to DCD.
When considering wellbeing levels, we have demonstrated significantly higher anxiety levels and poorer levels of wellbeing in adults with DCD compared to their peers. Both of these factors have been found previously (Harris et al., 2021; Hill & Brown, 2013; Hill et al., 2011; Tal Saban et al., 2014) but this is the first study to provide strong evidence that there are no differences in any of the wellbeing measures across the diagnosed DCD group and the self-identified DCD group. Furthermore, we have provided strong evidence that the valence of the self-concepts (both general and DCD specific) are not related to the age of diagnosis. This seemingly goes against previous research which indicates that a diagnosis of ADHD and of autism can support self-concept and thus wellbeing (O’Connor et al., 2018; Wilson et al., 2023) and that an earlier diagnosis of DCD and of autism would support self-concept and wellbeing (Cleaton et al., 2021; Wilson et al., 2023). It is worth bearing in mind that DCD is underrecognised by healthcare professionals (Meachon et al., 2024), teachers (Bidwell, 2022), employers (Doyle, 2020), and wider society (Steenbergen et al., 2024). Therefore, even with a diagnosis, the support received during childhood and adulthood may simply not be sufficient to benefit those with a diagnosis over those without (Steenbergen et al., 2024). However, one limitation of our study is that we did not collect data considering the motor skills of our dDCD and sDCD groups so we cannot be sure that these groups are equivalent in terms of their experiences of DCD symptomology.
In comparing the valence of general and DCD-specific statements to wellbeing measures, we have demonstrated strong evidence that the valence of both general and DCD-specific statements are related to psychological wellbeing. In delving into this a little further, when considering factors which might predict wellbeing, we have seen strong evidence that both general and DCD-specific valence of identities predicts wellbeing, whereas diagnostic status does not. Once again, this may suggest that it is not as simple as a diagnosis supporting wellbeing, but rather, in line with previous work, that diagnosis can result in a range of emotions (Williams et al., 2015). This is also supported by a systematic review which found evidence showing an association between positive autistic identity and improved mental health and wellbeing (Davies et al., 2024). Therefore, suggesting that the links between identity and wellbeing which we have found here are not isolated to this population. Finally, Bayesian analysis suggests no evidence of a non-significant effect in terms of the importance of the DCD-specific statements and their relation to wellbeing.
Above, we have highlighted the mixture of strong and inconclusive evidence and also some limitations to study one, namely, the dilution of ‘general’ identity statements with mention of DCD and no information regarding the comparability of the dDCD and sDCD group in terms of symptomology. Therefore, we conducted a second study which only considered individuals with DCD and included a screening questionnaire for motor skills. We chose to focus only on participants with DCD in study 2 as we wanted to explore in detail the memories that might underpin DCD-related self-concepts. The primary objectives of this second study were to replicate the findings above, to collect data on identities while specifically asking for those that do or do not relate to DCD and to examine the autobiographical memories associated with the self-concept participants define themselves with.
Comments (0)