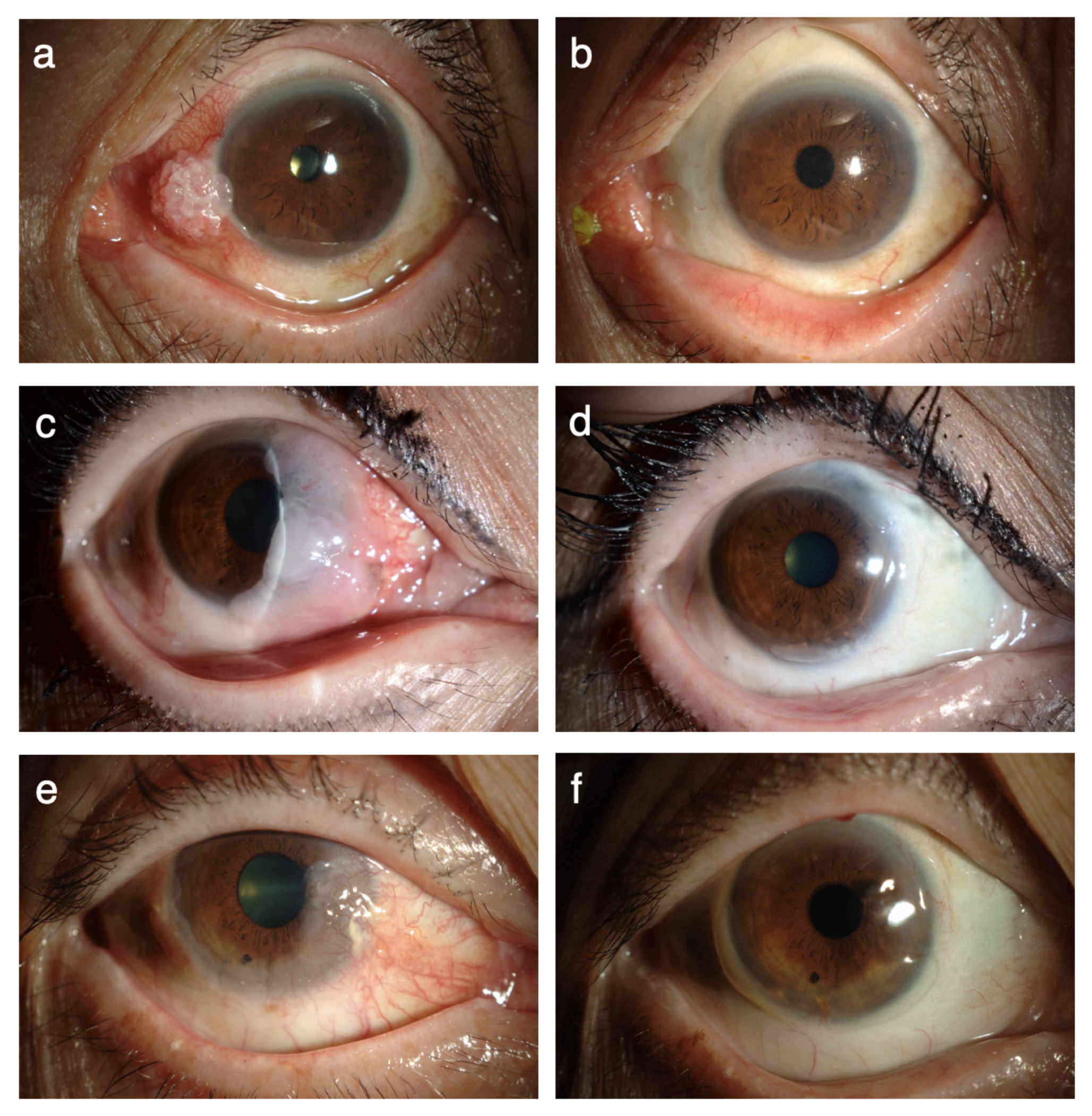
We clarified that IJCN is characterized by the presence of pigmented masses with trophic vessels and cystic lesions that are located near the corneal limbus of the bulbar conjunctiva. No significant differences were reported between the sexes in terms of the incidence of the nevus; however, IJCN was observed more commonly in boys with some kind of allergic reactions. Some of these characteristics are consistent with those reported in previous studies [2,3,4,5, 7,8,9, 13]. The serum immunoglobin E levels of boys tend to be higher than those of girls until puberty and boys tend to be more sensitive to allergies than girls [14]. This might explain the sex differences observed in the incidence of IJCN.
The triggering factors that cause marked inflammation in IJCN are not exactly known. Compared with noninflammatory nevi, IJCNs exhibit an increase in the number of eosinophils, lymphocytes, and mast cells. Fibroblasts in these lesions promote eosinophil adhesion via NGF (nerve growth factor) and induce allergic inflammation. This process is reported to be an immune response induced by the nevus itself [15]. Furthermore, Kato and colleagues reported that conjunctival melanocytes are involved in conjunctival pigmentation with a stem cell factor that is produced by fibroblasts under conditions of allergic inflammation [11]. Thus, the conjunctival pigmentation observed since early childhood in our cases might have been accelerated by recurrent inflammation of the lesions.
Conjunctival nevi rarely (< 1%) show malignant transformation [5]; however, nevus cells that are atypical or found in large nevi of > 10 mm, with acute progression, are difficult to distinguish from malignant tumors [16, 17]. Findings such as cyst formation and vascular invasion are suggestive of IJCN [2, 5, 7], and AS-OCT has been used to visualize cyst formation within the tumor and detect the border above the underlying sclera [18]. The differential diagnosis of IJCN remains challenging because vascular invasion is usually observed in both IJCN and malignant tumors [5]. We have shown that AS-OCTA can visualize low blood flow within the pathogenic lesion and the invading vessels are mainly confined to the sclera underlying the lesion. Although we consider that this observation achieved using AS-OCTA is not specific to IJCN, this is the first study to demonstrate this finding of IJCN using AS-OCTA.
That AS-OCTA can be used to differentiate IJCN from malignant tumors without any invasion, especially in children, is very important. This disease should also be differentiated from nodular scleritis. Differential diagnosis is made on the basis of clinical background factors such as age, ocular pain, sex, onset, and history of allergic conjunctivitis [19, 20]. Previously, IJCN has been characterized by the presence of epithelial inclusion cysts and solid epithelial islands [2, 6] as a variant of a benign conjunctival nevus, a subset of childhood nevi lacking maturation in particular [4, 8,9,10]. The present study also confirmed that IJCN is a benign melanocytic tumor that showed negative staining for Ki-67 and positive staining for Melan A and melanosomes. Infiltration of T cells and macrophages was also observed. Therefore, tacrolimus was expected to be an effective treatment for the inflammation induced by related cytokines. In our cases, the histologic findings may have been affected by the treatment with immunosuppressant eye drops; the resected tissue samples are different from those observed in the active phase. Nonetheless, we would still have observed T cells and macrophages. We hypothesized that more inflammatory cells would be observed before the administration of treatment. The inactive phase of the samples in the excised case might explain the lack of eosinophils in our cases. CD44, a cell surface glycoprotein involved in cell–cell interactions, cell adhesion, and migration, is strongly expressed in IJCN. Whether CD44 may play a role in the pathophysiology of IJCN has not been determined; however, the role of CD44 in IJCN should be clarified in the future. On the basis of the histopathologic findings of IJCN, we speculated that antiallergic agents and immunosuppressants would be effective in treating this disease. Kato and colleagues reported cases in which the use of antiallergic agents alone or in combination with tacrolimus was effective [11]. Administration of antiallergic agents is sometimes effective, but the efficacy depends on the severity and duration of the disease. All our patients were resistant to antiallergic agents and required immunosuppressive agents such as steroids and tacrolimus. However, administration of steroids may lead to complications such as glaucoma in young patients [12, 21]. In fact, two of the seven patients (28.6%) included in the present study had elevated intraocular pressure resulting from the administration of steroid eye drops. Thus, to treat IJCN, the use of immunosuppressant eye drops, such as tacrolimus or cyclosporine, is preferred over steroid eye drops. The administration of immunosuppressant eye drops was successfully tapered in most cases. However, IJCN is an allergy-related disease that occurs at a young age. Thus, treatment should be resumed if signs of recurrence are observed during follow-up.
In conclusion, the present study revealed the clinical and histopathologic characteristics of IJCN, reporting new findings obtained through AS-OCTA and the effectiveness of immunosuppressive agents in the treatment of IJCN.


Comments (0)