
Remember me

Thyroid cancer has become the fifth most common cancer in women.[1] Indeed, the incidence rate of thyroid cancer is almost 2.6 times higher in females than in males.[2] In the United States, the female age-adjusted incidence rate of thyroid cancer has risen from 6.15/105 in 1980 to 19.72/105 in 2017.[3] In China, the female age-standardized incidence rate of thyroid cancer increased from 4.35/105 to 15.81/105 from 2005 to 2016.[4,5] Among all types of thyroid cancer, differentiated thyroid cancer (DTC) accounts for approximately 95%.[6]
DTC is very common in women of reproductive age. Statistics from World Cancer Observatory indicate that thyroid cancer is the third most common cancer in women aged 25–45 years.[7] Compared with nonpregnant women, pregnant women have an increased release of human chorionic gonadotropin and estrogen, with the former having a function similar to that of thyroid-stimulating hormone (TSH),[8,9] and the latter potentially affecting the proliferation and growth of thyroid cancer cells via mitogen-activated protein kinase (MAPK) cytoplasmic signaling.[10] Thus, the potential association between pregnancy and DTC progression has drawn much attention from both clinicians and patients.
Relevant studies on the present topic have been heterogeneous in study design, population, outcome measures, and findings. To our knowledge, only one systematic review has focused on examining the prognosis of DTC potentially associated with pregnancy.[11] However, this systematic review only included four studies with a comparison group, and the included patients were diagnosed during pregnancy from 1994 to 2010. Moreover, one of the studies included in the review suggested a higher rate of recurrence in patients with DTC related to pregnancy compared with the nonpregnancy, whereas the remaining three studies showed no significant difference in the prognosis of pregnancy-related DTC between pregnancy and nonpregnancy groups. Furthermore, there has been no systematic review quantitatively synthesizing the association of pregnancy with recurrence of previously treated DTC by using the meta-analytic technique.
To fill this research gap, this study aimed to conduct a systematic review and meta-analysis to quantitatively summarize the most up-to-date studies and determine whether pregnancy is associated with disease recurrence in patients previously treated for DTC. We also performed several subgroup and sensitivity analyses to elucidate whether the study design and response to therapy status modifies main study findings.
Methods Search strategyThe present systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines,[12] and the prespecified protocol was registered at PROSPERO (No. CRD42022367896, https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022367896). We systematically searched the PubMed, Embase, Web of Science, Cochrane, and Scopus databases until February 1, 2023. Our search strategy combined MeSH terms and variations of the free terms “Thyroid Cancer” and “Pregnancy” (see details in Supplementary Material, https://links.lww.com/CM9/B888).
Study selectionWe selected studies based on the PICOS framework: (1) Population–patients diagnosed with DTC before pregnancy; (2) Intervention–patients initially treated (operation with/without radioactive iodine [RAI] treatment) before pregnancy; (3) Comparison–studies designed with or without a comparison group; (4) Outcomes–studies reporting recurrence of DTC; and (5) Study design–studies with nonpregnant subjects as the comparison group or studies using the single-group design (without a comparison group). We excluded (1) case reports; (2) studies failing to identify the time of diagnosis or initial treatment of DTC; (3) studies published in languages other than English; and (4) studies without full text.
Quality assessmentOverall, we assessed the quality of the included studies based on the study design, and studies with a comparison group were rated as having higher quality than those single-group studies. We adapted the rating criteria for the two study designs separately [Supplementary Tables 1, 2, https://links.lww.com/CM9/B888] according to revised U.S. Preventive Services Task Force criteria.[13] For studies with a comparison group, we set three criteria: (1) study subjects were comparable in age at pregnancy and disease severity (assessed by Tumor Node Metastasis [TNM] stage/American Thyroid Association [ATA] risk stratification/response-to-therapy status) at baseline between the pregnant group and nonpregnant group; (2) studies adequately controlled the potential confounders of age at pregnancy and disease severity (assessed by TNM stage/ATA risk stratification/response-to-therapy status) by using multivariate analyses; and (3) studies prespecified and defined outcomes of disease recurrence. Studies that met all three criteria were rated as “good”, two as “fair”, and one or none as “poor”. For single-group studies, those that accurately ascertained confounders and predefined outcomes were rated as “fair”; those that met only one of the two criteria or neither were graded as “poor”.
Data extractionTwo researchers with rich experience in public health (Rui Shan) and clinical practice (Xin Li) extracted the following information from the included studies: (1) basic characteristics—study design, country, enrollment, sample size in the pregnancy and nonpregnancy groups, and sample age; (2) pregnancy and DTC information—diagnosis-to-pregnancy and treatment-to-pregnancy interval time, response to therapy, clinicopathology (histology, conditions of extrathyroidal extension, lymph node metastasis, and distant metastasis) at baseline, and follow-up time; and (3) primary outcomes—number and proportion of recurrence, type of recurrence (structural or biochemical), the adjusted risk ratio (RR), and the hazard ratio (HR).
Definitions of recurrence and response to therapy statusRecurrence of DTC was classified into structural recurrence and biochemical recurrence. Structural recurrence was defined as the appearance of new local/metastatic lesions or a 20% or more increase in size of the existing lesion before pregnancy.[14,15] Biochemical recurrence was defined as a 20–25% or more increase in the serum thyroglobulin (Tg) concentration and/or an increase of 20–25% or more in the serum anti-Tg antibody concentration compared with the prepregnancy level.[14,16]
Response to therapy status was classified into four categories defined by the 2015 ATA[17] (for patients treated with total thyroidectomy and radioiodine remnant ablation) and Momesso et al[18] (for patients treated with lobectomy or total thyroidectomy without radioiodine remnant ablation): excellent, indeterminate, biochemical incomplete, and structural incomplete response.
Data analysisFirst, we pooled single proportions for DTC recurrence in pregnant women by using a generalized linear mixed model. We compared proportions of DTC recurrence between (1) structural and biochemical recurrence and (2) different follow-up times (below or above five years) by the chi-squared test. In addition, we conducted a trend test to examine whether the presence of a trend of a higher risk of DTC progression was associated with weaker response to therapy among the four groups of response status in subgroup analyses. We applied double arcsine transformation to resolve issues of computational error due to rare events (no events were observed in a high proportion of the studies).[19,20] Second, we pooled the odds ratio (OR) to compare the proportion of disease recurrence in the pregnancy group with that in the nonpregnancy group by using the Mantel–Haenszel method with random effects variants (“metabin” function in R package “meta”). We also contrasted the OR of recurrence in studies with a comparison group based on the follow-up time (below or above five years). Third, we evaluated heterogeneity between studies with I2 statistics and chose a random effects model for estimation. Based on Cochrane Handbook, we set the rough thresholds for interpretation of I2 statistics as follows: 0–30%—unimportant heterogeneity; 30–50%—moderate heterogeneity; 50–75%—substantial heterogeneity; 75–100%—considerable heterogeneity.[19] Finally, we drew a funnel plot and conducted Egger’s test to assess potential publication bias when the number of studies was greater than or equal to ten. Data analysis was conducted in R (https://www.r-project.org/, version 4.2.1).
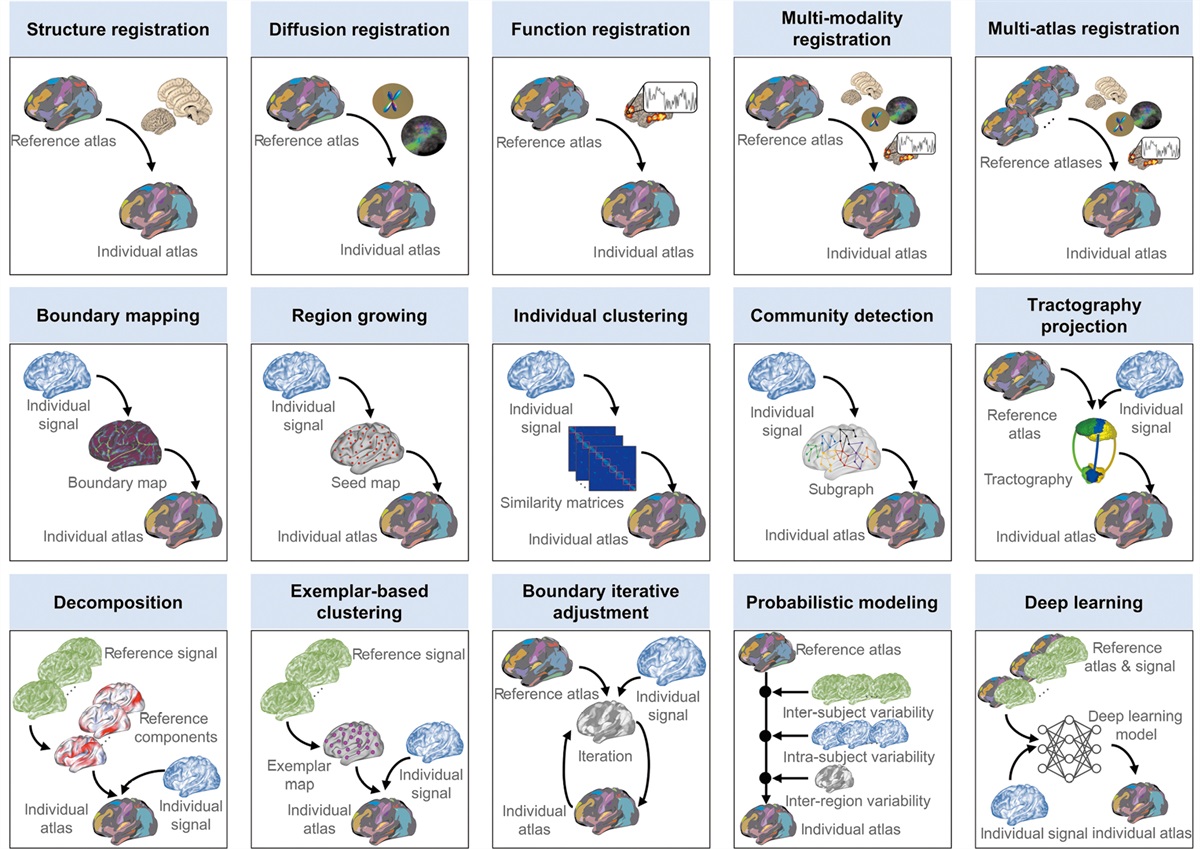
Results Study selectionAs shown in Figure 1, a total of 5266 studies were identified from databases (PubMed: 720, Cochrane: 3, Embase: 869, Web of Science: 1747, and Scopus: 1927). Then, we conducted duplicate elimination (n = 2098 removed), abstract screening (n = 3125 excluded), report retrieval (n = 5 excluded) and full-text screening (n = 28 excluded). Finally, four studies with a comparison group[15,16,21,22] and six single-group studies[14,23–27] were included in our systematic review.
 Figure 1:
Figure 1: Literature flow diagram of study selection.
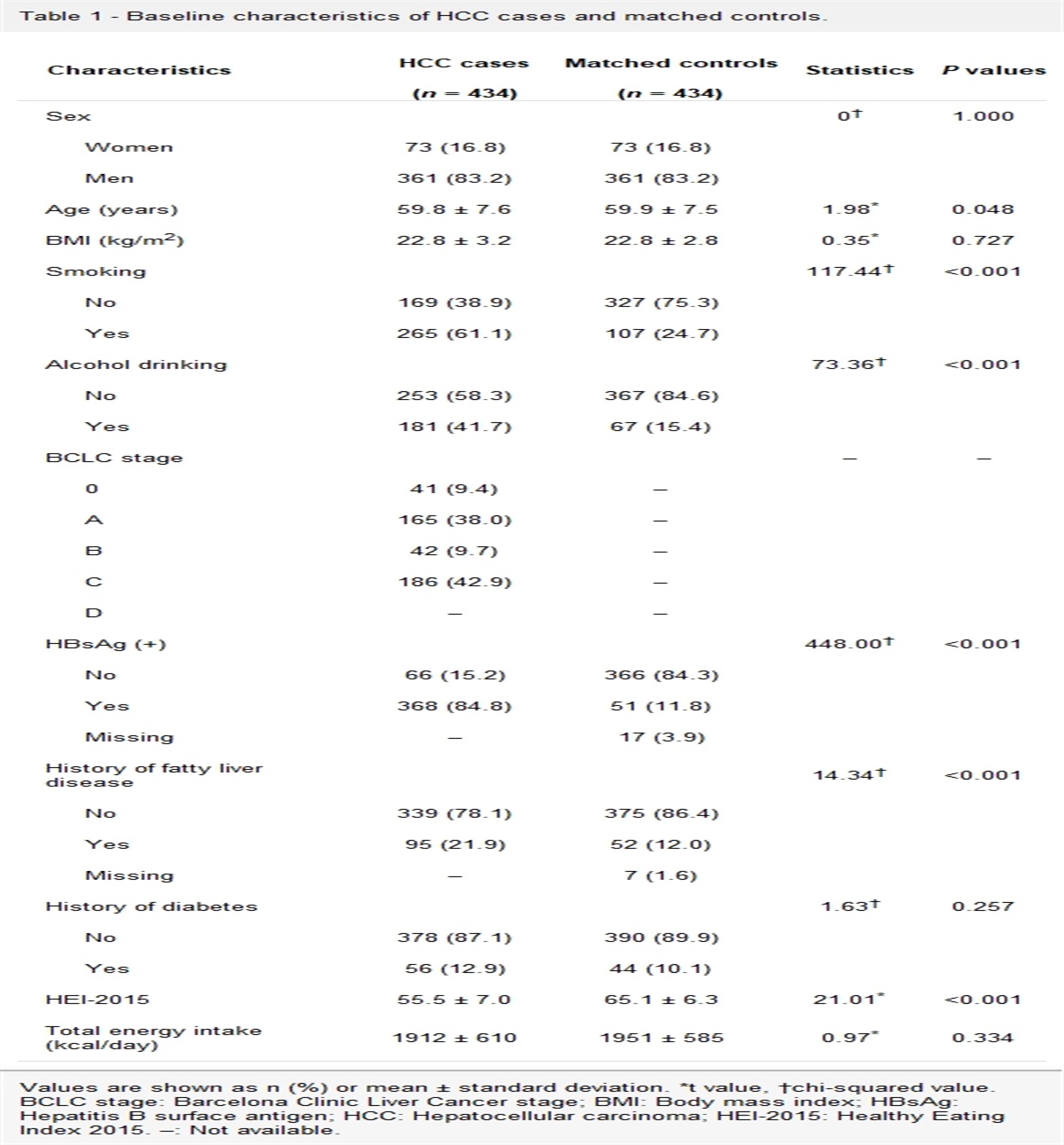
Study characteristicsThe basic characteristics of the ten included studies are shown in Table 1. The studies were conducted in the USA, Brazil, Israel, Turkey, Morocco, China, Italy, and Japan. The sample size of the ten studies ranged from 8 to 235, with participants’ age at pregnancy or delivery ranging from 28 to 35 years. The follow-up time varied from 0.1 to 36 years. Table 2 shows the detailed clinicopathological characteristics, including papillary or follicular thyroid cancer type, extrathyroidal extension, lymph node metastasis, distant metastasis, and response to therapy of the participants. Supplementary Tables 1,2 https://links.lww.com/CM9/B888 show the quality of the included studies. Among four studies with a comparison group, three of them were rated as “good” and only one of them as “poor”; among six studies without a comparison group, three of them were rated as “fair” and the other three of them as “poor”.
Table 1 - Characteristics of the included studies regarding the association of pregnancy with DTC recurrence. Study Study design Country Enrollment, n Age at pregnancy or delivery, years Interval time between diagnosis and pregnancy Interval time between initial treatment and pregnancy Follow-up Leboeuf et al [24] Single-group study USA 36 33.6 ± 3.9* (33.5, 24.3–42.2)† NR 5.5 ± 3.8* years 0.3, 0.1–1.7† years Rosario et al [27] Single-group study Brazil 64 32.0, 23.0–39.0‡ NR 30.0, 15.0–74.0‡ months NR Hirsch et al [14] Single-group study Israel 63 29.7 ± 4.7* (29.4, 20.1–41.2)† NR 5.1 ± 4.4* years** 4.8 ± 3.8* (3.8, 0.3–17.3)† years Budak et al [21] Study with a comparison group Turkey Pregnant, n = 36 Control, n = 36 Pregnant, 29.9 ± 5.1* (21.0–40.0)§ 40.5 ± 26.4* (12.0–120.0)§ months NR Pregnant, 6.1 ± 2.5* years Control, 5.2 ± 0.5* years Rakhlin et al [26] Single-group study USA 235 34.0 ± 0.4* (34.0, 20.0–45.0)† 4.9 ± 0.3* (3.0, 0.1–23.0)† years NR 3.0–12.0§ months Driouich et al [22] Study with a comparison group Morocco Pregnant, n = 42 Control, n = 75 Pregnant, 35.0 ± 6.5*,|| NR 4.4 ± 3.1* years Pregnant, 14.5 ± 2.4* month Control, 18.2 ± 3.7* months Nobre et al [25] Single-group study Brazil 76 32.0, 21.0–44.0† 4.8, 0.9–19.0†,¶ years NR 11.0, 1.0–47.0† years Xi et al [16] Study with a comparison group China Pregnant, n = 37 Control, n = 87 Pregnant, 28.6 ± 4.1* (28.0, 22.0–40.0)† NR 46.3 ± 25.7* (42.0, 7.0–102.0)† months 82.0, 25.0–136.0† months Colombo et al [23] Single-group study Italy 8 33.1 ± 4.6* (35.0, 27.0–38.0)† 62.0 ± 43.8* (66.0, 12.0–120.0)† months NR 97.0†† months Yamazaki et al [15] Study with a comparison group Japan Pregnant, n = 28 Control, n = 97 Pregnant, 32.0, 25.0–45.0† 4.8, 0.3–18.9† years 2.1, 0.5–14.5† years Pregnant, 10.9, 4.2–32.5† years Control, 6.6, 0.1–36.0† yearsData are presented as *mean ± SD; †median, range; ‡mean, range; §range or ††mean. ||Age at diagnosis; ¶Interval time between diagnosis and delivery. **Interval time between initial treatment and delivery. DTC: Differentiated thyroid cancer; NR: Not reported; SD: Standard deviation.
In total, ten studies reported 625 patients who became pregnant after diagnosis and initial treatment for DTC, 101 of whom experienced recurrence. The pooled proportion of recurrence in the random effects model was 0.13 (95% confidence intervals [CI], 0.06–0.25; I2 = 0.58 [substantial heterogeneity]) in the pregnant patients previously treated for DTC [Supplementary Figure 1, https://links.lww.com/CM9/B888].
Specifically, four studies[14,24–26] classified recurrence into structural and biochemical types. The proportion of structural and biochemical recurrence in the pregnant DTC patients was 0.06 (95% CI, 0.03–0.11; I2 = 0 [no heterogeneity]) and 0.10 (95% CI, 0.04–0.23; I2 = 62% [substantial heterogeneity]), respectively [Supplementary Figure 2, https://links.lww.com/CM9/B888]. We observed no evidence of a significant difference in the proportion of DTC recurrence between the structural and biochemical types (P = 0.09).
In addition, a total of nine studies reported follow-up time. We found no significant differences (P = 0.50) in the pooled proportion of recurrence between the pregnant DTC patients below (proportion, 0.19; 95% CI, 0.10–0.35) and above (proportion, 0.15; 95% CI, 0.05–0.36) the 5-year follow-up [Supplementary Figure 3, https://links.lww.com/CM9/B888].
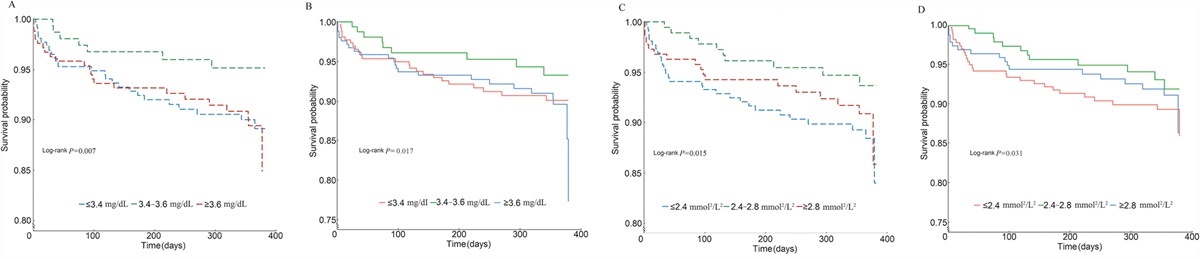
Furthermore, six studies[14,23–27] described response to therapy status before pregnancy. The pooled proportion for recurrence in the pregnant DTC patients was 0.00 (95% CI, 0.00–0.05), 0.09 (95% CI, 0.00–0.73), 0.14 (95% CI, 0.11–0.18), and 0.41 (95% CI, 0.06–0.81) for those with excellent (n = 287), indeterminate (n = 44), biochemical incomplete (n = 41), and structural incomplete response (n = 70), respectively [Figure 2]. We observed a trend for a higher risk of recurrence in order of excellent response, indeterminate response, and biochemical incomplete response and structural incomplete response (trend test, P <0.05).
 Figure 2:
Figure 2: Response to therapy status and the pooled recurrence in pregnant patients. CI: Confidence intervals.
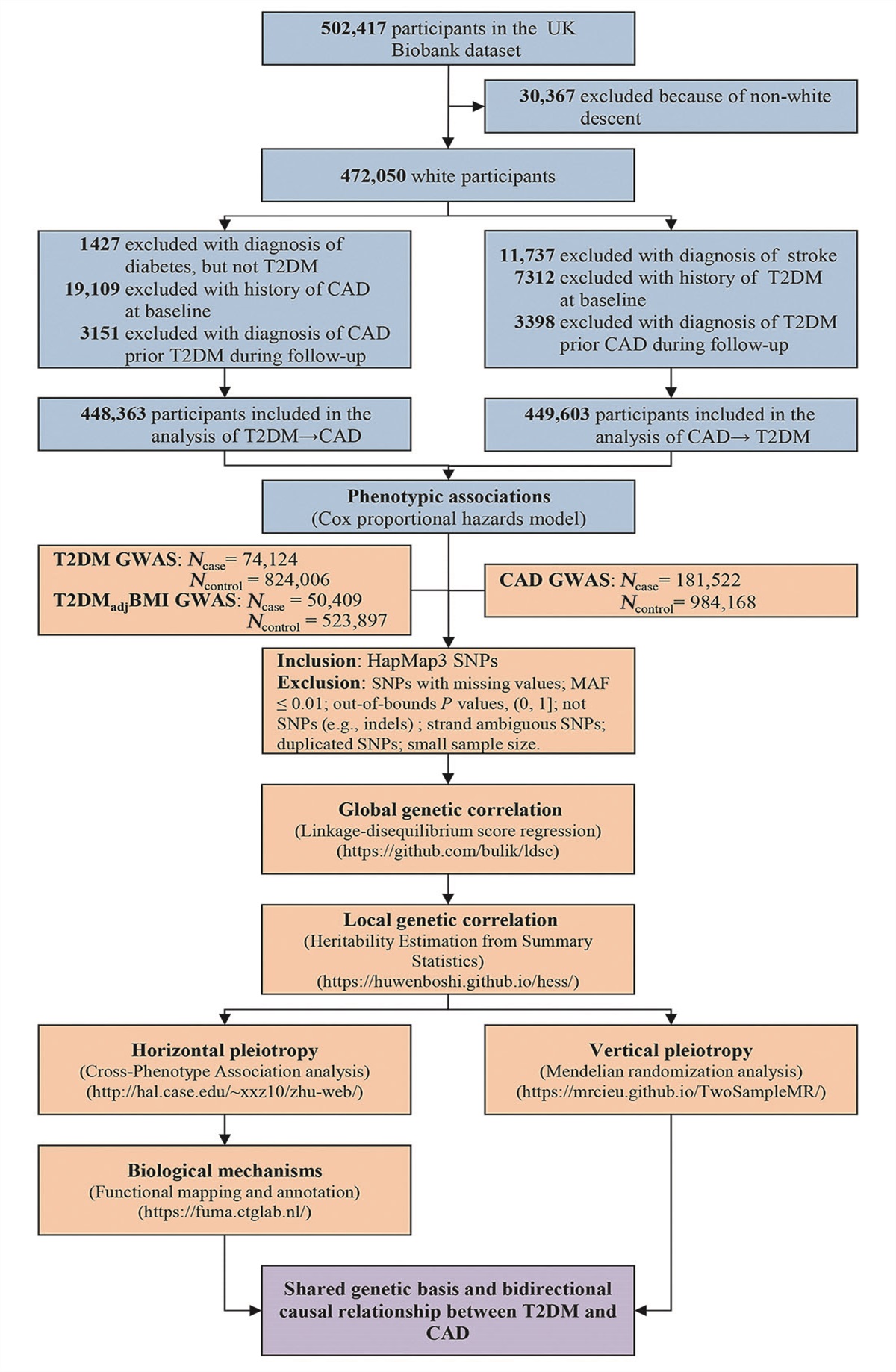
Association of pregnancy with DTC recurrence in studies with a comparison groupAmong four[15,16,21,22] of the ten included studies designed with a comparison group, the OR for recurrence was 0.75 (95% CI, 0.45–1.23; I2 = 0 [no heterogeneity]) when comparing pregnant patients with nonpregnant patients [Figure 3A]. For the two studies[15,16] that focused on DTC patients with distant metastasis, the OR for recurrence was 0.51 (95% CI, 0.14–1.87; I2 = 59% [substantial heterogeneity]) when comparing pregnancy and nonpregnancy groups [Figure 3B]. In multivariate analyses, Driouich et al[22] reported that the adjusted relative risk (aRR) of pregnancy for disease recurrence was 1.04 (95% CI, 0.91–1.32), and Yamazaki et al[15] showed that the HR of pregnancy for progression-free survival was 0.268 (95% CI, 0.061–1.181) (P >0.05).
 Figure 3:
Figure 3: The pooled recurrence OR. (A) between pregnant patients and nonpregnant controls; (B) in patients with distant metastasis at the time of diagnosis. CI: Confidence intervals; OR: Odds ratio.
Specifically, we found no significant differences (P = 0.47) in the pooled OR for recurrence between three studies with a follow-up over 5 years (OR, 0.62; 95% CI, 0.34–1.12) and one study with a follow-up under 5 years (OR, 0.90; 95% CI, 0.39–2.07) [Supplementary Figure 4, https://links.lww.com/CM9/B888].
Assessment of publication biasThe funnel plot for the proportion of recurrence in pregnant patients was presented in Supplementary Figure 5, https://links.lww.com/CM9/B888. We observed no evidence of publication bias by the visual inspection of the funnel plot and by the Egger’s test (P >0.05).
DiscussionOur study is among the first to systematically review and quantitatively summarize the association between pregnancy and disease progression of DTC after initial treatment. We conducted several sensitivity and stratification analyses, and the overall results consistently indicated that pregnancy might have a minimal association with recurrence of DTC in patients treated before pregnancy.
Our meta-analysis results of the pooled proportion of recurrence in pregnant women (0.13 [95% CI, 0.06–0.25]) were not higher than those in nonpregnant women (0.14–0.41) reported in the literature.[15,16,21,22] In line with this finding, we found no evidence of a significant difference in risk of recurrence of DTC in pregnant women, including those with distant metastasis, from that in nonpregnant women among the included studies with a comparison group. In addition, we found that the difference in follow-up time (below/above 5 years) was not associated with neither the proportion of recurrence in all pregnant patients (P >0.05) nor the OR of recurrence in studies with a comparison group (P >0.05). The complicated mechanisms of thyroid cell regulation include both TSH-dependent and TSH-independent pathways. Although TSH is considered to be a stimulus for thyroid cell growth, there is evidence showing that suppression of TSH may not significantly improve disease recurrence among patients with low-risk thyroid cancer.[28] As such, despite having a weak function similar to TSH, pregnancy-induced human chorionic gonadotropin (HCG) alone may not greatly influence the progression of thyroid cancer.
Furthermore, we detected a trend of elevated risk of disease recurrence from excellent, indeterminate, and biochemically incomplete responses to therapy to structurally incomplete response. The outcome suggested that even if pregnancy may not be significantly related to the disease, more attention is still needed for patients with incomplete responses to therapy during gestation. Our findings support the 2017 ATA guidelines that women with excellent response to therapy do not require additional monitoring but that those with incomplete response (structural or biochemical) do need monitoring during pregnancy.[29]
To our knowledge, there were only three reviews of the present topic, among which we only found one systematic review conducted in 2011.[11] However, only four studies were included, and the patients were diagnosed during pregnancy or within 12 months postpartum. None of the previous reviews conducted quantitative analyses, making it difficult to conclude the association of pregnancy with DTC progression. More subsequent studies have been conducted after that systematic review. For example, two Italian studies reported a higher risk of recurrence in patients who were diagnosed with DTC during pregnancy or shortly after delivery.[10,30] However, a Chinese study claimed that pregnancy had no association with prognosis of DTC for patients treated before pregnancy.[16] Discrepancies across studies may be attributed to the variable time of diagnosis (during pregnancy or before pregnancy), study design (single-group study or study with a comparison group), or inclusion of patients with distinct responses to DTC therapy. The research question becomes even more complicated considering those potential confounders. Our study was advantageous in reaching a robust conclusion, as we specifically included previously treated DTC patients before pregnancy, conducted sensitivity analyses among patients with distant metastasis, and performed subgroup analysis based on response to therapy status.
Notably, our finding of little association between pregnancy and DTC progression should be interpreted cautiously. None of the included studies explicitly compared women’s health conditions between the pregnant group and the nonpregnant group. Thus, we could not exclude the possibility that the pregnant women were in relatively good health, which might dilute the association of pregnancy with DTC progression. Several studies mentioned the healthy mother effect, suggesting that women with better health conditions were more likely to conceive.[15,16]
Our study had limitations. First, we only searched citations published in English. Second, almost all included studies were retrospective, leading to potential confounding, selection, information, temporal, and immortal time bias (the period between exposure and data collection was too short for an event to occur, thus influencing the precision of derived associations).[31] Nevertheless, our study comprehensively searched the PubMed, Embase, Web of Science, Cochrane, and Scopus databases. Our study was advantageous in systematically and quantitatively summarizing the correlation between pregnancy and disease progression among previously treated DTC patients by using a meta-analytic technique. Furthermore, we performed several subgroup and sensitivity analyses considering the potentially confounding effect response to therapy status before pregnancy and original disease stage (with or without distant metastasis) on disease recurrence, which increased the robustness of our findings.
Our study has important implications for future research. First, we suggest that future studies answer the present research question by comparing the pregnancy group with the nonpregnancy group. In this way, we may be able to elucidate whether DTC recurrence is due to the pregnancy process itself or simply a natural process of DTC in both pregnant and nonpregnant patients. Second, we suggest that future studies increase the sample size to ensure sufficient statistical power. Third, to estimate the unbiased exposure–outcome association, confounding factors such as age at pregnancy and TNM stage/ATA risk stratification/response-to-therapy status should be adequately controlled by using multivariate analyses. Fourth, the definition of recurrence and its structural or biochemical type should be ascertained and prespecified clearly.
Our study also has clinical implications. Clinicians should provide personalized suggestions to patients of childbearing age with DTC based on their response to therapy status before pregnancy. For patients with incomplete response to therapy before pregnancy, active monitoring of disease progression is strongly suggested during pregnancy; by contrast, for those with excellent or indeterminate response, pregnancy might not need to be postponed and the active monitoring is probably not necessary during pregnancy.[29]
In conclusion, our up-to-date systematic review showed that overall, pregnancy appears to have a minimal correlation with the recurrence of DTC with initial treatment. Clinicians should pay more attention to progression of DTC among pregnant women with biochemical and/or structural persistence.
FundingThe study was funded by National Natural Science Foundation of China (No. 82373694), Young Elite Scientists Sponsorship Program by CAST (No. 2023QNRC001), the Beijing Office for Education Sciences Planning (No. BECA23111), and the Fundamental Research Funds for the Central Universities (No. BMU2021YJ030).
Conflicts of interestNone.
References 1. Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021;71:209–249. doi: 10.3322/caac.21660.
Comments (0)