
Remember me
Small fiber pathology is defined as clinical symptoms of small nerve fiber impairment accompanied by signs of small fiber damage on functional or conduction and/or morphological level.10 Damage to the small caliber nerve fibers as a hallmark of small fiber pathology is also present in a subgroup of patients with fibromyalgia syndrome (FMS)31,38,49 giving rise to the question, whether FMS equals small fiber neuropathy (SFN).47 There is multilevel evidence for the distinction between FMS and SFN. The traditional clinical description of FMS is deeply located chronic widespread pain with additional symptoms such as depression and fatigue.15,24,55 In SFN, superficial acral burning pain is predominant, accompanied by sensory disturbance and autonomic dysfunction.2 Electrophysiologically evoked potentials investigating A-delta and C nerve fibers and microneurography have provided data supporting a distinction between FMS and SFN in some studies10,11,38,49 while not in others.50,52 Morphologically, loss of skin nociceptors is a confirmed finding in subgroups of FMS patients, which results in distinct innervation patterns.7,9,11,20,46,52 However, clinical investigations so far failed to determine defined differences in FMS subgroups with and without small fiber pathology.12 In contrast, some studies reported no small fiber pathology in FMS patients.14,50,51 On a functional level, elevated thermal perception thresholds were reported in FMS.11,32
The question remains, if clinically applicable characteristics can be found that may help distinguishing FMS from SFN. So far, one study assessed the intergroup difference of patients with FMS with and without small fiber pathology using questionnaire data and reported minor differences.25 We retrospectively studied an extensive data set of women with FMS and SFN who were recruited in 2 previous studies10,11 asking for potentially distinguishing factors to be used in clinical practice.
2. Patients and methods 2.1. PatientsWe retrospectively analyzed clinical data of 158 women with FMS11 and 53 women with SFN,10 who were monocentrically recruited during 2 individual studies at our Department of Neurology, University of Würzburg, Germany. The respective studies were approved by the Ethics Committee of the University of Würzburg (#121/14 and #135/15), and all participants gave written informed consent before study inclusion. For study inclusion, current diagnostic criteria for FMS54,55 and SFN8 were applied. The following inclusion criteria were further observed for both patient groups: adult patients and no hints for polyneuropathy in the neurological examination and nerve conduction studies. Exclusion criteria for both cohorts were as follows: pain of other origin, renal insufficiency, previously diagnosed diabetes mellitus, untreated thyroid dysfunction, acute infection, malignancy within the last 5 years, epilepsy, drug or alcohol abuse, eye diseases or surgery, usage of hard contact lenses, cardiac pacemaker, and pending compensation claims. In the SFN cohort, patients with B12 hypovitaminosis were additionally excluded.10 In the FMS cohort, severe psychiatric disorder currently requiring treatment was another exclusion criterion.11 All patients were interviewed in a standardized manner and neurologically investigated by a neurologist (D.E., N.Ü.). The SFN cohort consists of patients seen as regular inpatients or outpatients at our department. Patients with FMS were recruited for study participation from all over Germany.
2.2. Pain characterizationIndividual pain characteristics were determined by spontaneously reported descriptors of the patients covering pain phenotype (character, intensity, location, radiation, onset, relieving, and aggravating factors) and symptoms accompanying pain. Intensities were reflected on a numeric rating scale (NRS) with 0 = no pain and 10 = worst pain imaginable. To assess the potential influence of disease duration on symptoms and signs, we have performed a subgroup analysis comparing 33 patients with FMS and 32 patients with SFN with a disease duration of ≤5 years. All patients filled in the following standardized pain questionnaires: Neuropathic Pain Symptom Inventory (NPSI),5 Graded Chronic Pain Scale (GCPS),53 and Pain Catastrophizing Scale (PCS).29,41 Pain chronicity was rated on the Mainz Pain Staging System (MPSS).16 For depressive symptoms, the “Allgemeine Depressionsskala” (ADS) was used.34 We further studied analgesic medication and nonpharmacological treatments applied.
2.3. General medical assessmentWe compared data obtained on patients' comorbidities. Family history was recorded in a systematic manner asking patients about neurological diagnoses, FMS or SFN diagnosis, respectively, or similar symptoms in family members, such as parents, grandparents, siblings, own children, as well as the siblings of parents and grandparents. Laboratory data that were cross-compared comprised the oral glucose tolerance test (oGTT), glycosylated hemoglobin (HbA1c), thyroid stimulating hormone (TSH), vitamin B12, and blood count (erythrocytes, leukocytes, thrombocytes, hematocrit, and hemoglobin).
2.4. Small nerve fiber assessmentWe analyzed data on small nerve fiber morphology, function, and electrical conduction collected as follows: (1) intraepidermal nerve fiber density (IENFD) quantified on 6-mm skin punch biopsies taken from the lower leg and upper thigh.45 In both studies, skin biopsies were taken according to a standardized protocol45 and were assessed following published counting rules.21 After fixation and immunoreaction with an antibody against protein gene product-9.5 (Ultraclone RA95101 PGP9.5 1:800; Wellow, Isle of Wight, Great Britain), imaging was performed using a fluorescence microscope (Zeiss Axiophot 2, Jena, Germany). IENFD <5.4 fibers/mm was the distal limit and <8.5 fibers/mm the proximal limit. (2) Corneal nerve fiber length (NFL), density (NFD), and branching (NFB) determined by corneal confocal microscopy (CCM).42 (3) Individual sensory profiles established by quantitative sensory testing (QST) at the dorsal foot.35 (4) Latencies and peak-to-peak amplitudes (PPA), when recording pain-related evoked potential (PREP) at the feet.49 Normative values were used as detailed in Ref. 10 and listed in the respective table. Pain-related evoked potential was performed according to a standardized protocol18,22,49 using 2 superficial and concentric stimulation electrodes on the dorsum of the feet which induce a pinprick sensation. The recording of the potentials was performed with a needle electrode at Cz and 2 reference electrodes at the earlobes (A1–A2) according to international 10 to 20 system.19 Twenty triple pulses with an intensity twice as strong as the individual perception threshold were applied. Ten curves each were averaged and compared for the extraction of first positive peak (N1), following negative peak (P1) and peak-to-peak amplitude.
2.5. Statistical analysisStatistical analysis was performed using IBM SPSS Statistics software version 27 (IMB Deutschland GmbH, Ehningen, Germany). A significance level of P < 0.05 was defined. The Shapiro–Wilk test was used to test for normal distribution. Normally distributed data were analyzed with the Student t test, whereas nonnormally distributed data using the nonparametric Mann–Whitney U test. Categorical data were assessed using Fisher exact test and the χ2 test. Krita (Version 5.1.0; Stichting Krita Foundation, Deventer, Netherlands) was used for graphical data visualization.
3. Results 3.1. Epidemiological characterization of study cohortsTable 1 gives a synopsis of the main epidemiological characteristics of the study cohorts. At symptom onset, patients with FMS were on average 10 years younger than patients with SFN (FMS: median 35.0, 4–65 years; SFN: median 47.0, 12–67 years; P < 0.001). Time until diagnosis was 3 times longer in patients with FMS compared with patients with SFN (FMS: median 8.0, 0–46 years; SFN: median 2.8, 0–20 years; P < 0.001). We found that etiology was potentially genetic in 11 of 53 (20.8%) patients with SFN, potentially metabolic in 17 of 53 patients (32.1%), and potentially autoimmune in 6 of 53 patients (11.3%). In 19 of 53 patients with SFN (35.9%), etiology remained idiopathic.
Table 1 - Epidemiological characteristics of study cohorts. FMS SFN P No. of patients 158 53 NA Median age in years [range] 51.5 [21.6–74.8] 53.4 [22.4–73.2] n.s. Median age at symptom onset [range] 35.0 [4–65] (n = 158) 47.0 [12–67] (n = 52) P < 0.001 Median age at diagnosis [range] 45.5 [19.6–67.3] 53.2 [20.4–73.2] P < 0.001 Median disease duration in years [range] 15.8 [0.0–56.0] 4.0 [0–20.0] P < 0.001 Median time in years between symptom onset and diagnosis [range] 8.0 [0–46] 2.8 [0–20] P < 0.001FMS, fibromyalgia syndrome; NA, not applicable; n.s., not significant; SFN, small fiber neuropathy.
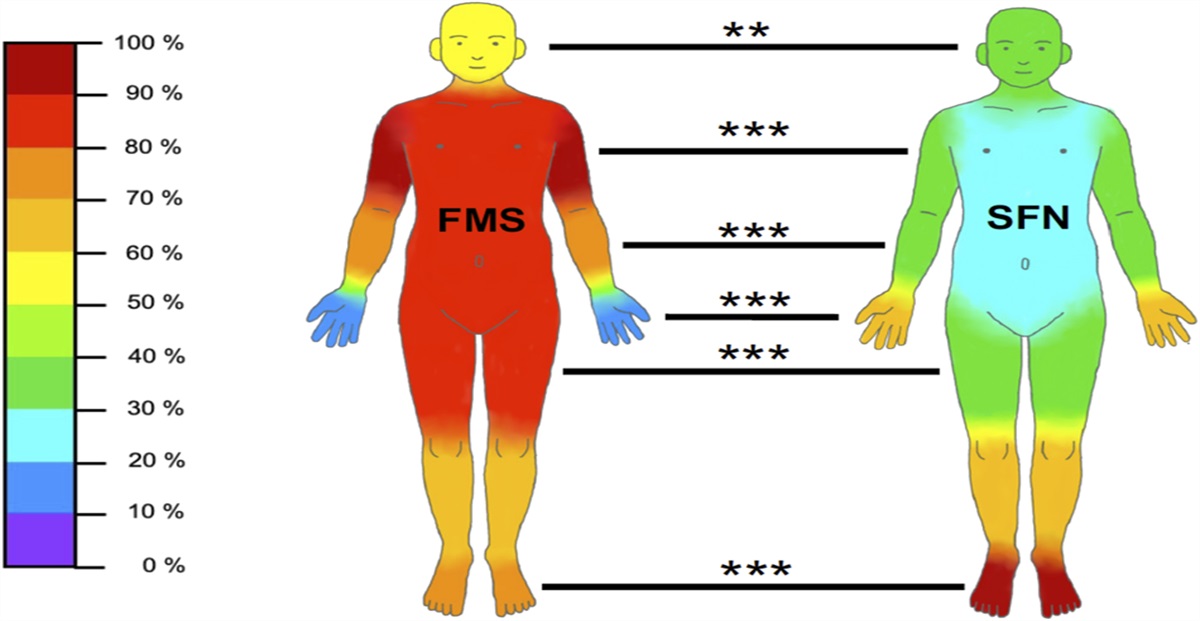
Table 2 shows pain characteristics of patients with FMS and SFN. During pain interviews, the main discriminators between the 2 entities were burning (FMS: 66/158 [41.8%], SFN: 45/53 [84.9%], P < 0.001) or stabbing pain (FMS: 39/158 [24.7%], SFN: 35/53 [66.0%], P < 0.001). Patients with FMS further described pain like muscle soreness (40/158, 25.3%). Pain localization also distinguished well between FMS and SFN with widespread pain being predominant in FMS and acral pain in patients with SFN (Fig. 1). In FMS, physical activity, rest, and warmth alleviated pain, whereas cold and stress evoked pain (Table 2). In contrast, patients with SFN reported cold, warmth, and touch as both pain relieving and triggering factors (Table 2). Furthermore, patients with FMS reported a higher number of aggravating factors compared with patients with SFN (FMS: 2.3 [0–6], SFN: 1.6 [0–5], P < 0.001). When using pain questionnaires, the NPSI pressure score (FMS: median 0.5 [0.0–1.0], SFN: median 0.3 [0–0.9], P < 0.001), evoked pain score (FMS: median 0.4 [0–0.9], SFN: median 0.3 [0–0.9], P < 0.001), and GCPS pain intensity (FMS: median 66.7 [26.7–90.0], SFN: median 56.7 [13.3–86.7], P < 0.001) discriminated best between FMS and SFN (Table 3). Interview data are summarized in Figure 2.
Table 2 - Pain characteristics of patients with fibromyalgia syndrome and small fiber neuropathy (elicitation by interview). FMS SFN P Median pain intensity on NRS [range] During interview 5.0 [0–9] (n = 156) 4.0 [0–9] (n = 53) <0.01 After pain medication 2.0 [0–6] (n = 126) 1.0 [0–1] (n = 40) <0.001 Pain character Burning 66/158 (41.8%) 45/53 (84.9%) <0.001 Stabbing 39/158 (24.7%) 35/53 (66.0%) <0.001 Tearing 16/158 (10.1%) 8/53 (15.1%) n.s. Pain localization Head 91/158 (57.6%) 16/52 (30.8%) <0.01 Neck 141/158 (89.2%) 18/52 (34.6%) <0.001 Shoulders/upper arm 151/158 (95.6%) 18/52 (34.0%) <0.001 Elbow/lower arm 112/158 (70.9%) 18/52 (34.0%) <0.001 Hands/fingers 23/158 (14.6%) 34/52 (64.2%) <0.001 Trunk 123/158 (77.8%) 7/53 (13.2%) <0.001 Upper back 131/158 (82.9%) 17/53 (32.1%) <0.001 Lower back 137/158 (86.7%) 22/53 (41.5%) <0.001 Hips 124/158 (78.5%) 16/51 (31.4%) <0.001 Thighs 130/158 (82.3%) 20/53 (37.7%) <0.001 Knees/lower legs 102/158 (64.6%) 37/53 (69.8%) n.s. Feet/toes 115/158 (72.8%) 52/53 (98.1%) <0.001 Pain triggers Heat 4/158 (2.5%) 18/53 (34.0%) <0.001 Cold 106/158 (67.1%) 12/53 (22.6%) <0.001 Stress 101/158 (63.9%) 6/53 (11.3%) <0.001 Humidity 28/158 (17.7%) 1/53 (1.9%) <0.01 Time of day 0/158 (0.0%) 3/53 (5.7%) <0.05 Weather 32/158 (20.3%) 1/53 (1.9%) <0.01 Touch 4/158 (2.5%) 20/53 (37.7%) <0.001 Median number of pain aggravating factors [range] 2.0 [0–6] 2.0 [0–5] <0.001 Pain relieving factors Physical activity 112/158 (70.9%) 12/53 (22.6%) <0.001 Resting 73/158 (46.2%) 10/53 (18.9%) <0.001 Cold 3/158 (1.9%) 7/53 (13.2%) <0.01 Heat 129/158 (81.6%) 9/53 (17.0%) <0.001 Touch 1/158 (0.6%) 5/53 (9.4%) <0.01 Median number of pain relieving factors [range] 2.0 [0–4] 1.0 [0–3] <0.001FMS, fibromyalgia syndrome; NRS, numeric rating scale; n.s., not significant; SFN, small fiber neuropathy.
 Figure 1.: Proportion of patients who reported pain in distinct body areas. The graph depicts the frequency of pain reported in distinct body areas in relation to the FMS (n = 158) and SFN (n = 53) patient groups. For exact data, please see Table 2. FMS, fibromyalgia syndrome; SFN, small fiber neuropathy. **PP
Table 3 -
Pain characteristics of patients with fibromyalgia syndrome and small fiber neuropathy (elicitation by questionnaires and Mainz Pain Staging System).
FMS
SFN
P
NPSI
Sum score: mean [range]
0.4 [0.1–0.9]
0.4 [0.0–0.7]
<0.05
Burning score: median [range]
0.5 [0–10.0]
0.4 [0.0–0.9]
n.s.
Pressure score: median [range]
0.5 [0–10.0]
0.3 [0.0–0.9]
<0.001
Attack score: median [range]
0.4 [0.0–1.4]
0.4 [0–10.0]
n.s.
Evoked pain score: median [range]
0.4 [0.0–0.9]
0.3 [0.0–0.9]
<0.001
Paresthesia/dysesthesia score: median [range]
0.4 [0.0–1.0]
0.6 [0–10.0]
n.s.
Discriminative score: mean [range]
54.3 [23.4–95.2]
51.2 [28.6–79.3]
n.s.
GCPS: median [range]
Pain intensity
66.7 [26.7–90.0]
56.7 [13.3–86.7]
<0.001
Disability
60.0 [10.0–86.7]
50.0 [3.3–100.0]
<0.05
Grade
2.0 [1–4]
2.0 [0–4]
n.s.
ADS median [range]
23.0 [3–51]
17.0 [2–38]
<0.001
PCS median [range]
22.2 [0–49]
21.2 [3–41]
n.s.
Classification according to MPSS
Median [range]
3.0 [2–3]
3.0 [1–3]
<0.05
Figure 1.: Proportion of patients who reported pain in distinct body areas. The graph depicts the frequency of pain reported in distinct body areas in relation to the FMS (n = 158) and SFN (n = 53) patient groups. For exact data, please see Table 2. FMS, fibromyalgia syndrome; SFN, small fiber neuropathy. **PP
Table 3 -
Pain characteristics of patients with fibromyalgia syndrome and small fiber neuropathy (elicitation by questionnaires and Mainz Pain Staging System).
FMS
SFN
P
NPSI
Sum score: mean [range]
0.4 [0.1–0.9]
0.4 [0.0–0.7]
<0.05
Burning score: median [range]
0.5 [0–10.0]
0.4 [0.0–0.9]
n.s.
Pressure score: median [range]
0.5 [0–10.0]
0.3 [0.0–0.9]
<0.001
Attack score: median [range]
0.4 [0.0–1.4]
0.4 [0–10.0]
n.s.
Evoked pain score: median [range]
0.4 [0.0–0.9]
0.3 [0.0–0.9]
<0.001
Paresthesia/dysesthesia score: median [range]
0.4 [0.0–1.0]
0.6 [0–10.0]
n.s.
Discriminative score: mean [range]
54.3 [23.4–95.2]
51.2 [28.6–79.3]
n.s.
GCPS: median [range]
Pain intensity
66.7 [26.7–90.0]
56.7 [13.3–86.7]
<0.001
Disability
60.0 [10.0–86.7]
50.0 [3.3–100.0]
<0.05
Grade
2.0 [1–4]
2.0 [0–4]
n.s.
ADS median [range]
23.0 [3–51]
17.0 [2–38]
<0.001
PCS median [range]
22.2 [0–49]
21.2 [3–41]
n.s.
Classification according to MPSS
Median [range]
3.0 [2–3]
3.0 [1–3]
<0.05
ADS, allgemeine depressionsskala; FMS, fibromyalgia syndrome; GCPS, Graded Chronic Pain Scale; MPSS, Mainz Pain Staging System; NPSI, Neuropathic Pain Symptom Inventory; n.s., not significant; PCS, Pain Catastrophizing Scale; SFN, small fiber neuropathy.
 Figure 2.: Clinical aspects distinguishing FMS and SFN. The plot summarizes the most important opposing aspects that can be collected during interview. The figurines showing the pain localization are taken from Figure 1. The exact data can be found in Tables 1, 2, 4, 5 and 7. FMS, fibromyalgia syndrome; SFN, small fiber neuropathy.3.3. Patients with fibromyalgia syndrome report sleep disturbance and depressed mood, whereas patients with small fiber neuropathy mainly suffer from sensoalgesic symptoms
Figure 2.: Clinical aspects distinguishing FMS and SFN. The plot summarizes the most important opposing aspects that can be collected during interview. The figurines showing the pain localization are taken from Figure 1. The exact data can be found in Tables 1, 2, 4, 5 and 7. FMS, fibromyalgia syndrome; SFN, small fiber neuropathy.3.3. Patients with fibromyalgia syndrome report sleep disturbance and depressed mood, whereas patients with small fiber neuropathy mainly suffer from sensoalgesic symptoms
We evaluated patients' comorbidities and further symptoms, an overview is given in Table 4. The average number of additional symptoms spontaneously reported by the patients was higher in patients with FMS than in patients with SFN (FMS: median 8.0 [0–28], SFN: median 4.0 [0–14], P < 0.001). Patients with FMS rarely reported paresthesias, whereas patients with SFN often described tingling (FMS: 26/158 [16.5%], SFN: 36/53 [67.9%], P < 0.001), numbness (FMS: 19/158 [12.0%], SFN: 15/53 [28.3%], P < 0.01), or hypersensitivity to touch (FMS: 1/158 [0.6%], SFN: 7/53 [13.2%], P < 0.001). Patients with FMS more frequently suffered from gastrointestinal and urogenital symptoms than patients with SFN (Table 4). Patients with FMS also more frequently described sleep problems (Table 4), fatigue (FMS: 139/158 [88.0%], SFN: 3/53 [5.7%], P < 0.001), or apathy (FMS: 24/158 [15.2%], SFN: 2/53 [3.8%], P < 0.01). They reported cognitive impairment (FMS: 62/158 [39.2%], SFN: 0/53 [0%], P < 0.001) or problems of attention (FMS: 114/158 [72.2%], SFN: 1/53 [1.9%], P < 0.001). Furthermore, patients with FMS more prevalently reported depressed mood (FMS: 29/158 [18.4%], SFN: 1/53 [1.9%], P < 0.01) than patients with SFN.
Table 4 - Additional symptoms and comorbidities in patients with fibromyalgia syndrome and small fiber neuropathy. FMS SFN P Comorbidities Bronchial asthma 20/158 (12.7%) 1/53 (1.9%) <0.05 Migraine with aura 12/158 (7.6%) 3/53 (5.7%) n.s. Migraine without aura 27/158 (17.1%) 1/53 (1.9%) <0.01 Tinnitus 18/158 (11.4%) 1/53 (1.9%) <0.05 Depression 74/158 (46.8%) 6/53 (11.3%) <0.001 Diabetes type 2 0/158 (0.0%) 3/53 (5.7%) <0.05 Sicca syndrome 8/158 (5.1%) 3/53 (5.7%) n.s. Borreliosis 9/158 (5.7%) 3/53 (5.7%) n.s. Hypothyreosis 20/158 (12.7%) 7/53 (13.2%) n.s. Hyperthyreosis 1/158 (0.6%) 1/53 (1.9%) n.s. Hashimoto disease 13/158 (8.2%) 7/53 (13.2%) n.s. Neurological symptoms Numbness 19/158 (12.0%) 15/53 (28.3%) <0.01 Tingling 26/158 (16.5%) 36/53 (67.9%) <0.001 Paresthesias 24/158 (15.2%) 6/53 (11.3%) n.s. Hypersensitivity to touch 1/158 (0.6%) 7/53 (13.2%) <0.001 Hypohidrosis 8/158 (5.1%) 6/53 (11.3%) n.s. Hyperhidrosis 59/158 (37.3%) 28/53 (52.8%) n.s. Conspicuous sweating (hypohidrosis or hyperhidrosis) 66/158 (41.8%) 34/53 (64.2%) <0.01 GI and urogenital symptoms Irritable bladder 25/158 (15.8%) 1/53 (1.9%) <0.01 Obstipation 25/158 (15.8%) 1/53 (1.9%) <0.01 Diarrhea 24/158 (15.2%) 5/53 (9.4%) n.s. Irritable bowel 69/158 (43.7%) 1/53 (1.9%) <0.001 Nausea 1/158 (4.4%) 5/53 (9.4%) n.s. Sleep problems Unrefreshed sleep 81/158 (51.3%) 0/52 (0.0%) <0.001 Sleep disturbance 100/158 (63.3%) 11/53 (20.8%) <0.001 Difficulties in falling asleep 29/158 (18.4%) 2/53 (3.8%) <0.01 Mental symptoms Fatigue 139/158 (88.0%) 3/53 (5.7%) <0.001 Apathy 24/158 (15.2%) 2/53 (3.8%) <0.01 Asthenia 30/158 (19.0%) 6/53 (11.3%) n.s. Agitation 16/158 (10.1%) 1/53 (1.9%) n.s. Irritability 13/158 (8.2%) 1/53 (1.9%) n.s. Depressed mood 29/158 (18.4%) 1/53 (1.9%) <0.01 Cognitive symptoms 62/158 (39.2%) 0/53 (0.0%) <0.001 Concentration problems 114/158 (72.2%) 1/53 (1.9%) <0.001 Other symptoms Limb stiffness 95/158 (60.1%) 3/53 (5.7%) <0.001 Joint swelling 8/158 (5.1%) 9/53 (17.0%) <0.05 Vertigo 19/158 (12.0%) 8/53 (15.1%) n.s. Circulatory problems 12/158 (7.6%) 11/53 (20.8%) <0.05 Palpitations 14/158 (8.9%) 3/53 (5.7%) n.s. Respiratory distress 13/158 (8.2%) 0/53 (0.0%) <0.05 Restless legs 12/158 (7.6%) 2/53 (3.8%) n.s. Total number of additional and spontaneously reported symptoms: median [range] 8.0 [0–28] 4.0 [0–14] <0.001FMS, fibromyalgia syndrome; GI, gastrointestinal; n.s., not significant; SFN, small fiber neuropathy.
Mental disorders (FMS: 30/158 [19.0%], SFN: 3/53 [5.7%], P < 0.05) and chronic pain (FMS: 78/158 [49.4%], SFN: 17/53 [32.1%], P < 0.05) were mostly present in the family history of patients with FMS. In contrast, patients with FMS had fewer relatives suffering from neurological diseases than patients with SFN (FMS: 26/158 [16.5%], SFN: 22/53 [41.5%], P < 0.001). Detailed data and reported diseases are listed in Table 5.
Table 5 - Family history of patients with fibromyalgia syndrome and small fiber neuropathy. FMS SFN P Chronic pain (eg, migraine, joint/back pain, FMS, and rheumatoid arthritis) 78/158 (49.4%) 17/53 (32.1%) <0.05 Neurological diseases (eg, multiple sclerosis, epilepsy, Parkinson disease, polyneuropathy, and dementia) 26/158 (16.5%) 22/53 (41.5%) <0.001 Mental disorders (eg, depression, bipolar disorder, schizophrenia, drug or alcohol abuse, and psychosis) 30/158 (19.0%) 3/53 (5.7%) <0.05FMS, fibromyalgia syndrome; SFN, small fiber neuropathy.
Table 6 shows the results of the blood tests performed. Patients with FMS had lower HbA1c levels compared with patients with SFN (FMS: median 5.4% [4.7–6.4], SFN: median 5.5% [3.6–7.7], P < 0.05). However, data may be biased because diagnosed diabetes mellitus before study inclusion was an exclusion criterion. HbA1c was ≤6.4% in all patients with FMS. In contrast, 3 of 51 (5.9%) patients with SFN had an HbA1c >6.4%,indicating diabetes mellitus (P < 0.05). Although fasting blood glucose levels revealed no difference between the 2 cohorts, abnormalities were evident in the oGTT: after 1 hour (FMS: median 138.0 [68–246] mg/dL, SFN: median 172.0 [89–333] mg/dL, P < 0.01) and 2 hours (FMS: median 120.0 [65–217] mg/dL, SFN: median 123.0 [79–284] mg/dL, P < 0.05), patients with FMS were characterized by lower blood glucose levels than patients with SFN and less frequently had pathological results (2h oGTT >140 mg/dL: FMS: 23/157 [14.6%], SFN: 14/47 [29.8%]). As for TSH and vitamin B12 levels, patients in both cohorts showed normal values.
Table 6 - Blood tests in patients with fibromyalgia syndrome and small fiber neuropathy. FMS SFN P Median [range] HbA1c (%) 5.4 [4.7–6.4] 5.5 [3.6–7.7] <0.05 Fasting blood sugar levels (mg/dL) 95.5 [56–128] 97.0 [74–144] n.s. oGTT 1 h (mg/dL) 138.0 [68–246] 172.0 [89–333] <0.01 oGTT 2 h (mg/dL) 120.0 [65–217] 123.0 [79–284] <0.05 TSH (mU/L) 1.8 [0.0–10.8] 1.6 [0.0–9.2] n.s. Vitamin B12 (pg/mL) 449.5 [183–2000] 470.5 [215–2000] n.s. Pathological test results
Comments (0)