In the setting of malignant neoplastic disease, or irradiated patients, reconstructive options for disarticulation defects pose a significant challenge for the reconstructive surgeon. The options available depend on several factors including the extent of resection, predicted survival, state of dentition and occlusion, economic factors, and surgeon preference. The options that exist are as follows:
First, leave the mandible to ‘swing’ without reconstructing the TMJ. This has the advantage of simplicity and low surgical complication rates, but with large defects, significant functional impairment is likely, with malocclusion, facial asymmetry, and difficulty with chewing and swallowing.
The second option is the use of condylar prosthesis alone to replace the resected condyle. This approach has been shown to preserve facial symmetry, maintain occlusion, and with good case selection may have good short to medium term outcomes[8, 9], but is prone to complications. Key complications from prosthetic condylar replacement only include infection, plate exposure, glenoid fossa perforation, facial nerve injury, and hypertrophic bone formation [10]. Additionally, the condylar attachments to reconstruction plates that are available in the market are currently approved as temporary devices only (TMCRP, 21 CFR 872.4770), for a period of up to 24 months until definitive TMJ reconstruction is performed. However, apart from a formal total joint replacement, there are no rapidly available prosthetic alternatives to this temporary prosthesis.
The third option is direct bony microvascular replacement (Autogenous) of the condyle and ramus which is regarded the gold standard. With the development of microvascular reconstruction techniques, options for reconstruction with autologous bone include the fibula, DCIA (Deep circumflex iliac artery), scapula, second metatarsal-phalangeal joints, and lateral femoral condyle free flaps [11,12,13,14,15]. In the setting of ablative surgery, the fibula free flap has most commonly been used. The main advantage of the fibula is its length allowing for condylar replacement at the same time as potentially angle to angle mandibular reconstruction. Using the fibula alone as a condylar replacement secured to a reconstruction plate achieves similar functional results to a prosthetic condyle, although occlusal control may be more difficult [4, 10, 16, 17]. Although it is the gold standard, it is also associated with significant complications including displacement, ankylosis and malocclusion due to difficulty controlling the occlusion [4, 5, 18, 19]. Additionally, alternative options are needed where a bony free flap of adequate length such as a fibula is not a viable options due to peripheral vascular disease, or vascular anomalies (which was the case in 4 of our patients who underwent scapula reconstructions instead).
A fourth option includes combining the use of prosthetic condyles with microvascular techniques as presented in this series. With the use of virtual planning, a bony free flap secured to the plate along the ascending ramus with a prosthetic condylar component can allow accurate control of vertical ramus height. The main advantage over autologous reconstruction alone is that the prosthetic condyle reduces the risk of ankylosis and heterotopic bone formation, and improves vertical control of the neo-ascending ramus, in turn achieving better control of the post-operative occlusion and hence functional improvement. Few studies have evaluated the use of concurrent free flaps and prosthetic condylar replacements. Bredell et al. reported a series of 15 patients who had condylar reconstruction, among whom 4 had fibula free flaps with metal condylar replacements [10]. These patients had comparable outcomes to those who had autogenous reconstructions extending to the glenoid fossa. These findings are consistent with findings in some recent studies, where condylar prostheses and reconstruction plates with concurrent bony free flap reconstruction including the ascending ramus (type 3), have shown good short to medium-term outcomes [6, 20]. Similar to our findings, the best outcomes with reduced complications were observed when bony reconstruction extended up the ascending ramus. Results are likely to improve with improving technology, with recent studies showing good results when employing virtual planning with CAD-CAM techniques with accurate printed anatomic condyles and accurate ramus height restoration [6, 20]. 3D printing the reconstruction plate with the condylar segment as part of the reconstruction plate would be the ideal way to perform this technique without using the temporary condylar prosthesis currently available.
The authors do not advocate this technique for all cases with mandibular disarticulation, but present it as a viable option that can be considered with appropriate case selection. All of those with significant condylar prosthesis related infections and complications occurred in our series were in malignant cases. Hence, we would caution its use in malignant cases. It can be considered a viable option however in patients where alternative autologous options are not available, and those with a poor prognosis and unlikely long term survival. In our cohort, very challenging cases were managed with this technique with a sustainable functional outcome (see Table 1 and 4). Several of the malignant cases were advanced malignant tumors or high grade recurrences with poor long term expected survival and prognosis (patients 9, 11, 13, 14, 15, 17, 18, 20, 21, 23, 25). Additionally, several of the non malignant cases had no alternative option apart from resection and leaving the mandible to swing such as patient 8 with advanced myositis ossificans and bisphosphonate induced osteonecrosis, and patient 24 who had osteopetrosis since birth who was miserably suffering from chronic osteomyelitis. Resecting the infected side of her mandible and reconstructing her with a reconstruction plate with a prosthetic condyle gave her good function, and significant symptomatic improvement.
In the rare cases where large multi-subunit resections are required necessitating more than one concurrent free flap to reconstruct the defect, having a prosthesis seems to be a recipe for infection and ultimately the need for prosthesis removal. The likely explanation for the increased risk of infection in all of these cases is the amount of dead space around the prosthesis. The dead space fills with haematoma or seroma, an environment highly conducive to bacterial proliferation and resultant infection, especially in the presence of a prosthesis and saliva. The risk seems higher when the prosthesis and reconstruction plate are located between two microvascular free flaps. Special attention should be given to eliminating this dead space with vascularized tissue, either by extending the bony reconstruction (with its associated muscular tissue) as high up the ascending ramus as possible, or using a soft tissue flap (local or distant) to wrap the prosthesis and plate and eliminate the dead space.
Radiotherapy is a relative contraindication for prosthetic condylar reconstruction [10], and post-operative radiotherapy in malignant cases appears to increase the risk of prosthetic infection. However, unexpectedly, it is notable how few complications arose from our cases who underwent prosthetic condylar reconstruction for osteoradionecrosis. The 4 patients in this series all had good outcomes. None had undergone previous mandibular or oral cavity resections, allowing us to preserve the surrounding soft tissue, including the pterygomasseteric sling and the articular disk. This may explain the good outcomes seen in these cases.
Rare complications of prosthetic condyle replacement such as perforation of the glenoid fossa and facial nerve palsy need to also be discussed. Perforation of the temporal bone is a known complication of prosthetic condylar prostheses [3, 8, 9]. Several factors appear to contribute to the risk of glenoid fossa perforation including radiotherapy, articular disk removal and lack of posterior occlusal support [21]. Conversely, more anatomically accurate prostheses may reduce the risk. Virtual planning and CAD-CAM condylar prostheses designed to the mirrored condylar shape with accurate ramus height reconstruction led to better pressure distribution, and avoided maladaptive biodynamic changes to the glenoid fossa and residual joint components as demonstrated by a team in Bologna, Italy [6]. Ipsilateral posterior occlusal support may also reduce vertical condylar pressure on the glenoid fossa from unopposed masticatory forces. Preservation of the articular disk is also critical [9, 20, 21]. In our series, one patient developed a late perforation into the middle cranial fossa following two flap reconstruction for a large mandibular SCC, and was the only patient in our cohort whose resection included the articular disk at the time of resection. She had post-operative adjuvant chemo-radiotherapy, and suffered from recurrent infections. At 4 years after surgery, CT imaging demonstrated perforation of the prosthesis through the glenoid fossa. The prosthesis was removed without complication. Careful case selection and pre-operative planning is needed to reduce the risk of glenoid fossa perforation. A glenoid fossa prosthetic component could be considered for the prosthetic head to not directly contact the bone of the glenoid fossa. This should be seriously considered in cases where the articular disk is sacrificed in the resection.
Facial nerve injury in patients with prosthetic condylar replacements have also been reported [3, 10], and occurred in 2 of our patients. Both had radiotherapy and recurrent infections associated with the condylar prosthesis. The cause remains unknown, but is likely related to direct nerve contact with the prosthesis. Removal of the prosthesis did not to result in recovery. Inadequate soft tissue separating the condylar prosthesis from the nerve is the most likely contributing factor to facial nerve damage. In our series, facial nerve injury never occurred with type 3 reconstructions, likely because of the generous soft tissue and muscle bulk wrapped around the plate and prosthetic condyle. If a bony reconstruction is not concurrently performed, soft tissue interposition could be achieved with tissue from a vascularized soft tissue flap used, or from partial temporalis transposition flap secured around the neck of the condyle.
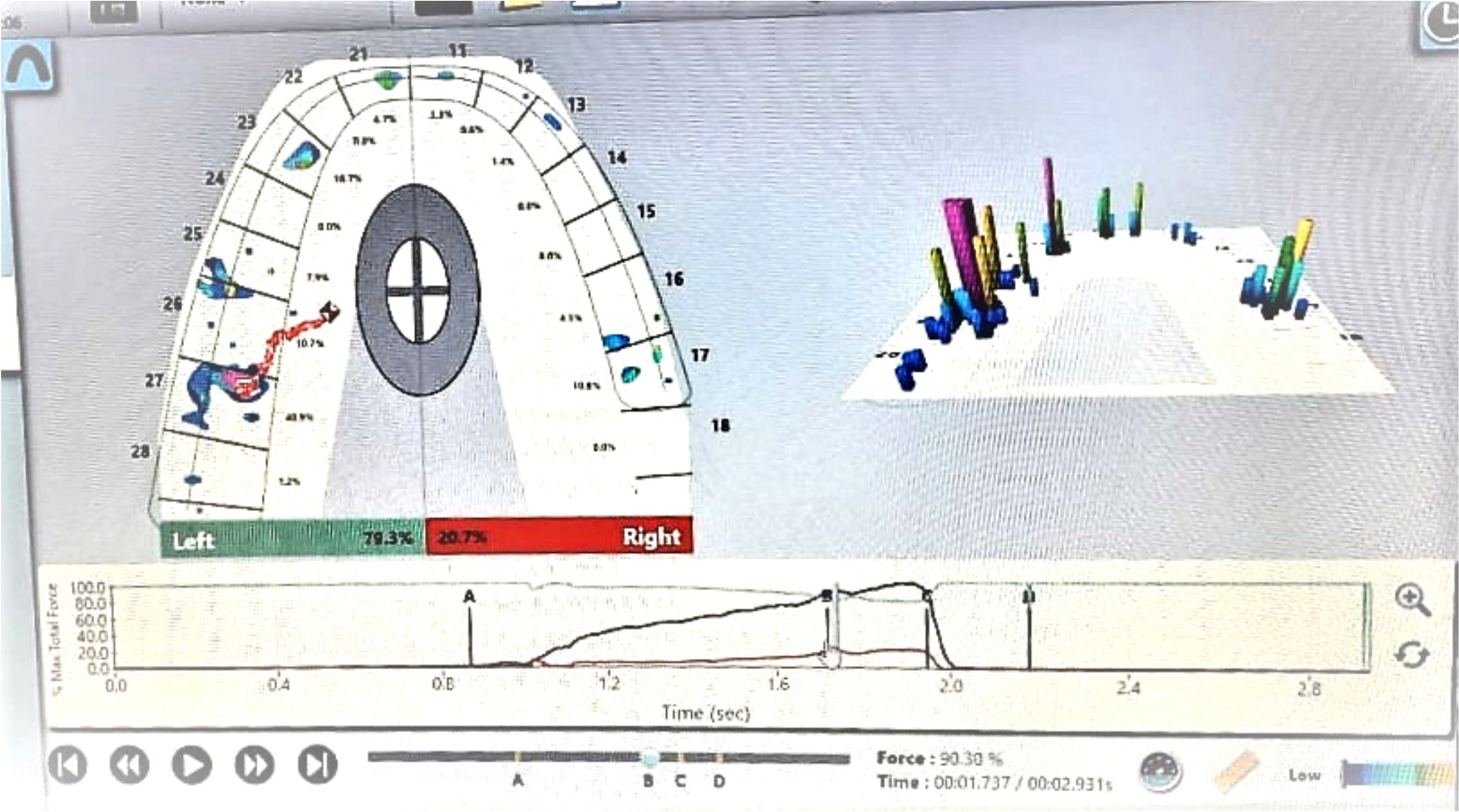
Functional outcomes in our cohort demonstrate good occlusal and oral intake outcomes. The results of the Functional Intraoral Glasgow score showed comparable results to fibula only reconstructions in patients with benign disease[16]. All patients maintained intelligible speech, and most were able to chew adequately. Chronic swallow dysfunction was secondary to post-operative radiotherapy. Patients who required removal of the condylar prosthesis had the worst functional outcomes. The following recommendations can be made from our experience to achieve good functional outcomes.
Where dental rehabilitation is considered, we recommend waiting for 12 months following reconstruction to allow for stabilisation of the anteroposterior and vertical position of the mandible prior to planning and insertion of implants.
Occlusion and condylar position can be controlled with the following:
Suspensory sutures or fascial sling from the reconstruction plate to the articular disk and residual joint tissue, or to the zygomatic arch.
For dentate patients, intermaxillary fixation intra-operatively and elastic support post-operatively for 6 weeks will guide a balanced post-operative occlusion.
Where pterygomasseteric sling muscles are preserved, resuspend the sling during closure, suturing the muscles to the plate or fibula.
The key limitation of this paper is the retrospective nature of the study, the heterogeneity of conditions included, and the small sample size. However, what differentiates this report from others is that it includes a large number of malignant cases, and it demonstrates the potential role of combined prosthetic condyles with microvascular reconstruction to achieve good functional outcomes in both malignant and benign cases. The authors, where possible, prefer autogenous reconstruction alone for disarticulation defects without a prosthetic condyle. However, we believe that the future of reconstruction of disarticulation defects may lie in the use of total joint reconstruction (fossa and condylar components), which has developed rapidly over the years for advanced internal derangement or arthritic conditions of the TMJ with evidence of long term success [22]. Acceptable results have been demonstrated with their use for mandibular disarticulation defects in benign disease [2, 10]. However, in the setting of malignant disease, there is a lack of evidence to demonstrate safety in the setting of radiotherapy, uncertainty regarding the positional stability after significant soft tissue resection, and significant time delays to design and production of a total joint prosthesis making it not suitable for malignant cases. Further development and more rapid CAD-CAM is required before total prosthetic joint replacement can be considered routine in malignant ablative mandibular defects.



Comments (0)