Antimicrobial prescribing is a decision-making process involving different factors and actors in NHs. Our results confirm what has already been described in the literature, despite geographical differences.
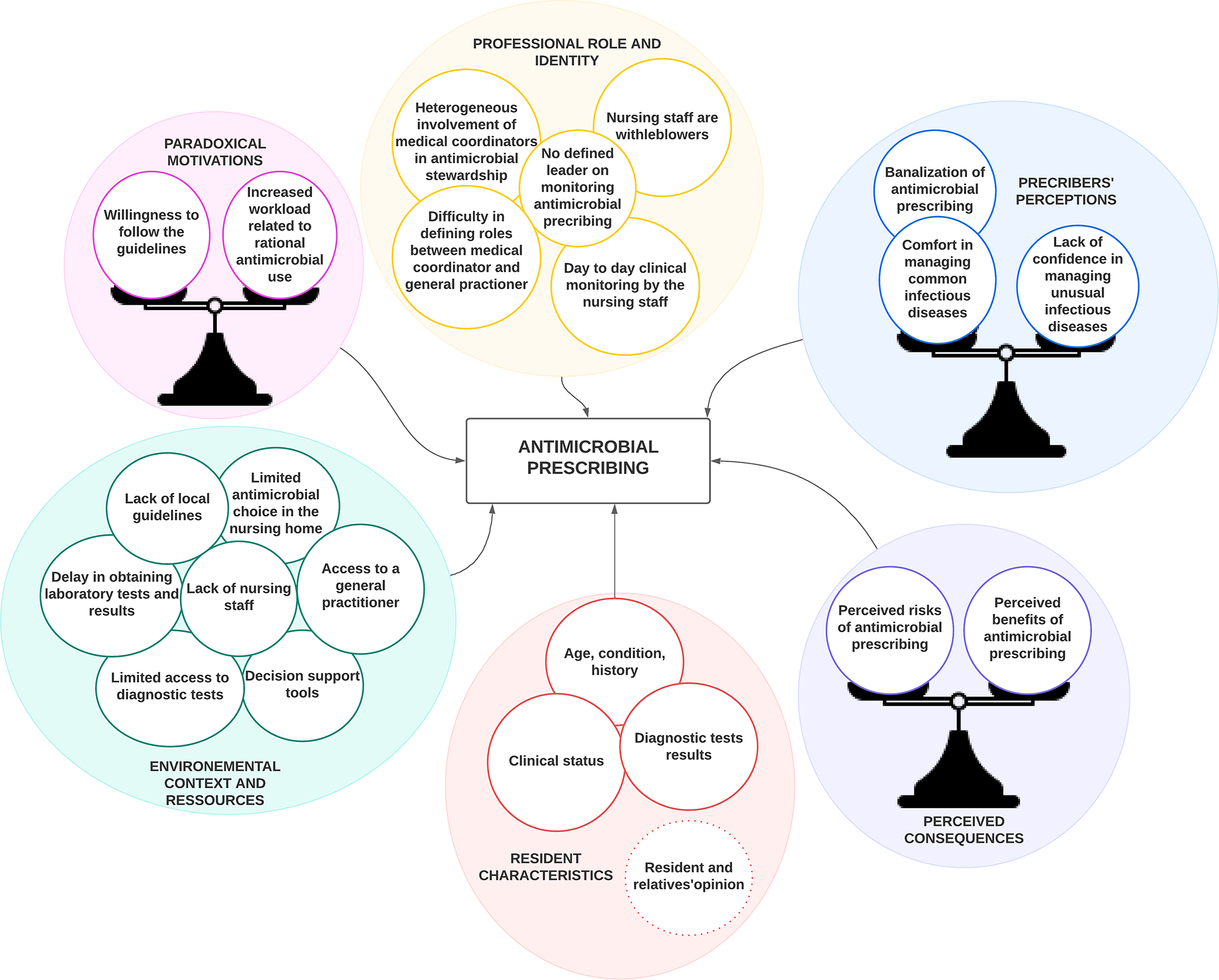
Resident characteristics (age, condition and history) was mentioned by all the participants. They placed particular emphasis on swallowing disorders which, to our knowledge, have not been described in the literature. However, it influences antimicrobial selection, which may then differ from the guidelines. Recent studies suggest that advanced age and comorbidities (e.g. history of infection and indwelling urinary catheters), potential signs of infection, or limited life expectancy tend to increase overall prescribing rate and inappropriate antimicrobial prescribing [3, 20, 22, 37]. Indeed, as interviewed physicians pointed out, perceived risk of infectious complications and discomfort among frail NH residents probably encourages antimicrobial prescribing.
AMS interventions targeting diagnoses process could help physicians to perform the right tests on the right patients and thus help them to make an accurate diagnosis and prescribing in particular clinical situations [38]. However, the fact that most of the interviewed physicians do not perceive difficulty in diagnosing and treating common infectious situation is a major barrier to the acceptability of these interventions.
Contrary to what has been described in the literature, few physicians in our sample felt pressure from nursing staff, families, or residents to prescribe antimicrobials [24, 39,40,41,42,43]. In our study, the lack of patient participation in decision-making seemed to be associated with the high prevalence of cognitive impairment in this population, but it could also be related to the lack of medical knowledge and high acceptability of care by these patients [43].
Participants also emphasized the influence of the environmental context and resources on antimicrobial prescribing. Indeed, the difficulty in obtaining microbiological samples, the lack of available GP, the lack of paramedical staff to monitor follow-up, the lack of guidelines tailored to the NH’s context and the limited access to some antimicrobials (notably those exclusively delivered at hospital) were perceived as hindering improvement in the management of infectious diseases in NHs. Those constraints accentuated situations of doubt and increased the perceived benefits of antimicrobial prescribing compared to its risks.
Participants considered that local and general guidelines tailored to NHs’ context and to the characteristics of institutionalized people could help improving proper antimicrobial use. International published guidelines on the management of infectious diseases in NHs are scarce [44,45,46,47] and often focus on one type of infection. The physicians never mentioned French guidelines for NHs as a reference [48], suggesting it might not be adapted to their needs or not well spread. It could thus be interesting to create a single document gathering the guidelines for the most frequent infections physicians encountered in NHs. These guidelines should consider the context of NHs where limited diagnostic tests and antimicrobials are available. It should also include antimicrobial prescribing in palliative care situations. Physicians also insisted on the utility of a CDSS like Antibioclic. Once appropriate guidelines available, it would be a good way to promote proper antimicrobial use since it seems to be well implemented, already highly used by physicians in NHs and have proven its effectiveness in literature [17].
The professional role of nurses and medical coordinators where identified as a key determinant of antimicrobial prescribing by participants. Nurses are the ones who alert physicians, monitor and follow up residents. They play a key role even if they don’t take the decision or the responsibility for antimicrobial prescribing. Therefore, AMS interventions focusing on accountability by straightening the roles of nurses seemed relevant to this study and to the literature attesting the central role of nursing staff in AMS [49,50,51]. Interventions could reinforce their current role (e.g. clinical assessment, performing tests) or enhance their skills (e.g. prescribing microbiological samples, adapt antimicrobial therapy). Recent studies suggest that nurses feel able to take on such responsibilities, particularly when they are experienced nursing home nurses [52, 53]. One way of improving these AMS interventions would be, as participants suggested, to offer training sessions on the various aspects antimicrobial prescribing in order to ensure quality and safety of their new role. Nurses are already enthusiastic about taking part in training sessions [49]. It could also tend to bring doctors and nurses up to the same level of knowledge and thus improve the shared medical decision, as long as there is good inter-professional communication. However, the lack of nursing staff added to work-overload and high turnover could limit the implementation of that kind of intervention.
The medical coordinators definitively have a role to play in AMS. However, this role was often neglected according to participants and did not appear among medical coordinators’ top priorities. It is essential to effectively train them to take the lead on AMS. Then, they could promote AMS interventions and develop and formalize interprofessional relationship on the territory. Besides, the presence of a coordinating physician shoed positive effects on reducing overall antimicrobial prescribing [54].
Some studies focused on aspects of human resources, management or organizational characteristics of NH, and revealed significant links with antimicrobial prescribing [20]. For some of these contextual factors, there is little room for action, particularly as they depend on public authorities and the economic context in which they exist. As a matter of fact, in France, 15% of the NHs don’t employ a medical coordinator and 37.7% reported difficulties in finding human resources, resulting in frequent understaffing [33] and once again limiting the AMS interventions.
Other antimicrobial prescribing determinants emerged from this study. Perceived consequences of antimicrobial prescribing, motivations and prescribers ’perceptions also influence antimicrobial prescribing. Perceived risk of infection complications (e.g. discomfort, deterioration, hospitalization), the fear of not treating an infection when diagnosis is unclear and complementary examinations are not available often prompted physicians to prescribe antimicrobials “just in case” despite the will to follow guidelines. Physicians stated that proper antimicrobial prescribing in NHs required a major effort but was not judged a priority as compared to other medical issues. Added to that is the fact that physicians feel comfortable in dealing with what they consider as common infection (even if the diagnosis and treatment of those conditions can be challenging) probably doesn’t prompt them to reconsider their prescribing habits and behaviors. Yet, prescribing habits are associated to overall prescribing rates and inappropriate antimicrobial prescribing [23].
In addition to actions to improve antimicrobials use, expertise and education, another important intervention suggested by the physician was audit and feedback. It could help physician step back and realize the impact of inappropriate antibiotic prescribing and motivate them changing their practice. Thus, encouraging results have been reported in French interventions based on the development on a list of quantitative and proxy indicators of appropriate antimicrobial prescribing in NHs [55,56,57]. These results are in line with recent systematic reviews that reported positive outcomes of AMS interventions in NHs in terms of overall antimicrobial use, appropriateness of antimicrobials and AMR rates [17,18,19]. Feedback is particularly efficient when: include an injunctive norm; compare prescribing to the lowest prescribers; targeted high prescribers; the source is a supervisor or colleague; it is given more than once; it is delivered both verbally and in writing; and when it includes objectives and action plan [58, 59].
Overall, many AMS intervention already exist and most effective seem to be multimodal. To date, the only intervention that has shown effects one year after intervention has combined clinician education, CDSS and feedback [28]. This could be explained by the fact that it acted on different determinants levels of antimicrobial prescribing. The implementation of those different AMS strategies, according to the interviewed physicians, relied on developing stakeholders’ relationships among NHs, training and education. They all agreed that the medical coordinator should have a central role in the process.
Some primary research articles on AMS interventions in NHs give us information on how AMS strategies were implemented. However, only a few give details on implementation strategies and on effectiveness for both implementation and clinical outcomes [60,61,62,63]. They all mention multimodal implementation strategies among which training and educating stakeholders and developing stakeholders’ relationships that were also cited by the interviewed physicians in our study. According to those studies, other efficient strategies where using evaluative and iterative strategies and providing infrastructure assistance. Raban et al. (2020) reviewed on AMS strategies which included a section on process evaluations of AMS interventions, briefly describing implementation facilitators, barriers, and outcomes from included studies [17]. The main barriers to AMS strategies implementations were similar to those pointed out by physicians in our study. It included a lack of motivation of the physicians to improve prescribing, difficulties in getting physicians to change practices and ensuring adequate training of new staff. They also noted the high baseline level of appropriate prescribing which was difficult to further improve, high physician turnover in the facilities, a lack of buy-in from nurses and family expectations of antimicrobials. There are several options to explore, including adaption to the context which seems to be a major element to consider in the choice of AMS and implementation strategies [30]. Instead of using the same strategies for all, it may be relevant to propose a tool box of those strategies where each medical coordinator could pick up elements that will fit to each specific context.
Because selection of participants was voluntary, the opinions expressed may be skewed toward those who are concerned about these issues. Results of this study are limited by sample size, type of physician, period of time and restricted geographic area. Moreover, when physicians worked in more than one NH, the inquiry did not delve into specific details about each individual nursing home they worked at. This approach may limit the granularity of the information as the conditions and resources in each nursing home could vary. Therefore, our results may not be representative and generalizable to all NHs, especially since we found that environment and professional role influence antimicrobial prescribing. We did not include other populations that are known to influence antimicrobial prescribing such as the nursing staff or the residents and their families.
Despite the limitations mentioned, the strength of this study is that it explored in depth the views of the prescribing physicians in NHs in the aim of proposing AMS interventions tailored to their needs and therefore more easily adopted because of its perceived interest. To ensure transferability and so that readers can judge whether they can apply our findings to their own settings, we have provided detailed descriptions of our research context, participant demographics, and the methods used. By offering this contextual information, readers can better assess the applicability of our results to their specific circumstances. Additionally, the consistency of our findings with existing literature further supports their potential transferability. We are confident that physicians will find valuable insights to improve antibiotic prescribing in nursing homes. It also allows us a deeper understanding of the NH’s particular context in order to propose the most appropriate AMS interventions and thus facilitate their implementation. These are essential steps to maximize the chances of promoting proper antimicrobial prescribing in these facilities.



Comments (0)