
Remember me
This prospective, mixed-methods, case series study was conducted at an Australian specialist cancer hospital between April 2022 and June 2023 following approval from the institutions’ Human Research Ethics Committee [15]. The published protocol (in which the NEAT is referred to by its original working title—The Checklist) provides a detailed description of methods and procedures [16].
Theoretical frameworkThis study was informed by Smart’s multidimensional model of clinical utility, where four dimensions (appropriateness, accessibility, acceptability, and practicability) impact the practical usefulness of an intervention to improve health outcomes [14]. “Appropriateness” explores the effectiveness and relevance of an intervention to clinical decision-making and disruptions to current work and care. Acceptability explores whether the intervention is acceptable to service users, providers, and broader society. “Practicability” examines suitability, whether the intervention performs in real-world settings; functionality, whether the intervention, training, and instructions are complete and in working order; as well as current and future training and knowledge requirements. “Accessibility” was not examined as it pertains to economic considerations of an intervention, which was out of the scope of this study.
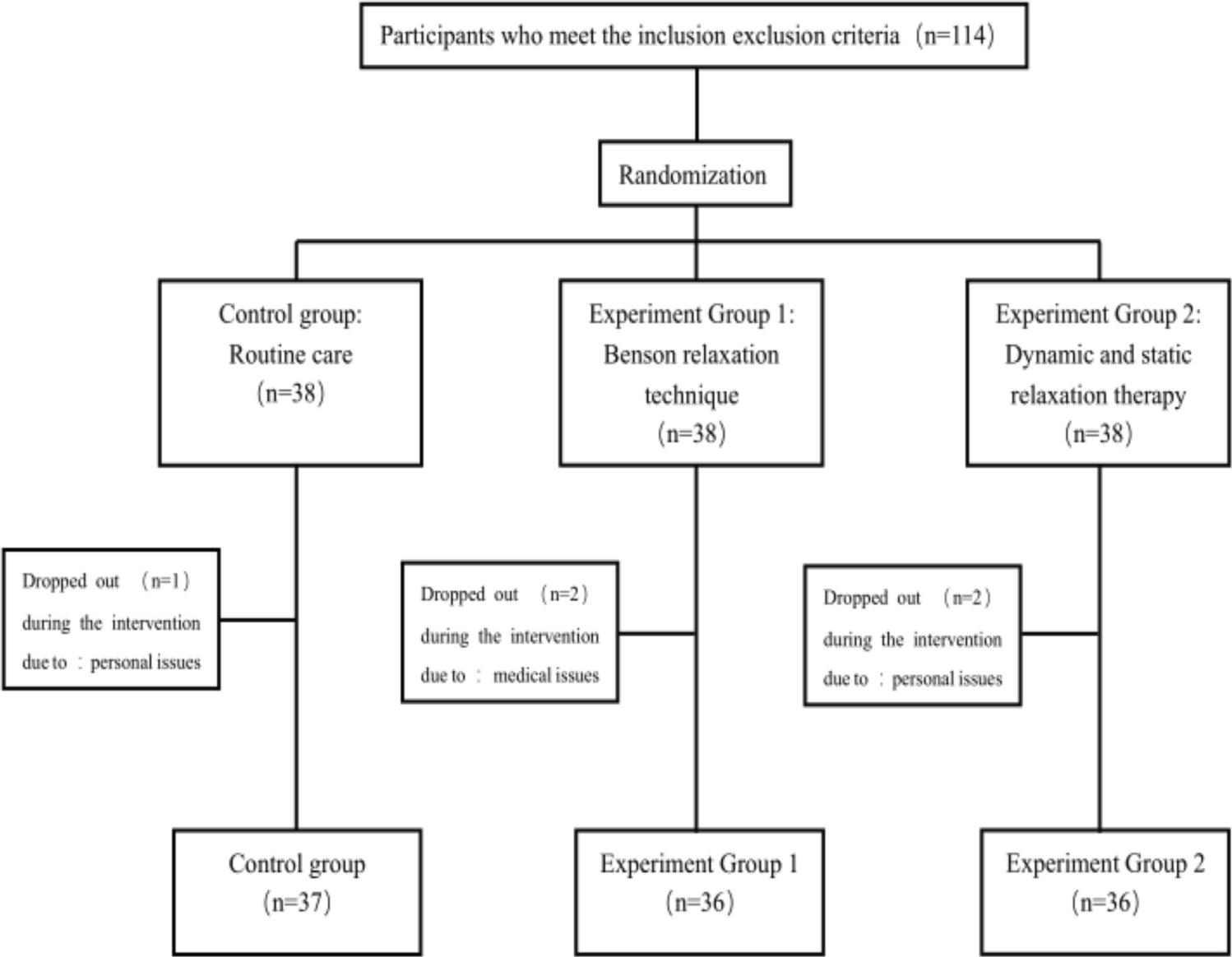
ParticipantsThe study sample comprised patients newly diagnosed with genitourinary, gynaecological, head and neck, or lung cancer (hereafter “patients”) and clinical nurse consultants (hereafter “CNCs”) delivering care. Eligibility criteria are provided in Fig. 2.
Fig. 2
Data collection procedures and corresponding study objectives
RecruitmentCNCs practising in each tumour group were invited to participate. Then, participating CNCs identified potentially eligible patients from out-patient clinic lists. Project officers, not involved in the care of patients, used the hospital’s electronic medical record (EMR) to confirm eligibility before approaching patients by phone and sending interested individuals a participant information form (PIF) to review via email or post, depending on participant preference. All participants provided signed informed consent prior to any data collection activities, and consent was re-affirmed and recorded at the beginning of interviews (Tables 1 and 2).
Table 1 Participant characteristicsTable 2 Qualitative quotes demonstrating patient and CNC perceptions of NEAT clinical utility (at time of interviews the NEAT was referred to by its original name, the “Complexity Checklist” or “Checklist”)Intervention: the NEATFocus areas targeted by the NEAT were identified via a review of published literature and focus groups with 100 Australian cancer nurses, in three repeated phases, until a stable draft of the tool was confirmed (preliminary content validity) [16]. Then, face and content validity was assessed by case study testing. Thirty nurses tested the NEAT using three hypothetical case studies across three phases to inform revisions until no further modification was necessary. Next, five CNCs tested the NEAT, with ten newly diagnosed cancer patients each to confirm face and content validity, and provide preliminary utility data [16].
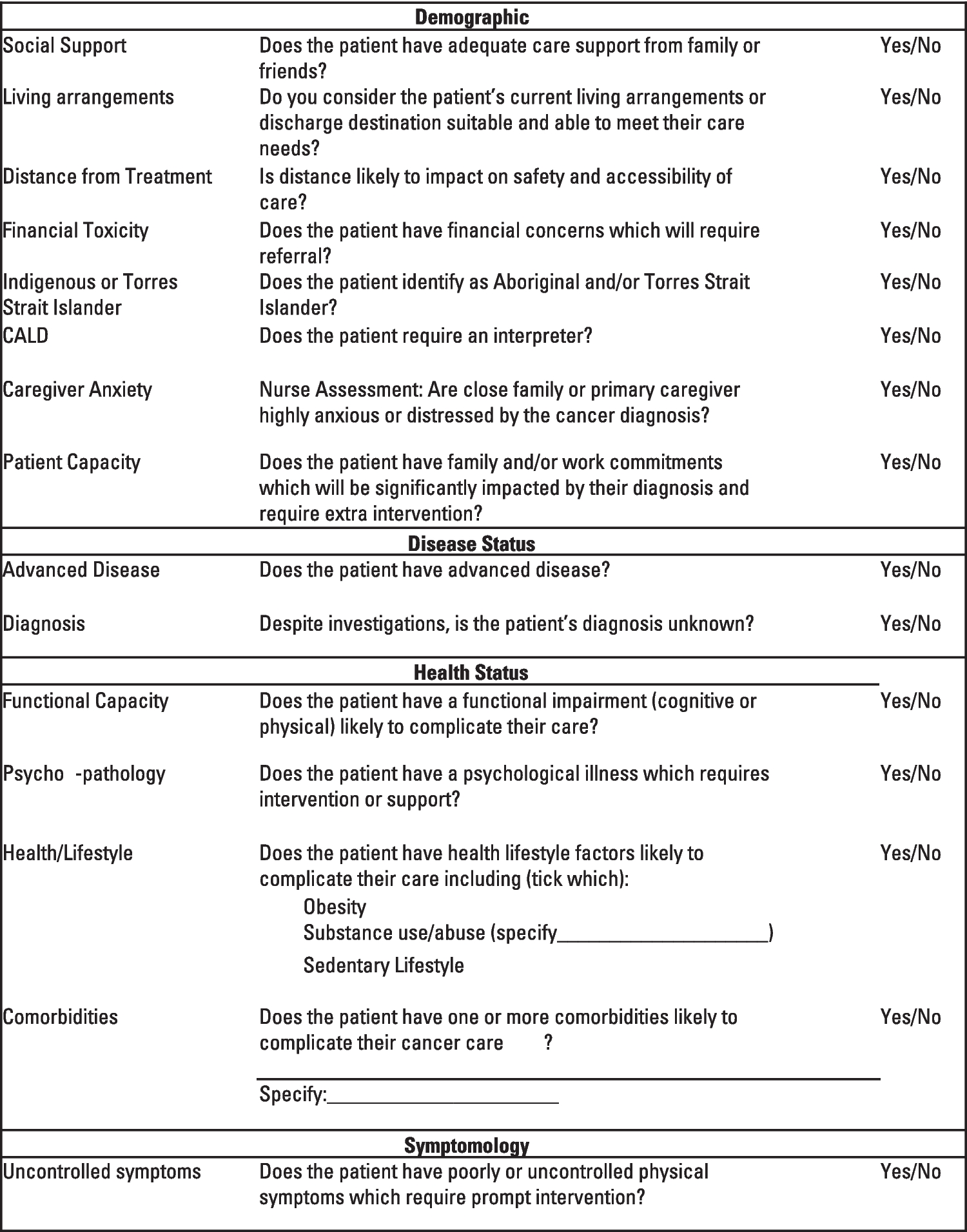
The intervention comprised CNC training and delivery of the NEAT, which consists of 15 items mapping to four domains (demographic characteristics, disease status, health status, and symptomatology) [16]. Each item in the NEAT is answered in a yes/no response format, where nurses elicit relevant information during consultation conversations to inform their clinical judgements. Importantly, there is no predetermined cut-off or threshold for caseness. Here, caseness is classified where a symptom or need is assessed as warranting a referral. The purpose of the NEAT is to ensure that each patient has opportunity to have their needs systematically and comprehensively explored early in their cancer journey, and support nurses’ clinical decision-making through structured comprehensive assessment. Assessment information was used by nurses delivering care to help inform tailored (or person-centred) information provision and referrals (see Table 3).
Table 3 Health service use by caseness (case = complex (n = 10) and non-case = not complex/unsure (n = 27)). Caseness based on classifications made at T0Before using the NEAT, CNCs took part in a 30-min training session either individually or in pairs, depending on availability. Training was delivered by the study project officer and registered nurse with expertise in cancer (EC) and detailed guidance on NEAT content and use, including standards for responding to items (e.g., what constitutes adequate exercise) [17, 18]. CNCs used the NEAT to guide discussions that identified SDoH factors, and thus risk of complex care needs, as part of a consultation with participating patients. Once complete, the NEATs were uploaded to the EMR and made available to the patient’s treating team.
Data collection proceduresA total of four data collection points were completed over a total of 24 weeks.
Patient participant enrolment was finalised on completion of the NEAT (T0) with a CNC. After its completion, CNCs filled out a brief survey on NEAT administration details comprising: time taken to complete the NEAT, mode of delivery, whether the patient had assistance to complete the NEAT, and caseness. For caseness, CNCs used NEAT data to provide a subjective determination to the question: “Would you consider/expect this patient to have complex care needs” assigning for each patient the following: case, non-case, unsure.
Within 2-weeks post-enrolment (T1), patients completed a semi-structured interview to explore their views on the clinical utility of the NEAT. Before interview commencement, patients completed five patient-reported outcome measures (PROMs) related to the following specific NEAT items:
Social support: PROMIS short-forms Instrumental Support [19]
Patient capacity: ability to participate in social roles and activities [20]
Functional capacity: physical function [21]
Uncontrolled symptoms: self-efficacy for managing symptoms [22, 23]
Financial toxicity: COST-FACIT [24]
Twelve weeks after enrolment (T2), patients reported uptake of services and unplanned service use (internal/external) since T1, via phone interview or online survey (based on patient preference). Interviews also explored aspects of the appropriateness, acceptability, and functionality of the NEAT. Patients were also asked to report referrals offered, accepted, and declined in the context of hospital care as well as externally.
Unplanned service use included any unplanned contact with their cancer care team, unplanned hospital admissions, and emergency department presentations. Twenty-four weeks after enrolment (T3), details on treatment, referrals offered by CNCs and accepted/declined by patients, and unplanned service use were extracted from the EMR. These data were used to confirm T2 data and record service usage between T2 and T3.
At T2 and T3, CNCs took part in semi-structured interviews to explore perceptions of the clinical utility of the NEAT and its application, including predictive capacity. The first interview focused specifically on appropriateness, acceptability, suitability, and training and knowledge requirements to deliver the NEAT, perceptions of its impact in routine care, and barriers and enablers to implementation. The second interview explored the impact of the NEAT on routine care and patient care trajectories during the study. CNCs also provided a re-appraisal of caseness (case/non-case) at T3 based on their knowledge of each patient’s pathway from T0 to T3.
Data analysis proceduresQualitative dataInterviews were transcribed verbatim and managed in NVivo12 [25]. The three groups of interviews were analysed separately using deductive and inductive content analysis [26]. Initial coding frames were informed by Smart’s multidimensional model of clinical utility and iteratively revised as data analysis progressed, concurrent to data collection [14, 26]. This process comprised adding and collapsing codes and categories to classify data. Two trained qualitative researchers (HC, EC) independently co-coded at least 10% of each interview group, and resolved discrepancies through consensus agreement. Data were synthesised to explore similarities and differences among participant perspectives regarding the clinical utility of the NEAT. Disagreement regarding interpretation of data and coding alignment was addressed through study team discussions.
Quantitative dataQuantitative data were analysed in Excel 365 and RStudio [27, 28]. PROMs were scored and recoded based on author guidelines [19,20,21,22,23,24, 29]. PROMIS t scores were recoded and scored to discrete variables comprising two categories: within normal limits and outside normal limits [29]. T0 caseness was recoded to a discrete variable: case (complex) and non-case (not complex/unsure). Descriptive statistics were used to summarise participant characteristics, CNC survey responses, and PROMs data. Caseness at each time point was determined as a proportion with 95% confidence interval using the Wilson method. Differences between participants and decliners were explored using chi-square, Fisher, and independent t tests as appropriate.
Differences in health service usage (number of admissions, referrals, and contacts e.g., phone calls) data between T0 caseness groups (case, non-case/unsure) were evaluated using Wilcoxon signed-rank tests. Contingency tables were used to explore the relationship between NEAT items and PROMIS scores. Cohen’s kappa was calculated to provide a measure of agreement. Concordance between the NEAT’s financial toxicity item and COST-FACIT scores was examined descriptively, and Cohen’s U3 calculated to provide a measure of non-overlap [30].
Comments (0)