
Remember me


This is a prospective, double-blind, randomized placebo-controlled trial designed to assess whether therapy with PRF + ACS on the DRG compared to PRF + PhS reduces neuropathic pain and its consequences, in patients with persistent LLR .
In addition, this it to evaluate if the fact of adding ACS can give a greater advantage for the reduction of pain in these patients.
Taking into account that pulsed RDF is currently the interventional treatment with the best results to offer to patients with persistent chronic radiculalgia, it is the design of the study proposed to perform PRF therapy on the DRG for 8 min, 45 V of the root affected to all the patients included in the study. At the end of the PRF therapy, a 3-mL dose of ACS will be administered on the DRG to the patients of the experimental group and a 3-mL dose of 0.9% PhS will be administrated on the DRG to patients of the placebo group.
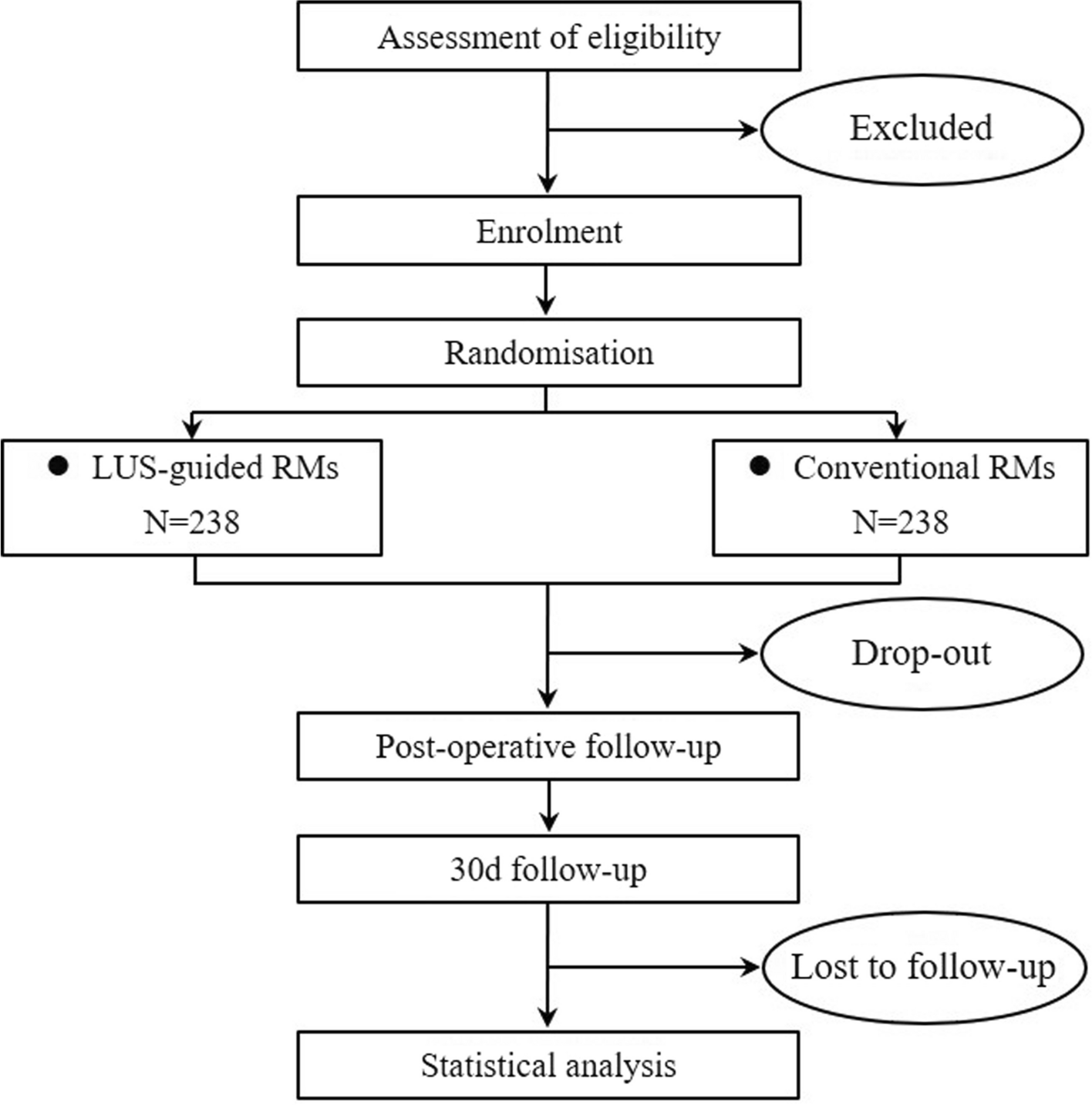
A schematic patient flow diagram is presented in Fig. 1 as recommended by SPIRIT [39].
Fig. 1 Setting
Setting The project will be carried out in the facilities of the pain unit of Department of Anaesthesiology, Resuscitation and Pain Treatment at the Dexeus University Hospital (DUH) in Barcelona. The principal investigator is the first responsible of all the project and its development.
Study populationThe study population proposed is 70 patients over 18 years of age, not illiterate, with radicular pain in the lower limb for more than 6 months. In addition, the symptomatic diagnosis screening criteria to confirm LLR will be used prior to the patient enrolment in the study. The inclusion and exclusion criteria are shown in Table 1.
Table 1 Inclusion and exclusion criteriaRecruitment and informed consentBoth the main investigator and the other doctors of the pain unit will proceed to recruit patients within their usual clinical practice and according to inclusion and exclusion criteria .
All the candidates will be informed in detail of the following information: the purpose of the study, interventions, benefits, possible risks, and corresponding responses. The patient accepts by signing the informed consent (IC) that he/she voluntarily participates in the study accepting that he/she may belong to the placebo or experimental group. They will sign the informed consent form voluntarily and will have the right to withdraw from the study at any time without any risk. The IC also includes a specific section on privacy consent and protection of personal data, according to the legal framework .
RandomizationRandomization will be carried out using a simple randomization based on an equiprobable algorithm. According to randomization algorithm, a three-digit numerical code list will be generated with the R statistical software. It contains the three-digit and the assignation group. This list will be given to the laboratory and to the pharmacy service of the DUH, so only these both will know which of the groups is placebo and which of the groups is experimental. Only the part of the lists containing the 70 three-digit numerical code (not the assignation group) will be given to the main investigator. For each recruited patient, the main investigator will assign consecutively a three-digit code number and give to the patient a document with his name and the three-digit numerical code. When the patient will go to the laboratory, it will know if the patient belongs to the experimental group or the placebo group and proceed to prepare the samples. The principal investigator and the patients will be blinded for the remaining.
Trial intervention and blindingTo comply with double-blind blinding, the following steps will be followed for the extraction and preparation of the ACS:
All patients will be scheduled 4 days before infiltration in the laboratory for blood collection and sample processing. Prior to extraction, patients will undergo the determinations based on the following documents: AEMPS REPORT/V1/23052013 and ROYAL DECREE 1088/2005. Given the laboratory will already know if the patient belongs to the experimental or placebo group, it will proceed to draw blood for the preparation of the ACS or not and store the syringes in the refrigerator at a temperature not exceeding – 18 °C.
All patients will undergo a blood draw for the preparation, or not, of the ACS, so they will not be able to know at any time which group they belong to. The syringes with the ACS or PhS samples are identical and sealed so that the main investigator will not be able to know to which group the patient belongs to. In addition, the way to evaluate the improvement or not of the pain will be through the self-assessment tests that the patient will answer individually at the control visits with what the main investigator will transcribe the results of the tests to the study database.
The day scheduled for infiltration, before performing the technique, adequate positioning of the patient, and proper monitoring in accordance with the protocol of the pain unit is mandatory. To perform the procedure, a transforaminal DRG approach technique will be performed under asepsis and antisepsis and under fluoroscopic vision. After checking the impedances (not higher than 450 ohms), the presence of sensory stimulation will be checked with a stimulation between 0.3 and 0.6 V and motor stimulation with a voltage at most double that is necessary to cause paresthesia. Finally, and once the injection of contrast is verified, PRF therapy will be carried out on the DRG (8 min, 45 V). Once the therapy is finished, the sample assigned to the patient will be injected.
Since most studies and clinical trials describe ACS therapy with 2 or 3 injections [31,32,33,34,35,36,37], separated in time by 7–15 days, the exact same procedure will be repeated 14 days after the first treatment.
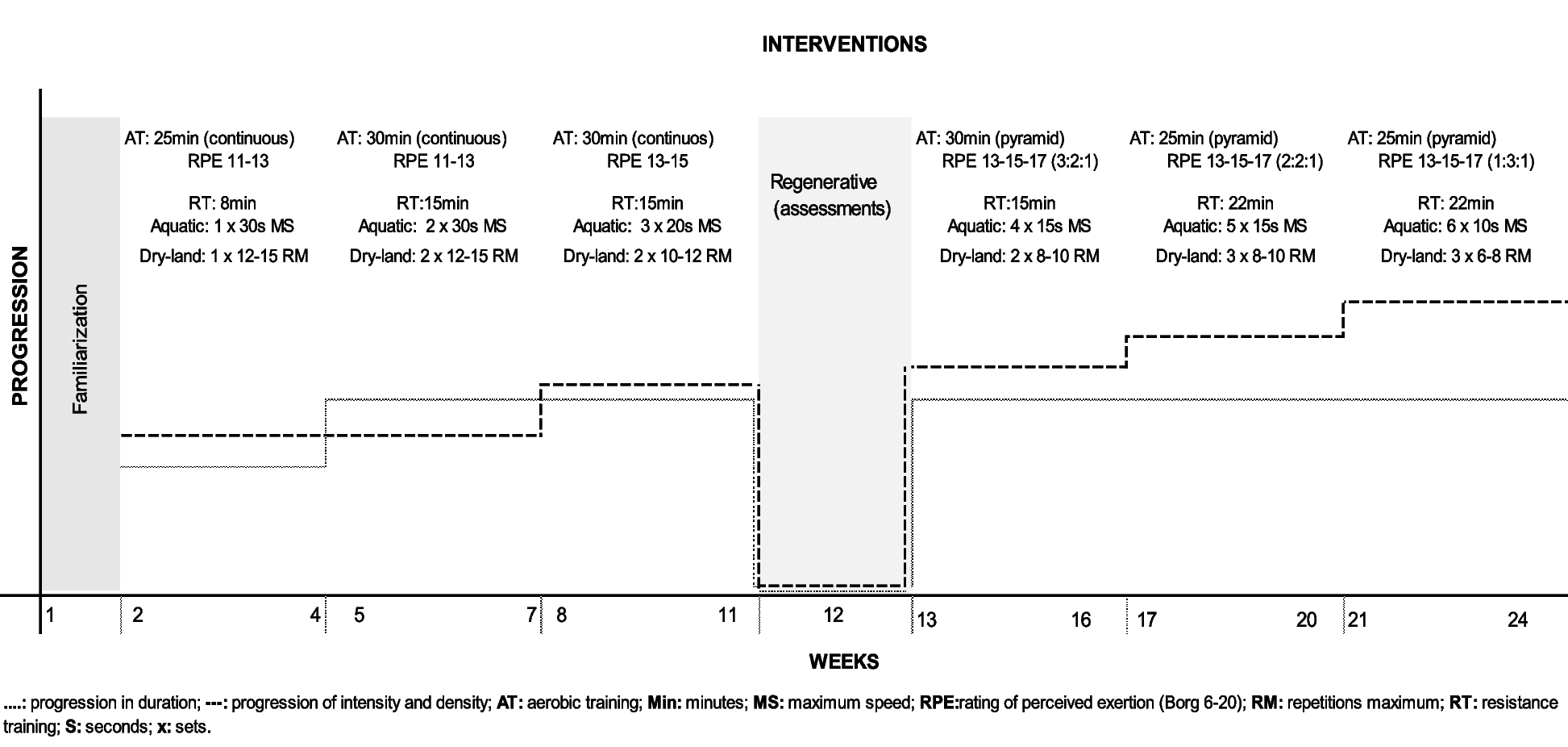
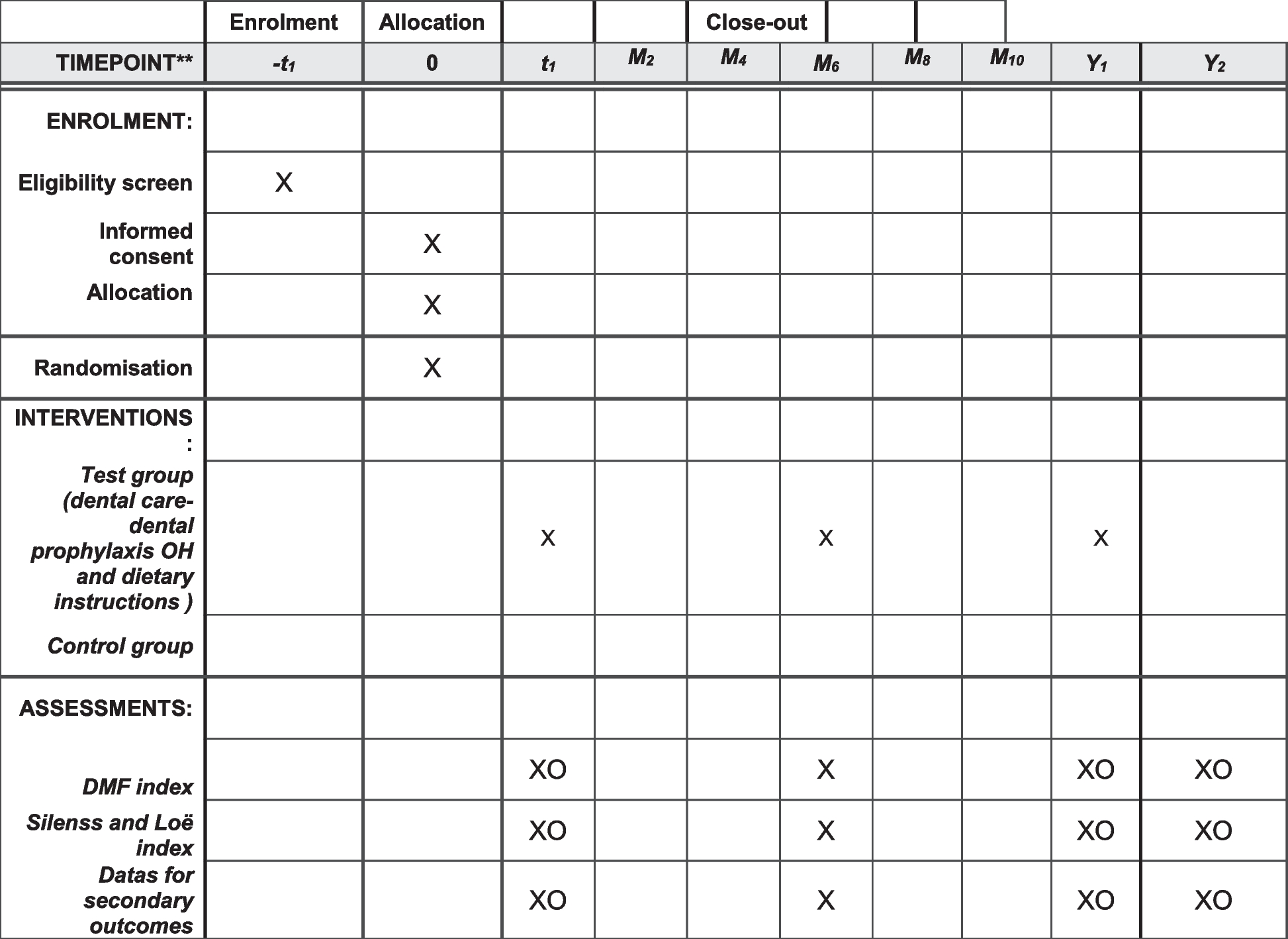
Time schedule of enrolment, interventions, assessments, and visits for participants is shown in Table 2 (timeline) and Table 3 .
Table 3 Schedule of assessments Outcome measures and follow-up Primary outcomeThe primary outcome will be level pain using Numeric Pain Rating Scale (NPRS). The NPRS is a segmented numeric version of the visual analog scale (VAS) in which a respondent selects a whole number (0–10 integers) that best reflects the intensity of his/her pain. A reduction of ≥ 2 points in NPRS is considered clinically significant pain relief [40]. This outcome will be measured at baseline at the moment of clinical interview and decision to recruitment and CI singed. This outcome will be measured again after the second intervention at 30 days, 3 months, 6 months, and 12 months after the intervention.
Secondary outcomesThe secondary outcomes include the following: Oswestry Low Back Pain Disability Scale (ODS) [41,42,43], Scale for Mood Assessment (MOAS) or Mood Rating Scale (MRS) [in Spanish original name Escala de Valoración del Estado de Ánimo (EVEA)] [44], Quality of Life (SF 12) test [45,46,47], and Douleur Neuropathique 4 questions (DN4) scale [48, 49]. They will be measured at baseline and after 1 month, 3 months, 6 months, and 12 months of the intervention (Additional file 1: Annex I).
The total duration of the randomized placebo-controlled study is expected to be 36 months, including 24 months for patient recruitment and 12 months for final patient follow-up.
Data collectionAt baseline, patient demographics and prior failed therapies will be documented, including frequency, duration, type, and compliance, as well as magnetic resonance imagining (MRI) and electromyography (EMG) diagnostic tests. Documentation of analgesic use for the treatment of LLR will include frequency, dosage, and duration. All baseline and post-procedural follow-up points will include reported outcomes documented through completing the NPRS, ODS, MOAS, SF-12, and DN4 questionnaires and documentation of narcotic and non-narcotic analgesic medication usage. Device and procedure-related adverse events and all serious adverse events will be documented throughout the study period (Table 3).
The data collected will be stored in locked cabinets, and only the main researcher will have access to this information. Data will be recruited in a computer spreadsheet with password protection to ensure confidentiality. To ensure no error, the spreadsheet will be monthly monitored and audited by a researcher who is blind to the participants’ group allocation and has no conflict of interest.
All patients who leave the study for any reason will no longer have their data collected.
Monitoring, safety, and quality controlThe primary safety endpoint is the incidence of device- and/or procedure-related adverse events, which will be compared statistically between the randomized groups using proportions of patients experiencing such an event. The endpoint will be met if this event rate is not significantly greater with ACS than with PhS. All study-related adverse events will be monitored and reported, including seriousness, severity, treatment, and relationship to the study device/procedure. Adverse events collected in this study will be determined by the mine investigator to be specifically related to the products or procedures used in the 2 treatment groups or one that is determined to be a serious adverse event .
To date, all published studies with ACS have shown high safety rates and no side effects for what ACS product itself represents. Even so, any intervention can lead to an adverse effect, so their monitoring will be an essential condition in this protocol .
Once the study has started, given that the inclusion of patients will be progressive over time as they are recruited, just in case there is a worsening of pain of more than 25% in more than 50% of the patients, the study would be reconsidered and the recruitment would be stopped to analyze the data and check if the worsening is in patients whom the ACS therapy was applied. If this were the case, the study would be definitively stopped and a report would be given to the laboratory. The author responsible for the study will carry out this audit if necessary. The main investigator together with the rest of the authors will make the decision to terminate the trial early .
Any other adverse effect as far as the interventions are concerned will be collected and analyzed (if necessary, the second intervention would be canceled, and the patient would be withdrawn from the study) .
The main investigator is the only person who will be in charge of follow-up with clinical interviews at 30 days, 3 months, 6 months, and 12 months. A schedule of visits will be established for each patient for their greater adherence to the study and not to delay follow-up. Apart from the following-up visit controls, the patients will provide from a telephone number of pain unit for any doubts, changing pain characteristics, or new interventions they will receive. In that way, it provides an improving of adherence to protocol of the study .
As far as the samples are concerned, both the laboratory responsible for the ACS and the pharmacy of DUH will have a record of the samples and their transport and temperature. Each sample will have a special label (study code, randomization number) and will be guarded by the pharmacy upon arrival from the laboratory and when it is withdrawn by the investigator on the day of its use for injection.
The study will be carried out in the facilities of the DUH, a document of suitability of the facilities signed by the head of the Department of Anaesthesiology and pain unit. In the same way, a commitment document is attached by the Hospital’s Pharmacy Department for the control and monitoring of the study. The main investigator will take the responsibility to monitoring of the study. She will coordinate with the people in the laboratory, pharmacy, and pain unit. There is also a thesis director who will meet monthly with the author responsible for the study and running the trial day-to-day to provide organizational support. In conclusion, since the day-to-day task falls on the main investigator, she will be responsible for any important protocol modification and technical aspects of the trial as well as data collection, outcome analyses, and results. She will be in charge of notifying the rest of authors as well as laboratory and pharmacy .
Sample sizeBased on the existing bibliography in relation to the treatment of pain by ACS treatment for other similar affections [32], it is estimated that accepting an alpha risk of 0.05 and a beta risk of 0.2 in a bilateral contrast, 35 subjects in the treatment group and 35 in the placebo group are needed to detect as statistically significant the difference between the proportion of patients with reduction pain of two points on the NPRS scale, which for the intervention group is expected to be 65%, and for the control group, it is expected to be 35%. A rate of loss to follow-up of 10% has been estimated.
Statistical analysisA descriptive analysis will be carried out for all the data collected. The normality of the data will be studied using the Kolmogorov–Smirnov and Shapiro–Wilk tests. For continuous quantitative variables, descriptions of central tendency and dispersion will be presented: mean and standard deviation respectively in case the variables follow a normal distribution or median and interquartile range for those variables that are not normally distributed. For categorical (qualitative) variables, frequencies and percentages will be presented. The main outcome (improvement > 2 points) will be tested using a generalized linear mixed model (GLMM). The GLMM model fit will include a between-subject factor and will also include a random effect for the time (baseline, 1st month, 3th month, 6th month, and 12th month) and the interaction between group and time variables. The inclusion of the interaction terms allows for a formal test between the groups over time. For the other variables, the mean effects of the interventions and the differences between groups and their respective 95% confidence intervals will be calculated using regression linear mixed models for repeated measures, which will incorporate terms for the treatment groups, time, and interaction terms. Treatment coefficients versus time interactions will be equivalent to the estimates of the differences between groups. All models will be adjusted for chance imbalances in outcome between groups at baseline. There will also be analyses of the covariates collected, including age, gender, and duration of symptoms. The analyses will follow the principles of intention to treat, and no interim analyses will be performed. No additional analysis will be performed. If a patient drops out of treatment, no additional outcome will be collected. The significance level will be set at 5%, and SPSS for Windows will be used for the statistical analysis.
The number of participants who complete the 12-month follow-up will be described by allocation; the study arms will be compared using chi-square tests and logistic regression to see if the attrition rate differs by arm and to compare baseline characteristics of participants who did and did not complete follow-up. Of those who complete follow-up, each variable will be examined for the presence of missing data, and if > 10% is observed for primary or secondary outcomes, then sensitivity analyses will be performed using complete case analysis or multiple imputation methods assuming data are missing at random (MAR). The MAR assumption indicates that the propensity for missingness does not depend on the unobserved outcome but rather is related to some other observed data.
Pain managementSpecial care different from the patient’s own reality will not be applied during the course of the trial; that is intended to resemble the real clinical applicability of the treatment as much as possible. In those patients who take opioid and non-opioid analgesics and/or neuromodulators as usual, medication will be documented in the baseline and follow-up controls. Likewise, if a patient undergoes any infiltration or surgical intervention in the same area affected by the trial intervention, this patient should be excluded from the clinical trial algorithm, and their data may not be used in the results from the date of surgery or infiltration .
Comments (0)