The 700-µg preservative-free sustained-release DEX implant is utilised as an intravitreal treatment to maintain therapeutic levels within the vitreous for an extended period [14]. At present, the DEX implant has emerged as a valuable option for managing posterior segment diseases. However, it carries certain pharmacological risks, including steroid-induced cataracts and glaucoma, as well as non-pharmacological complications such as anterior chamber migration, vitreous haemorrhage, and retinal detachment [15]. Essentially, the pharmacological risk is significantly lower compared to other intravitreal steroid injections [16]. Evidence indicates that intravitreal triamcinolone can increase IOP by approximately 35%, whereas the DEX implant increases IOP by about 15% in cases of retinal vein occlusion [17, 18]. Additionally, the relative risk of cataract progression with the DEX implant is about 3.5 times lower than with intravitreal triamcinolone [16].
However, this favourable pharmacological safety profile may be compromised by non-pharmacological adverse events that can occur when a cylindrical implant, measuring 6.0 mm in length and 0.46 mm in diameter, is injected through the pars plana using a 22-gauge needle. The mechanical trauma at the injection site, along with the proximity of the sharp needle to the retina, could potentially cause vitreous haemorrhage, retinal detachment, or the introduction of microorganisms into the eye. Moreover, in cases with previous history of vitrectomy, defective iris tissue, zonulo-capsular diaphragm instability, or anterior hyaloid face rupture, the DEX implant may migrate into the anterior chamber, potentially leading to irreversible corneal decompensation [14, 19, 20]. While ongoing efforts aim to enhance the safety of DEX implantation into the vitreous, concurrent evaluations are exploring new strategies to reduce the side effect profile while maintaining the efficacy of the DEX implant [21, 22].
Approval of suprachoroidal injection of TA by FDA has represented a breakthrough in this field. Previous studies have demonstrated that the concentration of TA in the posterior segment is 12 times higher with suprachoroidal injection compared to intravitreal injection. With only 3% of the drug entering to the anterior chamber [10, 11], steroid exposure within the anterior segment is minimised and the risk of IOP elevation and cataract formation is reduced with suprachoroidal injections [23].
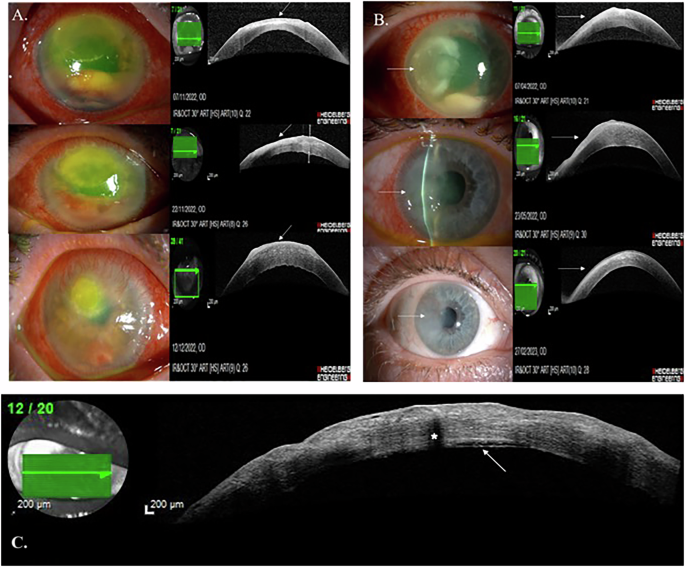
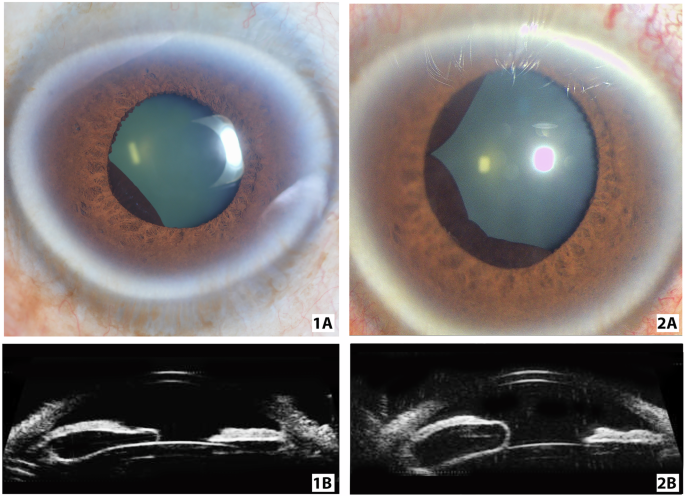
The results in our study showed that anterior segment OCT can be used as a tool to monitor the placement of the SC implant. Here in our cases, SC-DEX treatment was well tolerated and anatomical and visual efficacy and safety parameters were comparable to that of IV-DEX treatment. BCVA levels were significantly better in the SC-DEX group compared to the IV-DEX group during the first week of injections (p = 0.014). When considering both groups, although baseline BCVA was not statistically significant, the lower BCVA in the IV-DEX group may have contributed to the limited improvement after the IV-DEX injection, which differed from the literature [24]. No differences were observed between the two groups at any visit in terms of IOP fluctuations. However, due to the short follow-up period of the study, cataract progression could not be assessed in either group.
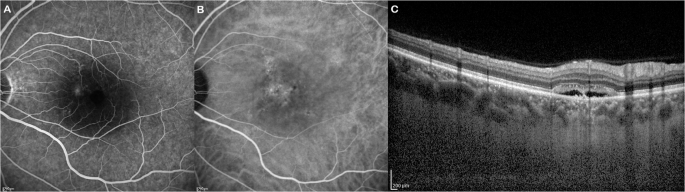
Our findings showed that the reduction of MRT was more pronounced in the 1st and 3rd months of follow-up compared to the 1st week. However, the duration of efficacy was relatively shorter in the SC-DEX group than the IV-DEX group. Although not statistically significant, the incidence of retreatments was slightly higher in the SC-DEX group. These differences may be attributed to pharmacokinetics within the SC space. Initially, the implant may exhibit a slow-release profile in the SC space, while the increased clearance of aqueous-soluble substances over time could contribute to early depletion [25,26,27,28]. The reduced effectiveness of the DEX implant in vitrectomized eyes may serve as a reference for demonstrating this mechanism [29]. In terms of MRT, a statistically significant difference was observed in the SC-DEX group in the postoperative period across different visits, except for the first week (Fig. 1C, D). Regarding CRT values, there was no statistically significant difference between the two groups at any visit, nor was there a statistically significant difference in CRT changes between groups (Table 2). However, the lack of significance in MRT change at the first week and the near-significant difference in CRT values during the first week may suggest a slower onset of the SC-DEX implant’s effect. Hydrophilic drugs are cleared via choroidal circulation, which may explain the weaker initial effect due to the early clearance of dexamethasone from the DEX implant. However, the relatively small sample size may also account for this finding. Since suprachoroidal DEX implant administration is novel in the literature, further studies are required to evaluate this observation.
Despite these promising early results, SC-DEX therapy may still raise concerns about its safety profile. Fortunately, no vision threatening complications occurred in either treatment groups. Along with further studies on safety, adhering to proper patient selection and injection technique could help prevent undesirable consequences [25, 29]. Previous studies on suprachoroidal application of corticosteroids have demonstrated optimistic outcomes. In a phase 3 study of suprachoroidal TA for noninfectious uveitis, the rate of increased IOP was 11.5%, which is lower than the 25–43% incidence reported with intravitreal DEX implants for uveitic macular oedema [8]. In an animal study by Chen et al., the authors suggested that the increase of IOP in suprachoroidal TA could be volume-dependent [12].
It is known that IV-DEX implantation can lead to cataract formation, with the risk increasing with repeated injections [14]. Reports indicate that 12.4% of eyes treated with IV-DEX implants required cataract surgery during follow-up [30]. Additionally, rapidly progressing cataracts have been reported after IV-DEX injections, potentially due to trauma from the injection procedure or contact with the intravitreal implant [31]. SC-DEX injection offers the advantage of preventing some non-pharmacological complications such as capsular damage to the lens and the risk of implant migration into the anterior chamber.
The results obtained in this study are important as they demonstrate that the SC space is amenable to injections beyond those previously established. To our knowledge this is the first study to investigate the efficacy and safety of SC-DEX injections. One of the strengths of the study is its comparative evaluation of outcomes for both intravitreal and SC injections. However, this study has several limitations. These include its preliminary nature, the relatively small sample size, off-label use of the implant, and the lack of multicentre collaboration. Additionally, the effect on macular oedema due to different indications, its impact on vitrectomized eyes, and its effects on naïve eyes should also be investigated, similar to intravitreal DEX implants [32, 33].
Given that various biopolymers are biocompatible, effective, and capable of extending the half-life of drugs in the suprachoroidal space, there is considerable potential for emerging therapies utilising various drugs administered via the suprachoroidal space [25]. Currently, the dexamethasone implant stands out as a leading candidate for this application.
In this context, detailed safety assessments conducted using the SC- DEX application can enable a thorough review and refinement of existing standard treatment approaches. This process may particularly support the development of personalised treatment strategies for cases with intravitreal related risks and facilitate modifications to treatment protocols. Specialised designs and materials may be necessary to facilitate injection into this area and ensure compatibility with the surrounding tissue.
In conclusion, this preliminary study suggests that SC injection of the DEX implant is a promising alternative for managing posterior segment diseases. It demonstrates effectiveness comparable to intravitreal administration, with the potential for similar or reduced complications. Comparative, multicentre studies with large sample sizes and the use of multimodal imaging are needed to confirm the efficacy and safety of SC-DEX injections and beyond.

Comments (0)