
Remember me


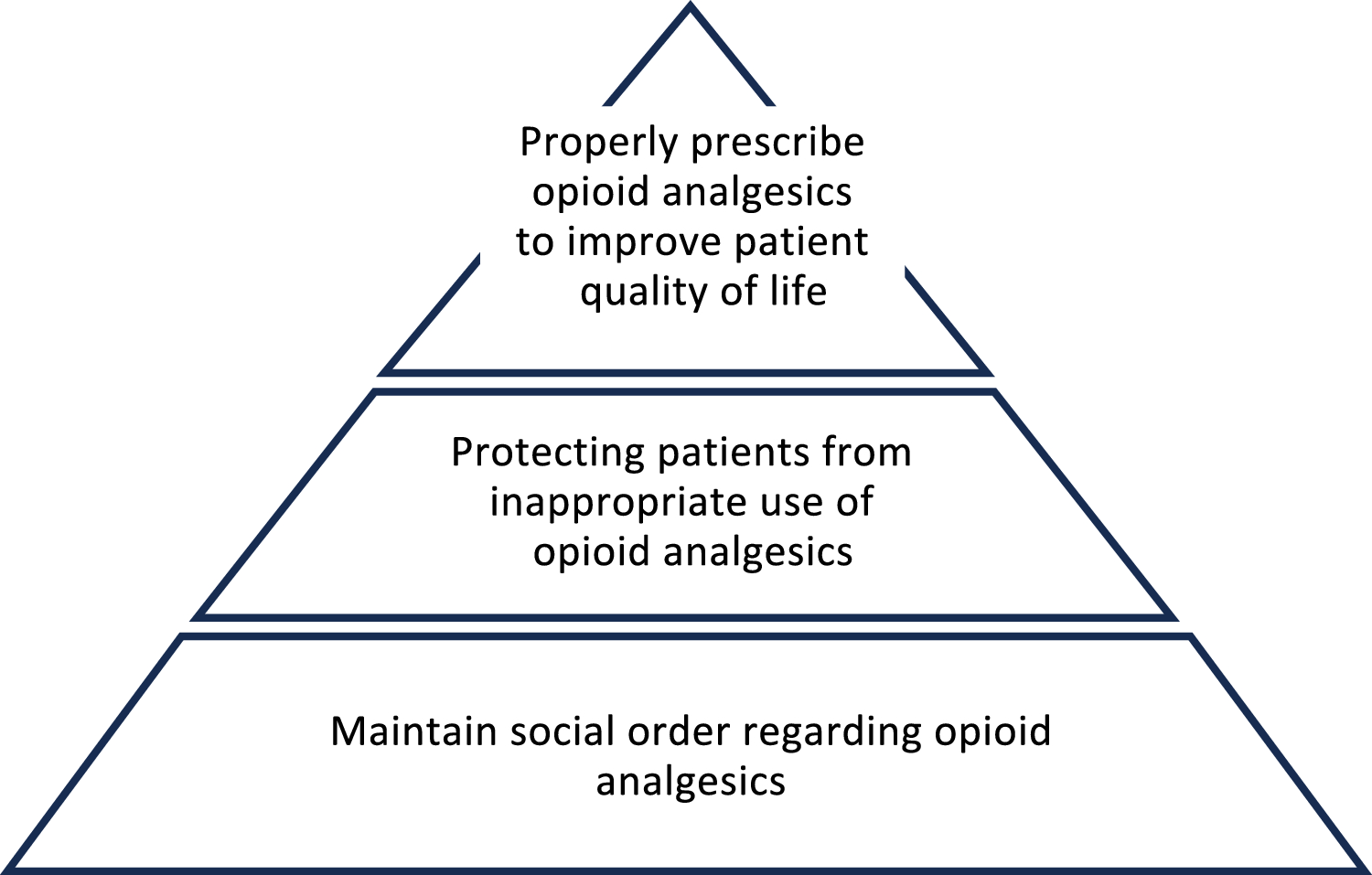
Opioid analgesics may be used only when non-opioid analgesics are ineffective and opioid analgesics are effective.
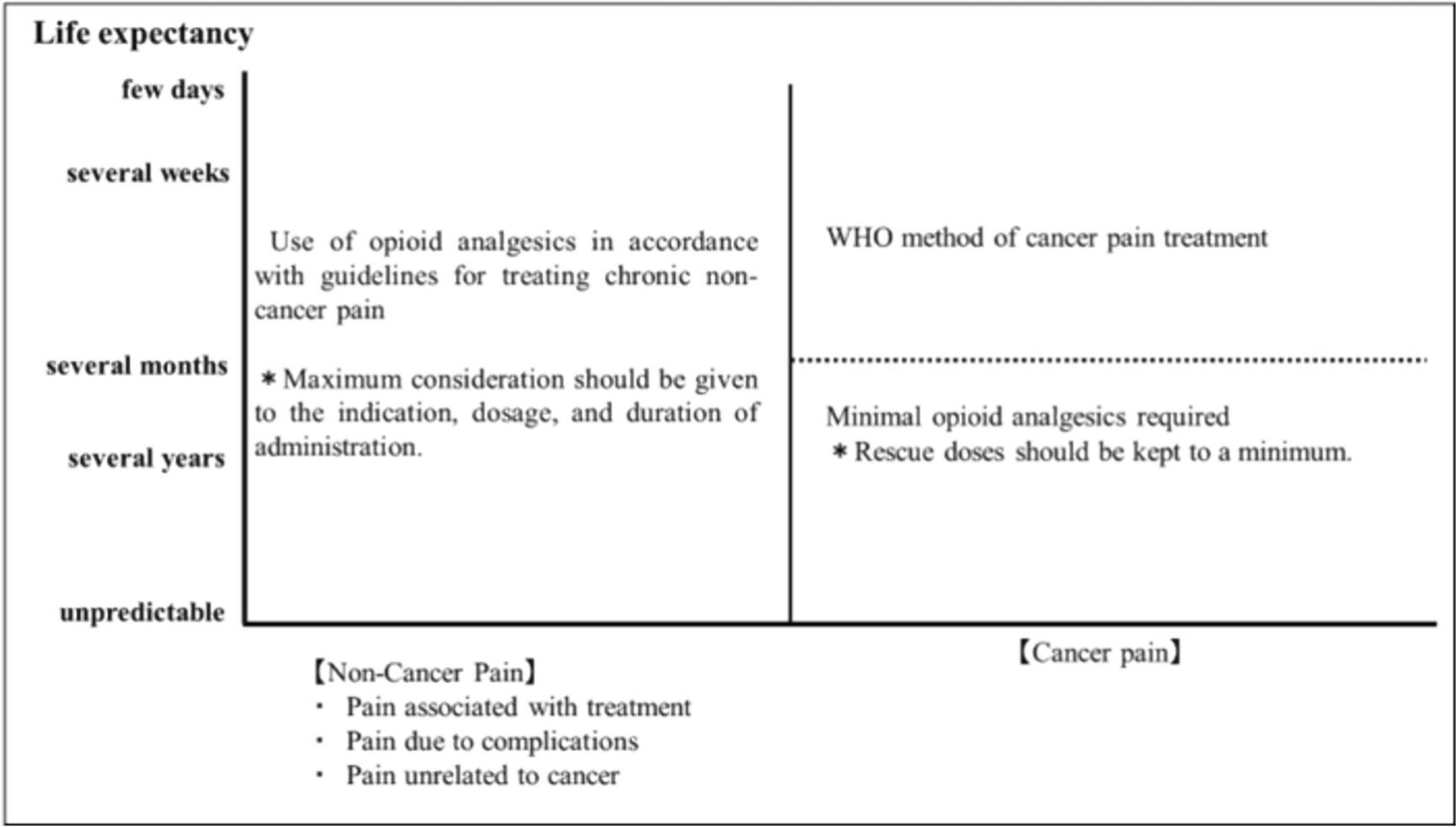
The method of use depends on the prognosis and whether or not the pain is caused by cancer.
If the prognosis is months or less and the pain is directly caused by cancer, cancer pain management according to WHO Analgesic Guidelines is indicated, and the use of rescue medication is also acceptable.
In cases of direct cancer pain with a prognosis of months to years, cancer pain management according to WHO Analgesic Guidelines is indicated, but the use of rescue medication should be kept to the minimum necessary.
For non-cancer pain, opioid analgesics should be prescribed according to the Guidelines for Prescribing Opioid Analgesics for Chronic Non-Cancer Pain only when non-pharmacologic therapies such as non-opioid analgesics and nerve blocks are ineffective, regardless of prognosis. A maximum dosage of oral morphine equivalent of 60 mg/day is recommended, and the dosage should not exceed 90 mg/day. The target duration of treatment should be 3 months and should not exceed 6 months, after which the drug should be withdrawn or the dose reduced and the patient reevaluated.
CommentaryWith advances in cancer treatment, cancer survivors are being treated for longer periods of time and their prognosis is improving. Cancer survivors are also experiencing pain for a longer period, and it is necessary to correctly assess each survivor’s situation and respond to pain according to each situation. It is also necessary to assess whether the pain is directly caused by cancer or is non-cancer pain (treatment-induced pain, cancer-related pain, or non-cancer-related pain). If the prognosis is months or less and the pain is directly caused by cancer, cancer pain management according to WHO Analgesic Guidelines is indicated, and the use of rescue opioid analgesia is also acceptable. In cases of direct cancer pain with a prognosis of months to years, cancer pain management according to WHO Analgesic Guidelines is indicated, but the use of rescue medication should be kept to the minimum necessary. For pain caused by factors other than cancer, regardless of prognosis, opioid analgesics should be prescribed in accordance with the “Guidelines for Prescribing Opioid Analgesics for Non-Cancer Chronic Pain” only when non-opioid analgesics are ineffective and non-pharmacologic therapies such as nerve blocks are ineffective [7]. Oral morphine equivalents are recommended up to 60 mg/day, with an upper limit of 90 mg/day. The target duration of treatment is 3 months, and should be reevaluated after a maximum of 6 months, with consideration given to drug withdrawal and dose reduction. Prescriptions should be made with attention to the patient’s history of alcoholism and drug dependence, as well as their psychiatric background.
Reported side effects of long-term use of opioid analgesics include constipation, confusion, upper gastrointestinal symptoms (heartburn, nausea, bloating), endocrine disturbances (fatigue, infertility, osteoporosis, decreased libido, menstrual irregularity) due to hypogonadism and increased prolactin secretion, neurotoxicity (myoclonus, worsening of psychological symptoms such as mood swings and memory impairment), risk of exacerbation of opioid-induced pain, and sleep-related disorders (exacerbation of apnea and sleep apnea syndrome due to concomitant use of benzodiazepines) [1]. Immunosuppression and tumor growth have also been reported, although evidence is lacking. For constipation and nausea, laxatives and antiemetics should be prescribed. In addition, to avoid long-term opioid use, it is important to continue pain assessment, aim for dose reduction/discontinuation, administer the lowest dose for the shortest period, and educate cancer survivors and their families [7, 8]. When reducing or discontinuing the dose, gradual reduction is necessary. When pain is under control, dose reductions should be made every 2–4 weeks [7], or by 10% to 25% followed by reevaluation, and temporary dose reductions of 50% to 75% should be made when dangerous side effects such as excessive sedation occur [9].
Clinical question: are opioid analgesics effective?Summary statementWhen prescribing opioid analgesics for cancer survivors, determine whether the pain is caused by cancer or non-cancer pain. When prescribing opioid analgesics for chronic pain other than cancer pain, follow the “Guidelines for the Prescribing of Opioid Analgesics for Chronic Non-Cancer Pain.”
The prevalence of adjustment disorders in cancer survivors is high, and substance abuse associated with long-term opioid analgesics is a concern, as it is in patients with chronic non-cancer pain.
The risk of substance abuse, gastrointestinal and cardiovascular events, falls and fractures, serious infections, and hospitalization in cancer survivors is high, and these risks increase with higher doses of opioid analgesics.
When treating chronic pain that requires long-term administration of opioid analgesics, prescription and patient care by a pain management specialist who can conduct rigorous patient screening and monitoring is recommended.
CommentaryOpioid analgesics such as morphine, fentanyl, and oxycodone can be prescribed for cancer pain in Japan, and also prescribed for chronic pain in cancer survivors. However, opioid analgesics that can be used for chronic non-cancer pain are limited to morphine tablets, morphine powder, fentanyl patch, and oxycodone (OxyContin® TR tablets). When prescribing long-term opioid analgesics for chronic pain in cancer survivors, it is necessary to consider whether prescriptions should be made in the same way as for chronic pain in non-cancer patients.
A cohort study of 34,188 early stage breast cancer patients in Denmark considered the relationship between opioid analgesics and breast cancer recurrence or development of second cancers [10]. The relationships between the type, duration, and dose of opioid analgesics and the breast cancer recurrence rate were unclear. Similarly, a United States cohort study of 4216 early stage breast cancer patients examined the relationship between long-term opioid analgesics (administered for > 75 days after cancer diagnosis) and breast cancer recurrence or development of a second cancer [11]. There were no significant differences in the rates of breast cancer recurrence or second cancer development between patients who were or were not receiving long-term opioid analgesics.
In Jones et al.’s integrative review of opioid analgesic use among cancer survivors [12], most references defined long-term opioid analgesic treatment as continued use for 3–6 months or longer after radical cancer treatment. In contrast, they defined chronic opioid analgesic treatment as continued use for 6–12 months or longer after the end of cancer treatment. Long-term opioid analgesics are used for 5% to 45% of cancer survivors and are more frequent in patients with head and neck cancer or breast cancer. Most long-term opioid analgesics were administered at dosages of oral morphine milligram equivalents (MME) of less than 20 MME/day. The proportion of patients receiving long-term opioid analgesics at 90 MME/day more than 3 years after completing cancer treatment was higher than in non-oncology patients. Prescriptions for opioid analgesics after completion of cancer treatment were often made by physicians who did not specialize in opioid analgesic treatment. In Canada, family physicians made more than 80% of long-term opioid analgesic prescriptions for patients beyond 5 years after cancer treatment. A history of opioid analgesic use and of chronic pain before cancer diagnosis were shown to be risks for long-term opioid analgesic use in cancer survivors.
Carmona-Bayonas et al., in their review of the literature on long-term opioid analgesic treatment of long-term cancer survivors [13], described the effects of opioid analgesic administration on the human body. Although there are many known effects of opioid analgesics on the immune system, such as decreased immune cell expression, the influences of long-term opioid analgesics on the immune system in long-term cancer survivors are unclear. The prevalence of adjustment disorders (including anxiety and mood disorders) among long-term cancer survivors is 27%–40%, raising concerns that psychological stress may lead to substance abuse during long-term opioid analgesic treatment. In patients with chronic pain, this treatment correlates with the incidence of self-harm, addiction, overdose, and hospital transport. Morphine, fentanyl, and oxycodone increase these risks, but data on long-term cancer survivors are scarce.
A United States cohort study of 38,310 cancer survivors aged 66–90 years who were cured after breast cancer treatment examined the risk of drug-related adverse events [14]. The study showed that opioid analgesics increased the risks of drug abuse, gastrointestinal events, falls, fractures, cardiovascular events, serious infections, and hospitalizations. Compared to patients who received non-opioid analgesics, the risk of drug-related adverse events in patients who received opioid analgesics was 2.3 times greater in the 1–49 MME/day group, and 3.4 times greater in the group receiving more than 50 mg MME/day, suggesting that higher doses of opioid analgesics raised the risk of drug-related adverse events. Although not shown definitively in that study, it can be inferred that most opioid analgesics administered at doses over 50 MME/day were morphine, fentanyl, oxycodone, etc.
As described in the aforementioned studies, long-term and high-dose opioid analgesics are prescribed for chronic pain in cancer survivors, depending on the type of cancer and the curative treatment. In addition, although some adverse events have been identified, the effects of long-term opioid analgesics in cancer survivors are still under study. When prescribing opioid analgesics for chronic pain in such patients, it is necessary to discuss rescue doses, the maximum dose, and the duration of administration from the perspective of adverse event prevention. At present, chronic pain caused by factors other than cancer pain should be treated in the same way as non-cancer chronic pain. Pain management specialists should take measures to prevent and treat opioid-related adverse events and also manage medication adherence.
Clinical question: are tramadol, buprenorphine, and codeine effective?Recommendations Summary statementTramadol is the most prescribed opioid for various types of pain in cancer survivors.
Tramadol is a second-line medicine for neuropathic pain when adjunctive analgesic drugs fail to provide adequate analgesia.
Tramadol can be prescribed without a narcotics license because it is classified as an unregulated drug in Japan. Since tramadol is an opioid, patients should be strictly followed, and careless administration and prolongation should be avoided.
The analgesic effects and side effect frequency of buprenorphine are the same as those of strong opioids such as morphine and oxycodone.
Insurance coverage for buprenorphine varies depending on the formulation.
CommentaryTramadol is used for various types of pain [15] and is the most frequently prescribed opioid for moderate to severe pain caused by cancer or non-cancer diseases [16, 17]. The metabolite O-desmethyltramadol (M1) has a weak affinity for the μ-opioid receptor and also inhibits the reuptake of serotonin and noradrenaline. Although it is expected to be effective for neuropathic pain, it has a “number needed to treat” of 4.4 and a “number needed to harm” of 4.2 [18], and the “Guidelines for the Pharmacologic Management of Neuropathic Pain” of the Japan Society of Pain Clinicians states that it is the second choice when antidepressants and gabapentinoids (pregabalin, gabapentin, and mirogabalin) do not provide sufficient pain relief [19]. Seizure due to tramadol is a side effect not seen with other opioid analgesics, and caution should be exercised because it can occur not only in the case of overdose but also at the recommended dosage [20]. Although it has been considered that tramadol is not associated with addiction liability even when used for chronic pain over a long period, recent reports have described the elevated, excited, and relaxed effects associated with dependence, as well as inappropriate use due to its lack of regulation as an opioid analgesic [21]. In addition, a cohort study not limited to cancer patients reported increased risks of all-cause mortality, cardiovascular events, and fractures, but there were no significant differences in the risks of constipation, delirium, falls, opioid dependence, or sleep disorders when compared with codeine [22]. In Japan, insurance covers tramadol alone as analgesia for chronic pain and for various types of cancer pain that are difficult to treat with non-opioid analgesics, while the combination of tramadol and acetaminophen is approved for chronic non-cancer pain that is difficult to treat with non-opioid analgesics and for pain after tooth extraction.
Buprenorphine is a partial μ-opioid receptor agonist that has a higher affinity for the μ-opioid receptor than other μ-opioid receptor agonists. Because of its strong analgesic effect, ceiling effect on respiratory depression, and low risk of respiratory depression at analgesic doses, it is the drug of choice for patients with sleep apnea, dependency tendencies, and respiratory disease, as well as those taking benzodiazepines, gabapentinoids, or muscle relaxants [23]. A comparison of extended-release morphine, oxycodone, fentanyl, and buprenorphine pastes showed no difference in analgesic efficacy over the 28-day observation period, as well as no difference in the incidence of adverse effects such as nausea, vomiting, constipation, and drowsiness [24]. Because of its analgesic effect, it is treated as a strong opioid in some countries. The effects of long-term administration on hormone secretion should be considered. Prolactin secretion is enhanced by low doses of buprenorphine (3 to 30 μg/kg) and suppressed by high doses (1,000 to 3,000 μg/kg). A study in opioid-dependent patients reported that patients treated with buprenorphine had preserved testosterone secretion and a lower incidence of hypogonadism than patients on methadone [25]. In Japan, injectable, suppository, and patch formulations are used clinically, but insurance coverage for injectable formulations is limited to postoperative indications, various types of cancer, and myocardial infarction; suppository coverage is limited to postoperative indications and various types of cancer; and patch coverage is limited to chronic back pain and osteoarthritis, which are difficult to treat with non-opioid analgesics.
Since codeine is metabolized to morphine by CYP2D6, its analgesic effect is diminished in patients with low levels of CYP2D6 metabolic activity. After the Centers for Disease Control and Prevention (CDC) issued guidelines for chronic pain [26], codeine prescriptions increased in the United States [27], but there are no studies with high-quality evidence on the use of codeine to treat chronic cancer pain. In Japan, insurance coverage is limited to analgesia regardless of the disease.
Are medications other than opioid analgesics effective in the treatment of chronic pain in cancer survivors?Clinical question: are non-opioid analgesics (NSAIDs, acetaminophen) effective?Recommendations Summary statementThe efficacy of NSAIDs and acetaminophen for neuropathic pain has not been demonstrated.
NSAIDs and acetaminophen should be used at the lowest effective dose for the shortest possible time, and their efficacy and adverse events should be assessed regularly to determine whether to continue or discontinue their use.
CommentaryNon-opioid analgesics are widely used worldwide for mild to moderate pain. NSAIDs have anti-inflammatory and analgesic effects. On the other hand, acetaminophen has analgesic and antipyretic effects but little anti-inflammatory activity in the periphery. These drugs are expected to be effective mainly for nociceptive pain [28]. Although NSAIDs and acetaminophen are frequently used for nociceptive pain in cancer survivors [29, 30], there is little high-quality evidence demonstrating their efficacy. A network meta-analysis of 81 RCTs (10,003 patients) on the treatment of chronic cancer pain found that other than opioid analgesics, codeine-aspirin combination therapy and diclofenac were effective treatments [31]. The 2016 ASCO publication “Management of Chronic Pain in Survivors of Adult Cancers: American Society of Clinical Oncology Clinical Practice Guideline” states that NSAIDs and acetaminophen may be prescribed for the relief of chronic pain and functional improvement if there are no serious drug interactions or contraindications [1]. However, while NSAIDs and acetaminophen may be effective for short-term pain control, their long-term administration and use at high doses should be avoided in light of their adverse effects (see below).
In addition, while neuropathic pain is often a component of chronic pain in cancer survivors, there is no high-quality evidence showing the efficacy of either NSAIDs or acetaminophen for neuropathic pain, and the Japanese “Guidelines for the Pharmacologic Management of Neuropathic Pain” do not recommend their use [19]. The Japanese “Clinical Guide of Management for Chemotherapy-Induced Peripheral Neuropathy” does not provide recommendations for their use due to lack of evidence [32].
Notable adverse effects of NSAIDs include gastrointestinal mucosal disorders, cardiovascular disease, renal disorders, hepatotoxicity, bleeding, and NSAID-exacerbated respiratory disease [33]. The risk of gastrointestinal disorders is higher with high-dose and long-term use of NSAIDs. The risk can be reduced using COX-2 inhibitors or by the concomitant use of proton pump inhibitors [34]. Regarding cardiovascular risk, previous NSAIDs are considered to have the same cardiovascular risk as COX-2 inhibitors, and NSAID use should be avoided in patients with cardiovascular disease [35]. In some countries, their use is contraindicated in patients in the setting of coronary artery bypass graft surgery. With regard to renal impairment, the Kidney Disease: Improving Global Outcomes (KDIGO) guidelines suggest that patients with an estimated glomerular filtration rate (eGFR) < 30 should avoid NSAIDs, and patients with an eGFR < 60 should avoid long-term NSAID use [36]. Other contraindications to the use of NSAIDs include a history of hypersensitivity to NSAIDs, serious blood disorders, serious hepatic disorders, serious cardiac dysfunction, serious hypertension, and late-stage pregnancy. In the treatment of chronic pain in cancer survivors, both the patient’s pain and general condition should be thoroughly evaluated, and if NSAIDs are indicated and effective, the lowest effective dose should be used for the shortest possible duration.
Although acetaminophen is considered better tolerated than NSAIDs, use of more than 2 g/day significantly increases the risk of upper gastrointestinal bleeding (relative risk 3.6 (95% confidence interval [CI], 2.6–5.1)) [37]. Furthermore, in recent years, the efficacy of long-term acetaminophen use for chronic pain in osteoarthritis has been questioned [38]. Therefore, discontinuation of acetaminophen should be considered if regular assessment indicates that it is not providing adequate analgesia. It should be used with caution in patients with hepatic dysfunction.
Clinical question: are adjuvant analgesics effective in the treatment of chronic pain in cancer survivors?RecommendationsGabapentinoids are used for neuropathic pain directly related to cancer in cancer survivors, and are weakly recommended in this context because they can reduce the necessary dose of opioid analgesics. [2B]
Duloxetine is weakly recommended for chronic pain in cancer survivors because it is more effective for pain due to chemotherapy-induced peripheral neuropathy (CIPN) than other adjuvant analgesics. [2B]
Corticosteroids should not be used long term in cancer survivors for the sole purpose of relieving chronic pain. [2D]
Summary statementAdjuvant analgesics such as gabapentinoids and antidepressants, which are first-line agents for neuropathic pain, can also be used for cancer-related neuropathic pain, allowing for a reduction in the dose of opioid analgesics. Gabapentinoids such as pregabalin have been validated for efficacy.
Pregabalin has been reported to be effective for prolonged pain in postmastectomy pain syndrome and post-thoracotomy pain syndrome, but there are no reports of long-term efficacy.
CommentaryAlthough opioid analgesics are often used for cancer-related neuropathic pain in patients with cancer, gabapentinoids and antidepressants are also used. The use of these adjuvant analgesics is recommended to reduce the dose of opioid analgesics, especially in long-term survivors [39]. The efficacy of pregabalin has been validated [40]. Antidepressants such as amitriptyline and duloxetine may also be effective, but there are few reports on the effects of antidepressants for cancer-related neuropathic pain, and there is no firm evidence [41]. These adjuvant analgesics should be modulated to ensure central nervous system tolerability.
In cancer survivors, quality of life may decrease due to persistent pain caused by cancer treatment, such as prolonged postoperative pain and peripheral neuropathy due to chemotherapy. A study demonstrated the efficacy of pregabalin in patients complaining of postmastectomy chronic pain (PMCP) [42]. There have been several prospective studies on postoperative pain after thoracotomy, many of which have shown the efficacy of pregabalin. However, there are no studies on the long-term effects of pregabalin, and more research is warranted [43]. The use of adjuvant analgesics may allow for the discontinuation or dose reduction of opioid analgesics when the latter are used to treat chronic postoperative pain. However, gabapentinoids should be used with caution in patients with renal dysfunction, and if long-term use is ineffective, discontinuation, dose reduction, or non-pharmacologic treatment such as interventional therapy should be considered. CIPN lasts from several months to several years after chemotherapy, causing sensory disturbance and neuropathic pain that reduce the quality of life of patients with cancer, and 30%–50% of patients develop chronic CIPN. One study showed that duloxetine was effective for CIPN-related pain as well as numbness in the lower extremities [44]. It is also the only drug recommended for CIPN by ASCO [45]. In Japan, the Japanese Association of Supportive Care in Cancer (JASCC) published the “Clinical Guide of Management for Chemotherapy-Induced Peripheral Neuropathy” in 2017 [32]. According to this guide, we are moderately confident in the effect estimate for duloxetine, and the strength of the recommendation is weak. On the other hand, the effectiveness of pregabalin is unclear.
Duloxetine is contraindicated in severe hepatic or renal impairment, and duloxetine administration may increase the risk of suicidal ideation or suicide attempts in patients under 24 years of age. It is sometimes used in combination with opioid analgesics for cancer pain, but it may cause adverse events such as drowsiness and dizziness. Concomitant use with monoamine oxidase inhibitors is contraindicated, and serotonin syndrome may occur with serotonergic agents.
Corticosteroids are recommended by the “WHO Guidelines for the pharmacological and radiotherapeutic management of cancer pain in adults and adolescents,” revised in 2018, to be administered for pain control as an adjunctive agent when indicated [46]. Previous reports provide moderate-quality evidence that corticosteroids may alleviate pain and improve quality of life, and that they may allow for dose reductions of opioid analgesics. Corticosteroids are used for a variety of pain conditions, including pain from bone metastases, but should be prescribed for as short a period as possible. Long-term use in cancer survivors for the sole purpose of relieving chronic pain is not recommended, as there are contraindications in some cases.
Clinical question: are Kampo medicine and bisphosphonates effective in the treatment of chronic pain in cancer survivors?Summary statementThe efficacy of Kampo medicine for CIPN has been widely reported, but no clinical evidence has been established to support its standard use.
The efficacy of Hangeshashinto for oral mucositis (OM) caused by cancer treatment has been reported in many cases.
The use of bisphosphonates is recommended for osteoporotic pain in cancer survivors receiving hormone therapy, but caution should be exercised regarding the development of osteonecrosis of the jaw with long-term use.
CommentaryChinese herbal medicine (Kampo medicine) is often effective in relieving pain that is not adequately treated by Western analgesics alone, and the choice of Kampo medicine for cancer pain in cancer survivors may reduce the use of opioid analgesics and improve quality of life.
In cancer survivors, CIPN often continues for a long time, resulting in decreased quality of life. There have been many basic and clinical studies on the treatment of CIPN with Kampo medicine [47]. CIPN is becoming an important issue in terms of maintaining quality of life due to the increasingly long-term survival of cancer survivors. There have been several reports on the efficacy of Goshajinkigan for CIPN [48, 49]. The efficacy of Ninjin’yoeito on CIPN has also been reported [50]. Although there have been several studies on Kampo medicine, clinical evidence supporting the standard use of Kampo medicine for CIPN has not yet been established, and future studies on the mechanisms of neuropathy as well as the efficacy of Kampo medicine are expected. The JASCC guidelines also do not recommend the administration of Goshajinkigan as prophylaxis for CIPN [32]. However, the use of Kampo medicine may reduce the dosage of other drugs. Side effects of Kampo medicine include liver dysfunction and interstitial pneumonia for Goshajinkigan, and pseudoaldosteronism and myopathy for Ninjin’yoeito, and these medicines should be discontinued if they are not effective.
OM occurs in 20% to 40% of patients receiving cancer chemotherapy. The incidence of OM increases from 60 to 85% when blood stem cell transplantation is added, and to 90% when patients receive chemotherapy combined with radiation for head and neck cancer. The effect of Hangeshashinto on OM has been shown to be due to the promotion of oral keratinocyte migration through upregulation of chemokine ligand 12 (CXCL12) via extracellular signal-regulated kinase (ERK) [51]. Studies in patients with colorectal cancer and gastric cancer reported that the mean time to improvement of grade 2 or higher OM was shorter in the group treated with Hangeshashinto than in the placebo group [52, 53]. OM caused by radiation or anticancer drugs is difficult to treat and may require the use of opioid analgesics, but their dosage may be decreased by the concomitant use of Hangeshashinto. Mouth rinses or topical application of Hangeshashinto is associated with fewer side effects than systemic administration.
Patients undergoing hormone therapy, such as patients with breast or prostate cancer, have reduced bone density and are at increased risk of osteoporosis [54]. When bisphosphonates and denosumab are used to treat osteoporosis pain in cancer survivors, they should be used at the indicated dose for osteoporosis [54]. The potential development of osteonecrosis of the jaw should be noted with long-term use of these agents.
Are non-pharmacologic therapies effective in the treatment of chronic pain in cancer survivors?Clinical question: is interventional therapy effective?RecommendationsNerve blocks with neurolytics for cancer-related pain in internal organs are effective and may be considered because they can reduce the use of opioid analgesics. [2C]
Intrathecal analgesia is an effective means of treating intractable cancer pain and may be considered. [2C]
Summary statementNerve blocks with neurolytics for visceral cancer-related pain are effective and can reduce the use of opioid analgesics. Early intervention is likely to be effective.
Intrathecal analgesia is an effective means of treating intractable cancer pain.
Spinal cord stimulation (SCS) may be considered for intractable cancer pain and pain associated with cancer treatment (e.g., peripheral neuropathic pain caused by anticancer drugs), although the quality of the evidence is low.
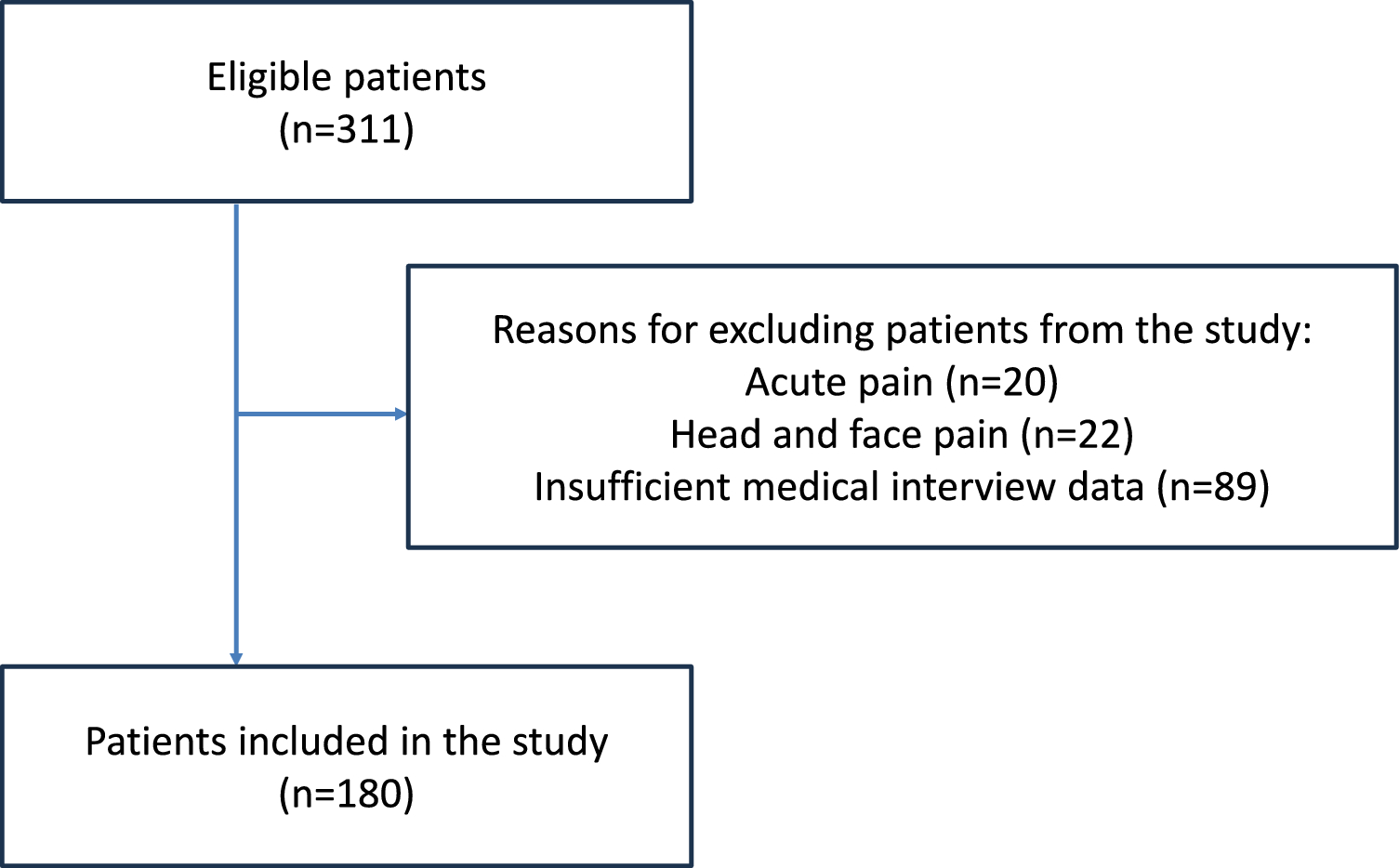
CommentaryAlthough it is difficult to conduct a high-quality RCT of interventional treatment for pain in cancer survivors since the number of target patients is small and their prognosis is variable, there is a relatively large number of reports on nerve blocks with neurolytics for cancer-related pain in internal organs. A comparison of two groups of patients, treated with or without a relatively early celiac plexus block (splanchnic nerve block), showed that the group with the block had better pain relief and quality of life [55]. In a report of superior hypogastric plexus block in 180 patients with pain due to pelvic malignancy, pain was reduced by 48% and the use of opioid analgesics was reduced by 55% within the 3 months after the procedure [56]. In an RCT of 50 patients divided into a superior hypogastric plexus block group and an opioid analgesics-only group, pain and the opioid analgesics dosage were reduced by more than 50% in the block group over a 2- to 3-month period [
Comments (0)