
Remember me
This study encompassed 26 patients diagnosed with probable MSA-C, recruited from the Department of Neurology at Baotou Central Hospital in the Inner Mongolia Autonomous Region. Data were collected from January 2018 to May 2024. Participants were randomly assigned to either the study group (n = 13) or the control group (n = 13). The allocation of patients, clinicians, and experimenters was blinded. The Ethics Committee of Baotou Central Hospital approved and monitored this experimental study methodology. The present study was registered at the Chinese Clinical Trial Registry (https://www.chictr.org.cn/index.html, ChiCTR2400085610). The inclusion criteria were as follows: (1) the patient be classified as a probable MSA-C type according to The Movement Disorder Society Criteria for the Diagnosis of Multiple System Atrophy published in 2022[5]. (2) Age range of 50 to 75 years. (3) Absence of other neurodegenerative diseases. The exclusion criteria were as follows: (1) The presence of an unstable neurological or mental condition, either independently or in conjunction with a clinical illness. (2) Conducting a screening process to identify clinically significant abnormal test results, such as anomalies in electrocardiograms or laboratory tests. (3) A documented history of substance misuse, along with either a lack of legal capacity or limited legal competence. (4) Individuals with a history of cranial metal implants, bio-magnetic implants, metal-coated implants, neurosurgery, epilepsy, claustrophobia, or prior use of medications like bupropion or other substances that may increase the risk of TMS-induced seizures. (5) Positive pregnancy tests were observed. (6) Mini-Mental State Examination (MMSE) scores below 24 points. (7) Participation in another study concurrently with this trial. (8) Patients who had received any treatment for ataxia, anxiety, depression, or fatigue in the past six months. At the time of enrollment, some patients were taking oral medications that would not have influenced our findings. Prior to the commencement of the study, all patients provided their informed consent and data released consent. All patients were successfully completed the entire study without experiencing any adverse events during therapy.
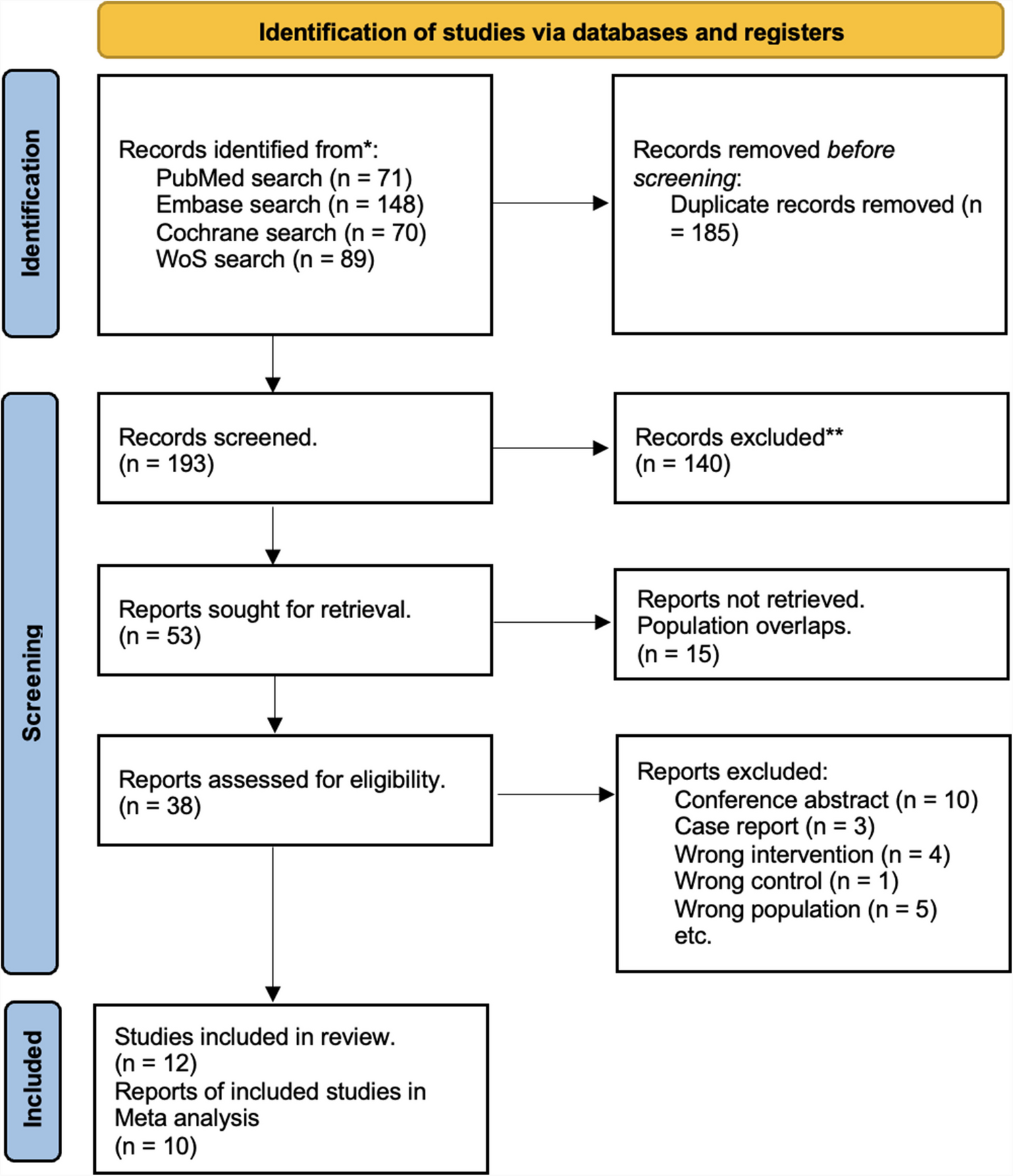
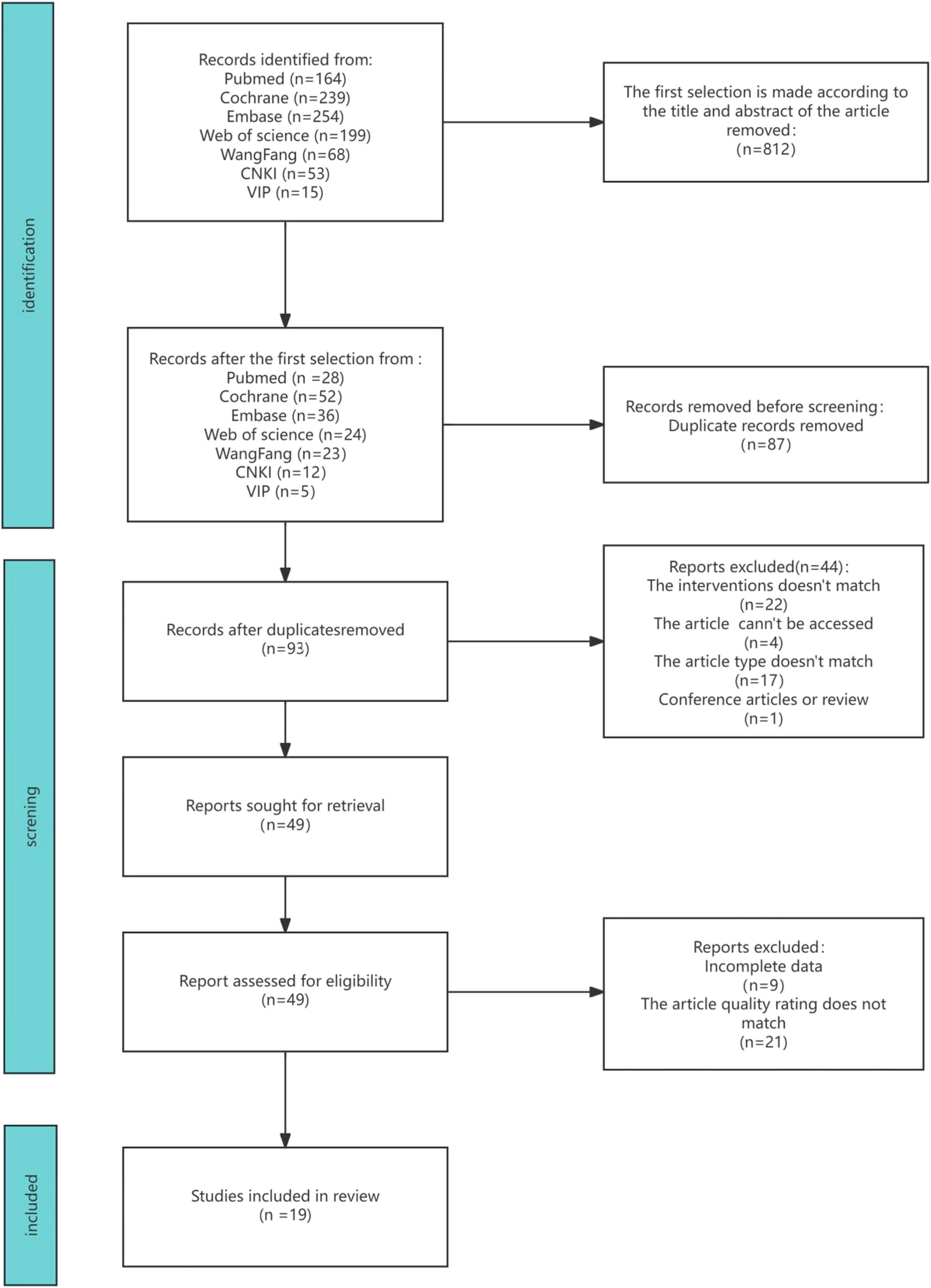
Experimental designThis is a single-center, randomized, double-blind experiment. A total of twenty-six patients diagnosed with MSA-C were assigned random numbers and then divided into two groups, namely the study group (n = 13) and the control group (n = 13), using a 1:1 ratio model (Fig. 1). The study group received iTBS for a duration of 10 days to activate both sides of the cerebellum, whereas the control group received sham stimulation. The treatment plan of patients was only known to rehabilitation therapist, while patients and other researchers remained blinded to both the treatment plan and the randomized sequence. Additionally, a blinded evaluation method was employed to assess the therapy's effectiveness.
Fig. 1
Schematic representation of experimental design
rTMS and Sham protocolsTMS was applied with a figure-of-eight coil (70 mm diameter) connected to a monophasic Magstim stimulator (Magstim Company Ltd., London, UK). The settings were configured to the resting motor threshold (RMT) multiplied by 80%. Intermittent Theta Burst Stimulation (iTBS), a specific form of TMS, consists of three pulses at a frequency of 50HZ, repeated every 200 ms. Each iTBS session includes a short burst lasting 2 s followed by an 8-s break, totaling 300 pulses per session. A total of 1800 pulses were provided, with three iTBS applied to both the left and right cerebellar locations, each spaced five minutes apart. Every patient received treatment at the same time each day. The stimulation coil was affixed to the robotic arm at a 45°angle inclination relative to the midsagittal surface, with the center of the coil oriented to activate both sides of the cerebellum. The control group received sham stimulation. Treatment was conducted over 10 days, spanning two consecutive weeks, with rest on Saturdays and Sundays, once daily.
Clinical assessmentsThe four scales were assessed at four time points: prior to the experiment (T0), the day following the experiment (T1), 2 weeks after T1 (T2), and 4 weeks after T1 (T3). In order to prevent potential bias, each patient underwent stimulation at various times throughout the day, ensuring unbiased data. The primary outcome measure was the scale for the assessment and rating of ataxia (SARA), which was used to assess the severity of ataxia and motor function. The secondary outcomes included the Fatigue Severity Scale-9 (FSS-9), the Hamilton Depression Scale-24 (HAMD-24), and the Hamilton Anxiety Scale (HAMA), which were utilized to assess the severity of fatigue, depression and anxiety.
Side effectsThe adverse effects commonly associated with the use of TMS devices can be categorized as follows: symptoms such as headache, pain, nausea, dizziness, and other unspecified symptoms. The trial should be terminated upon the occurrence of certain side effects.
Statistical analysisThe experimental data were analyzed by SPSS version 22.0 (IBM, Chicago, IL, USA). The demographic data were shown as the mean ± SD for continuous variables, and as the ratio for categorical variables. The outcome indicators were presented as the mean ± SD in the tables. For within-group comparisons of normally distributed scale scores, a paired t-test was employed. To compare scores between two different groups, a two-sample independent t-test was utilized. For non-normally distributed scale scores, the rank sum test was applied. A two-way repeated ANOVA analysis was conducted with rTMS/Sham group as the between-subjects factor and time (T0, T1, T2, T3) as the within-subjects factor to evaluate the effect of rTMS on clinical outcomes. A significance threshold of α = 0.05 was used to determine statistical significance. P-values < 0.05 was indicated a statistically significant difference.
Comments (0)