
Remember me

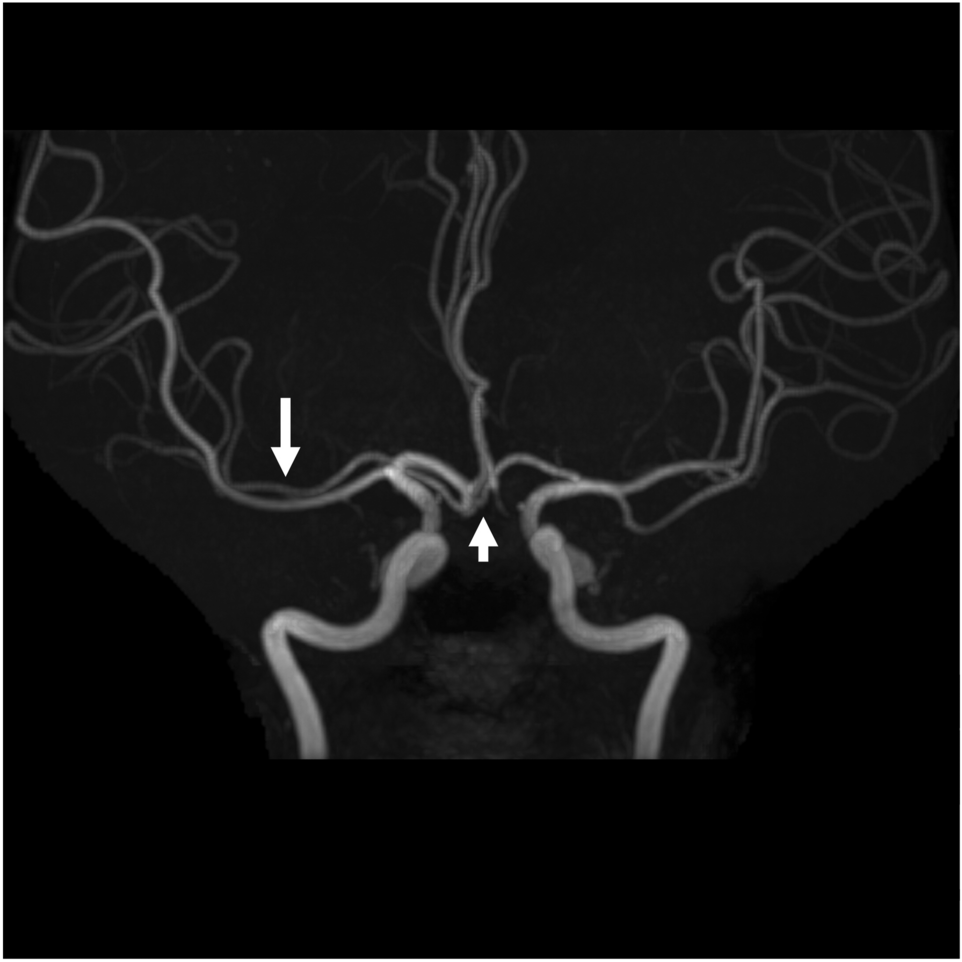
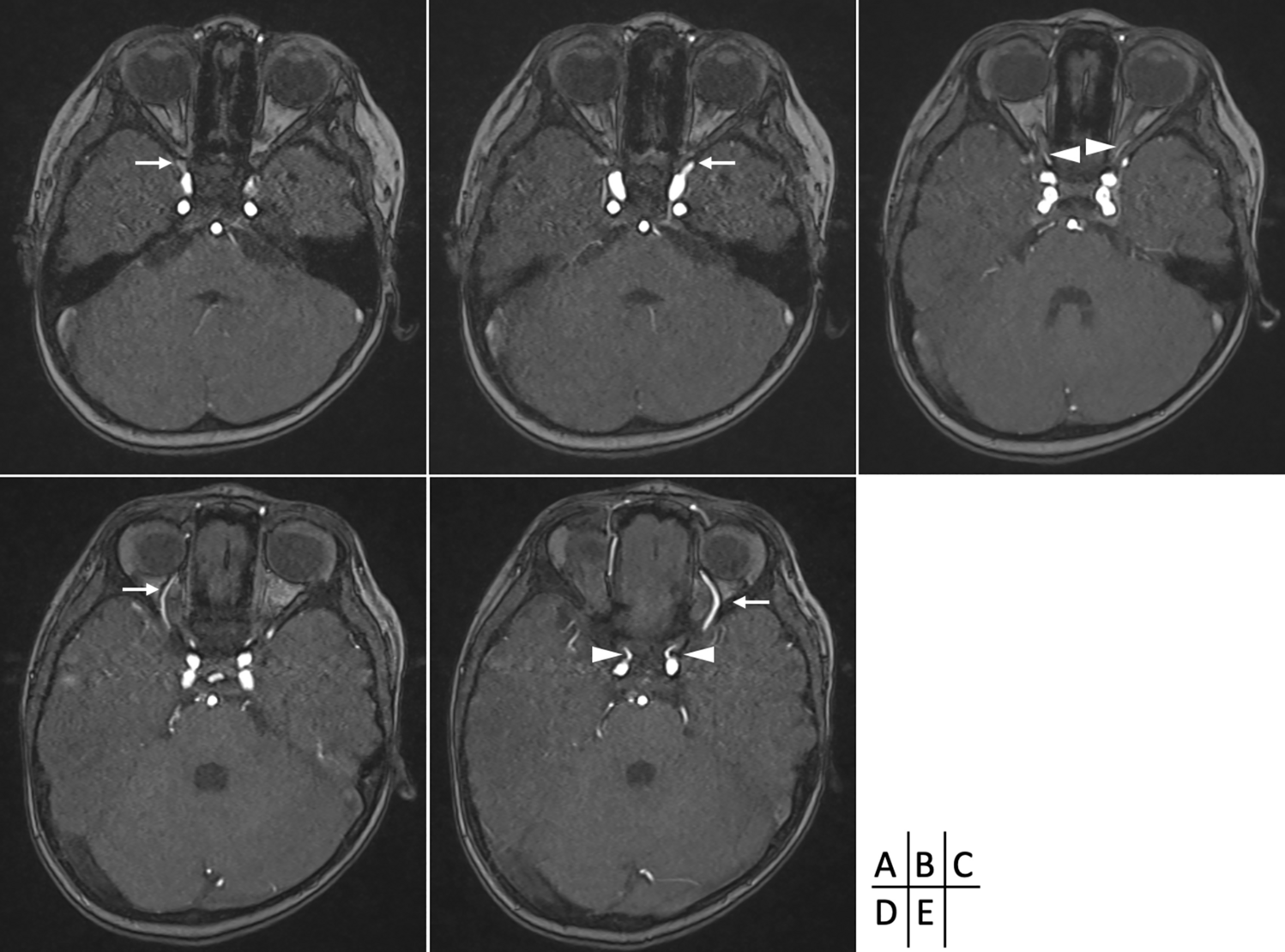
Case 1. A 79 years old female patient, that presented to neurologist for a persistent vestibular syndrome. At MRI exam was discovered a trigeminal artery that originates from the superior surface of proximal right internal carotid artery C4 segment, situated in the cavernous sinus lateral wall. From it’s origin, trigeminal artery is directed superior and lateral, situated inferior to oculomotor and trochlear nerves, medial to trigeminal nerve ophthalmic branch (Fig. 4).
Fig. 4
Anterior to petrous part of temporal bone, the artery is bending in an 90° angle, comes in close relation with trigeminal ganglia, then becomes horizontal, directs posterior and medial, it travers Meckel cavum, pierce dura mater inferior to petroclinoid ligament, medial to trigeminal nerve sensory root and goes in prepontine cistern, medial to trigeminal nerve, superior from abducens nerve, and tangent to pons right half. Trigeminal artery is anastomosing with basilar artery inferior from superior cerebellar artery origin superior to anteroinferior cerebellar arteries origin. The trigeminal artery has a 5.1 mm caliber an a length of 32 mm (Fig. 5).
Fig. 5
VR reconstruction with length measurements
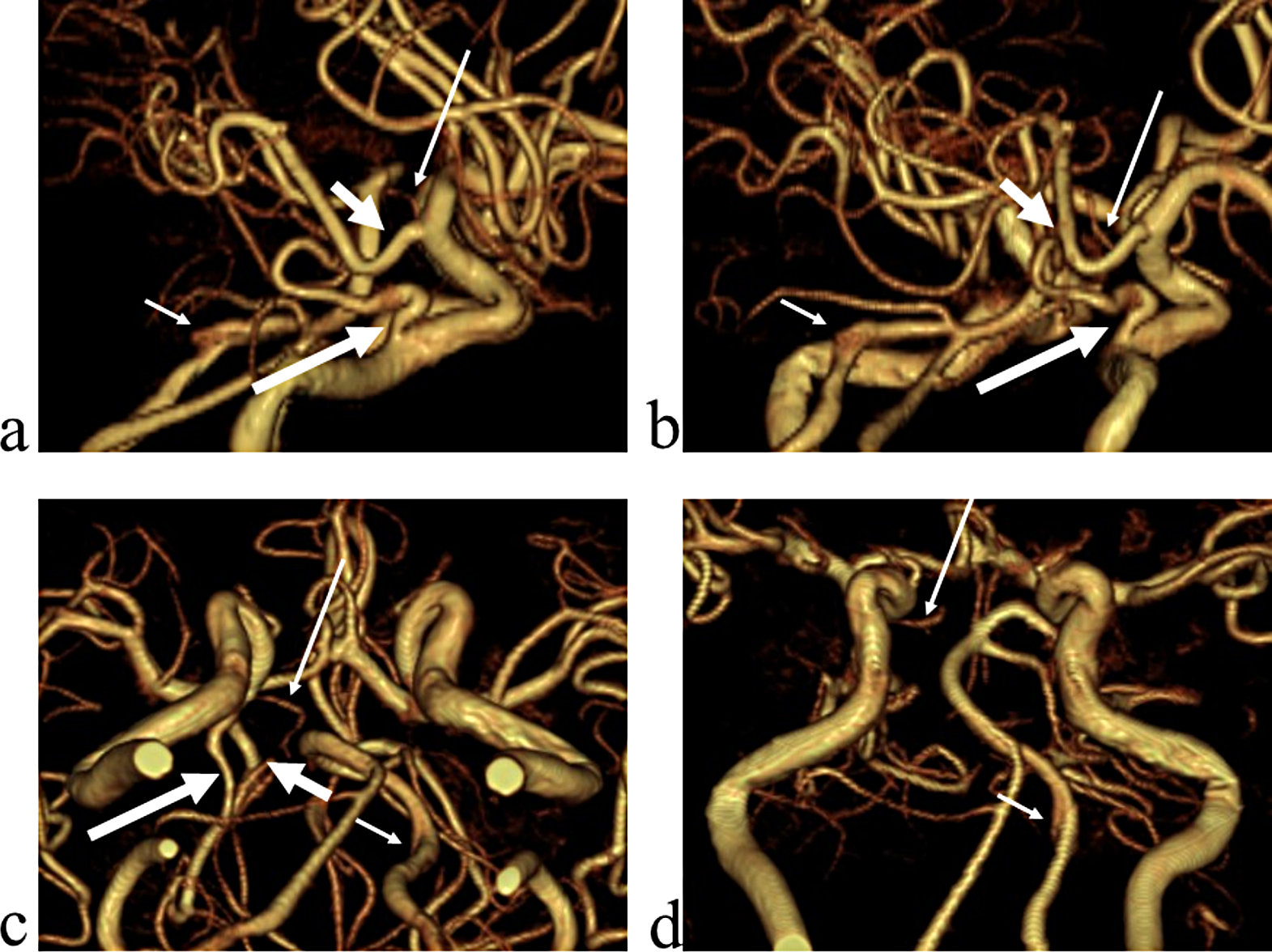
Trigeminal artery is associated with other anatomical vascular anomalies: basilar artery hypoplasia below anastomosis with trigeminal artery, where it has a caliber of 1.3 mm, superior to anastomosis with a caliber of 4.3 mm. Same side communicating artery cannot be seeing, agenesis, with normal developed posterior cerebral arteries that have a 2.7 caliber on left side, 3.2 mm on right side, so it can be included in Saltzman type I (Fig. 6). Also associates contralateral vertebral artery hypoplasia (Fig. 7, Fig. 8).
Fig. 6
VR reconstruction, of Saltzman type 1 trigeminal artery and contralateral vertebral artery hypoplasia
Fig. 7
TOF sequence demonstrating basilar artery hypoplasia
Fig. 8
TOF sequence with normal caliber basilar artery above trigeminală artery anastomosis
Case 2: A 32 years old female patient that presented to neurologist for left hemicranias. On MRI exam we discovered a trigeminal artery with its origin on left internal carotid artery superior surface in proximal C4 segment. The artery has a short ascending and lateral direction in the cavernous sinus lateral wall, with a length of 6 mm it angles at 70o, change its trajectory inferiorly and medially towards Meckel cavum, in this segment is positioned inferior and lateral to oculomotor nerve, medial to trigeminal nerve ophthalmic branch, that it also slightly deviates. The trigeminal artery perforates dura inferior to petroclinoid ligament it becomes horizontal forming an 110o angle and goes medial in prepontine cistern, comes in contact with trigeminal nerve laterally. The artery it’s anastomosing with basilar artery inferior from superior cerebellar artery origin. Trigeminal artery has a total length of 26 mm with a 3.9 mm diameter. From trigeminal artery rises left anteroinferior cerebellar artery at 9 mm distance from the anastomosis with basilar artery (Fig. 9, Fig. 10).
Fig. 9
VR reconstruction demonstrating trigeminal artery
Fig. 10
.Angle mesurent in TOF séquence
Trigeminal artery presence it’s associated with other vascular anomalies like: basilar artery hypoplasia, with a 1.8 mm caliber inferior to trigeminal artery anastomosis, 3.4 mm diameter superior from it, posterior cerebral artery hypoplasia that is not anastomosing with ipsilateral posterior communicating artery, it gives only the deep branches and posteromedial choroid artery. Left posterior communicating artery has a 2.1 mm diameter and is distributing in posterior cerebral artery cerebral vascular territory (Fig. 11). Right cerebral artery is normal developed with a 2.4 mm diameter. Trigeminal artery is also associated with right vertebral artery hypoplasia (Fig. 12). In relation with Saltzman classification, on the base of vascular territories, this trigeminal artery is an intermediary type with ipsilateral posterior cerebral artery hypoplasia, specific to type II and normal developed right posterior cerebral artery associated with basilar artery hypoplasia specific to type I.
Fig. 11
TOF sequence, the developed left posterior communicating artery
Fig. 12
MIP of a TPF sequence demonstrating basilar artery hypoplasia inferior to trigeminal artery
Case 3: 16 years old female patient presents to neurologist for hemicranias and diplopia, with right eye abduction deficiency. On MRI exam we discovered right rectus lateralis muscle edema and a trigeminal artery from right internal carotid artery. The origin of this artery is on C4 segment superolateral surface, it has a sinous aspect, it form al loop with lateral convexity at 18o, descends in cavernous sinus, medial to trigeminal nerve ophthalmic branch, comes in direct contact with abducens nerve at it entrance into cavernous sinus (Fig. 13), is positioned inferior to oculomotor nerve, angulates at 700 turn posteriorly and medially, it traverse Meckel cavum medial and inferior to trigeminal ganglia, pierces dura and change direction at 90o, becoming horizontal in prepontine cistern where it’s anastomosing with basilar artery inferior to superior cerebellar artery origin (Fig. 14). The trigeminal artery, in this case, has a 2.7 mm diameter and 32 mm length.
Fig.13
Coronal MIP of a TOF sequence with right trigeminal artery
Fig. 14
Axial MIP of TOF sequence of trigeminal artery anastomosing inferior to superior cerebellar artery
This case, besides trigeminal artery, has other vascular anomalies: bilateral posterior cerebral artery P1 segment hypoplasia that has 1 mm diameter on the right 1,2 mm diameter on left, the flow in cerebral vascular territory beying assured by posterior communicating arteries, that has 1.6 mm diameter on the right, 1.8 mm on the left, so it can be included in Saltzman type II. The basilar artery is hypoplasic inferior to trigeminal artery anastomosis with a 1.4 mm diameter, and superior to this with a 2.8 caliber, similarly with trigeminal artery. Also has right vertebral artery hypoplasia and a median pericallosal artery, with origin from anterior communicating artery (Fig. 15).
Fig. 15
VR reconstruction of a TOF sequence, with a type II Saltzman trigeminal artery
Discussions.
In this study we found an 0.35% incidence for trigeminal artery, value that is similarly with [12, 15]. Although the study was made on few cases, only 3 trigeminal arteries, we observed a clear dominance for lateral type, described by Salas [16], situated lateral to sella turcica, with origin on internal carotid artery C4 segment superior or superolateral surface. The arteries traverse cavernous sinus where are in relation with oculomor, trochlear, abducens nerves and trigeminal nerve ophthalmic branch. They are exiting cavernous sinus, inferior to petroclinoid ligament entering in prepontine cistern where are joining basilar artery inferior to superior cerebellar arteries origin. Also we noticed woman dominance for this anatomical variant. Regarding the position to middle line we observed a right dominance with 2:1 ratio.
On the base of vascular territories, regarding [17] classification, we found equal proportion for type I and type II and one case was an intermediary between those two. If type I assures blood flow to cerebellum, brain stem and posterior inferior and medial part of cerebral hemispheres and type II assures blood flow only for cerebellum and brain stem, the second case described in this study, trigeminal artery assures blood flow for cerebellum, brain stem and only one brain hemisphere, variant that was not included in [17] classification.
In all cases there was a degree of basilar artery hypoplasia and hypoplasia or agenesis of vertebral arteries, most commonly the contralateral, in a ratio of 2:1. Those vascular anomalies lead to decreased blood flow to posterior cerebral fossa that is being supplied by internal carotid artery thru trigeminal artery. There has being described brain stem strokes in case of internal carotid artery or trigeminal artery occlusion in studies made by Kwon [10], Okada [11], Kato [9].
In other cases there have being reported symptoms like vertigo, nausea, vomiting, parenthesis, all specific for circulatory insufficiency in the vertebrobasilar system [18], similarly to the one reported in the first case. In their studies, Battista [4] and Eluvathingal [8] are supporting the theory of transient ischemic attacks, as cause of vertigo [1].
In all cases trigeminal artery was situated medial to trigeminal nerve and trigeminal nerve ophthalmic branch, running parallel with it. From a clinical point of view, trigeminal neuralgia is one of the most encountered pathologies associated with trigeminal artery [4]. In second case, trigeminal artery effectuates a lateral convex curvature, creating a vasculo nervous conflict with trigeminal nerve ophthalmic branch corresponding to same side hemicranias described by the patient.
In third case, trigeminal artery has a descending route out of the cavernous sinus and comes in contact with abducens nerve near Dorello channel, with evidence of external rectus muscle suffering. Other studies also described different degrees of ophthalmoplegia associated with trigeminal artery, depending on the trajectory and relation that this artery have and cranial nerves that are coming in contact with [6, 8].
In our study we haven’t found arterial aneurysm or arteriovenous malformations.
Comments (0)