
Remember me




Between May 2007 and November 2021, four patients (men, 75%; median 57 years, range 43–66 years) were referred for percutaneous biliary neo-anastomoses at a tertiary care center including liver transplant.
History, etiology, indication as well as procedural details for percutaneous biliary neo-anastomoses are reported in Table 1.
Table 1 Patient characteristics and technical issuesThe indication for percutaneous biliary neo-anastomosis was made by a multidisciplinary board involving hepato-biliary-pancreatic surgeons, gastroenterologists and interventional radiologists.
Two of the four patients with leaking posterior right ducts were recipients of living-donor right hemi-liver transplants, which had been performed for hepatocellular carcinoma in cirrhotic livers. In two patients, major resections for biliary and pancreatic cancers had been performed. Three patients presented with peritonitis related to free intraabdominal bile leakage, and one patient had developed an extrahepatic biloma with recurrent septicemia.
All procedures were performed under local anesthesia and moderate sedation. Pre-procedural cross-sectional imaging (both CT and MRI) was reviewed. Attention was paid to perihilar vascular structures (hepatic artery, portal vein) in proximity to the planned neo-anastomosis. The excluded leaking bile duct had been identified on pre-procedural cross-sectional imaging, at fluoroscopy of indwelling biloma drains or percutaneous biliary drains (PTBD) placed via any other duct.
Two techniques were utilized to perform the percutaneous biliary neo-anastomosis (PBNA). Both techniques aimed at creating a new connection between an excluded posterior right duct and an intestinal loop (n = 3, Fig. 1) or the common hepatic duct (n = 1, Fig. 2). Technical success was defined as an established connection without any leakage.
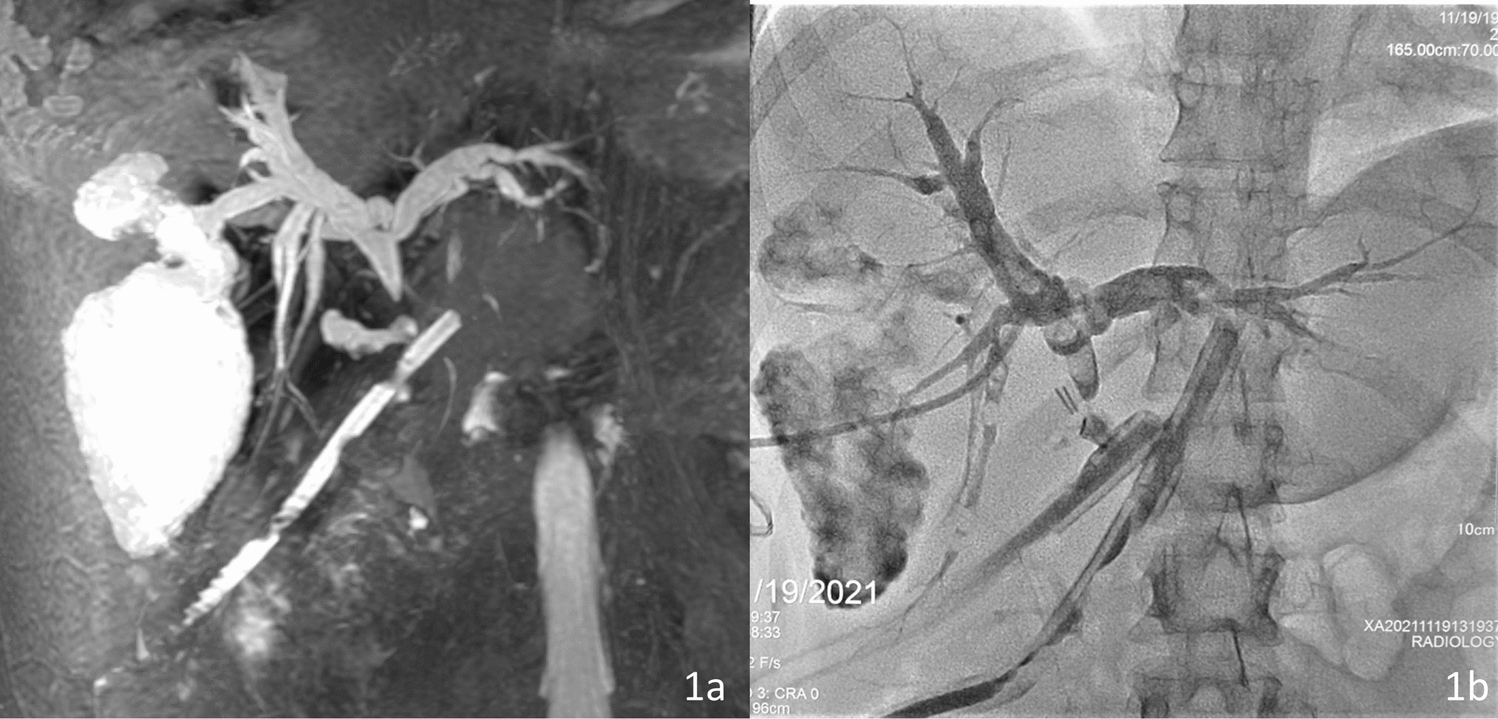
Fig. 1
A 66-year-old female with adenocarcinoma of the pancreatic head (patient 3). Twelve days after Whipple’s procedure she presented with fever. a Transhepatic cholangiography shows a leak from the excluded right posterior sectoral duct (arrowhead). b A PTBD was placed via the right anterior ducts to opacify the small bowel loop to be accessed. A 8F sheath and a 4F Kumpe catheter were percutaneously advanced through the excluded posterior right duct. Penetration of the small bowel loop was achieved with the backend of a 0.018″ guidewire (arrowhead). c The newly created bilio-enteric anastomosis was secured with an 8.5F PTBD (arrowhead). d At removal of the PTBD, approximately 3 months after the intervention, there is proper flow of contrast agent through the bilio-entero-neo-anastomosis into the small bowel (arrowheads) without bile leakage
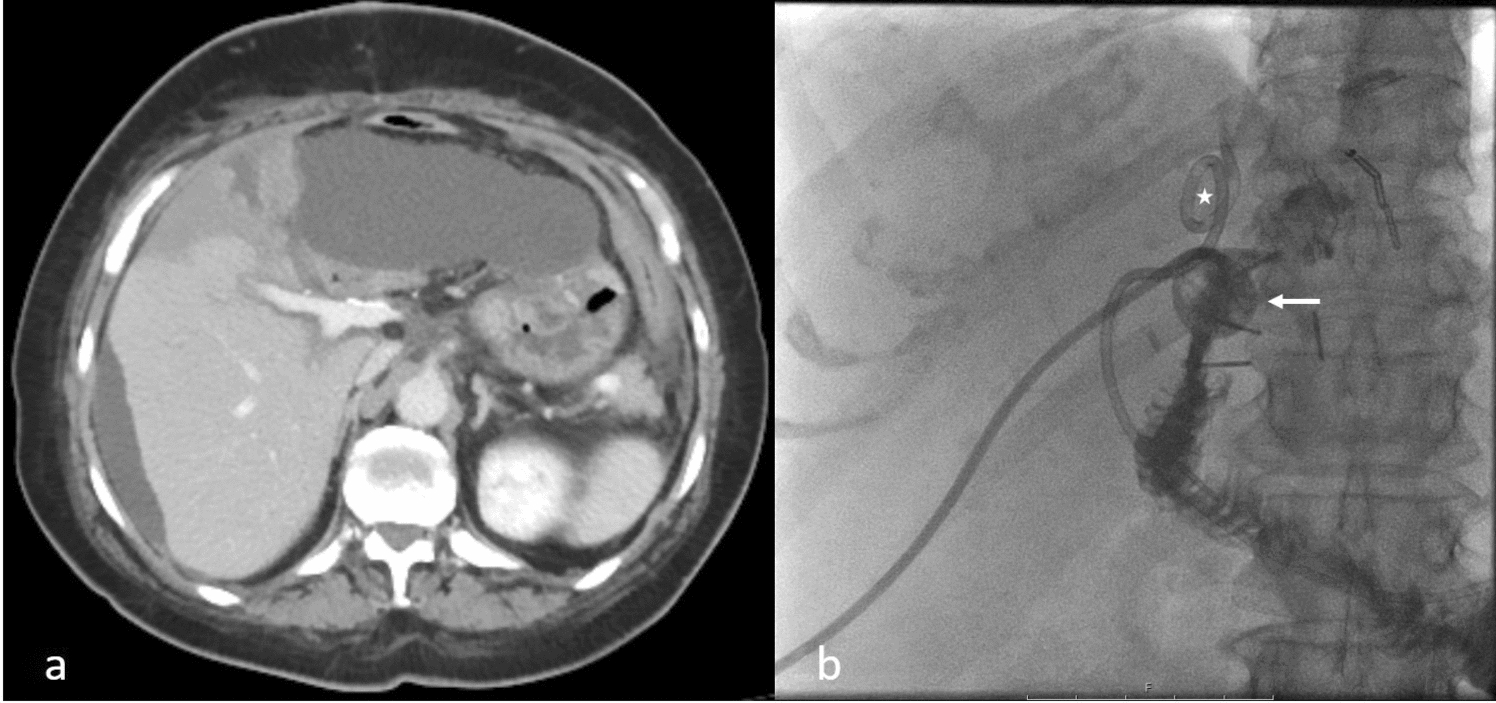
Fig. 2
A 64-year-old male (patient 2) who had undergone living-donor right hemi-liver transplant because of HCC and cirrhosis presented with persisting fever at 6 weeks. a A biloma was noted next to the liver resection margin and percutaneously drained (arrow). Retrograde opacification of the posterior right duct, but no communication with the endoscopically placed biliary stent-graft was found as the biloma drain was injected. That excluded duct was percutaneously accessed (arrowhead). b The indwelling stent-graft in the recipients common hepatic duct was utilized as a target at the puncture with a bent reversed 0.018″ guidewire (arrow). There is a rather large bile duct defect (arrowhead) filling the biloma. c Balloon dilatation (4 mm) of the neo-anastomosis. d The newly created bilio-bilio-neostomy was secured with an 8.5F PTBD (arrowheads). The biloma drain was left in place (arrow)
By means of a 22G Chiba needle the excluded posterior right hepatic duct was percutaneously transhepatically accessed. Vascular sheaths (8F, n = 3 or 10F, n = 1) were then introduced. A 5F catheter with an angled tip was then advanced as far as possible in the duct, followed by 2.7F coaxial microcatheter placement. Opacification of the bowel loop to be anastomosed was obtained in two cases by contrast injection via the PTBD. In the patient with the bilio-bilio-neo-anastomosis, the common hepatic duct (CHD) was easily visible under fluoroscopy due a previously placed stent-graft in the CHD. However, that stent-graft placed by endoscopy had failed to resolve the bile leak. In one patient the puncture of the bowel loop to be anastomosed was guided uniquely by fluoroscopy after review of the pre-procedural cross-sectional imaging depicting the anatomy of the adjacent small bowel.
In 3 out of 4 of cases, the stiff back end of a commonly available 0.018″ guidewire (V-18™, Boston Scientific Corp.) was used to access the enteric loop or the CHD. In order to direct this “sharp” recanalization, the tip of the reversed guidewire was bent accordingly. In one case, an Outback® Elite Re-entry catheter (Cordis, Miami Lakes FL, USA) was utilized. A microcatheter was advanced over the 018″ or, respectively, the 0.014″ guidewire through the presumed anastomosis. The correct enteric (n = 3) or CHD (n = 1) access was confirmed by means of contrast instillation. Dilatation of the track (2–4-mm-diameter angioplasty balloon) was then performed. Finally, the neo-anastomoses were secured by PTBDs (10.2F, n = 3; 12F, n = 1; Fig. 1).
The follow-up consisted of repeated cholangiographies via the PTBDs placed across the new anastomosis.
Comments (0)